
Abstract
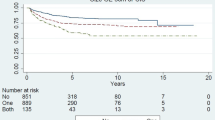
Objectives: To review our experience with early radical cystectomy in patients with T1G3 Transitional Cell Carcinoma of bladder (TCC). Patients and methods: Thirty patients, who underwent early radical cystectomy over a 10-year period for clinical stage T1G3 TCC bladder, were studied. Of these 21 (70%) had radical cystectomy without treatment with intravesical chemo/immunotherapy. The number of tumours, presence or absence of Carcinoma In-Situ (CIS) and the pathological stage of the cystectomy specimen were recorded in each patient. Disease specific survival was determined in the subgroups using Kaplan-Meier estimates. Results: Seventeen patients underwent radical surgery for a single tumour without concomitant CIS (Group A). The other 13 had multiple tumours with or without concomitant CIS or a single tumour with CIS (Group B). The disease was upstaged after cystectomy in 1 (6%) patient in Group A compared to 7 (55%) in Group B, (p = 0.009). Nine (53%) had pT0 disease in Group A compared to 0% in Group B, (p = 0.0017). The 5-year cancer specific survival rates were 92% in Group A and 82% in Group B. Conclusions: In patients with multiple T1G3 tumours with or without associated CIS, or in those with single T1G3 tumour with associated CIS the incidence of the disease being already muscle invasive at the time of clinical diagnosis is 55%. Early radical cystectomy should be advocated in this group. Conversely, for a single T1G3 tumour without associated CIS, conservative bladder preserving strategy with immuno-chemotherapy and close surveillance is justified.
Similar content being viewed by others


References
Freeman JA, Esrig D, Stein JP et al. Radical cystectomy for high-risk patients with superficial bladder cancer in the era of orthotopic urinary reconstruction. Cancer 1995; 76: 833–839.
Stein JP. Indications for early cystectomy. Semin Urol Oncol 2000; 18: 289–295.
Birch BRP, Harland SJ. The pT1G3 bladder tumour. Br J Urol 1989; 64: 109–111.
Sriprasad SI, Hopster D, Muir GH et al. The biological characteristics of pT1G3 bladder tumours are the same as muscle invasive cancer: a study of cell proliferation and molecular markers of aggressiveness. J Urol 2001; 165(5): supplement 192.
Brake M, Loertzer H, Horsch R et al. Recurrence and progression of stage T1, Grade 3 transitional cell carcinoma of the bladder following intravesical immunotherapy with Bacillus Calmette-Guerin. J Urol 2000; 163: 1697–1701.
Cookson MS, Herr HW, Zhang ZF et al. The treated natural history of high risk superficial bladder cancer: 15 year outcome J Urol 1997; 158: 62–66.
Montie JE, Wood DP Jr. The risk of radical cystectomy. Br J Urol 1989; 63: 483–486.
Rosario DJ, Becker M, Anderson JB. The changing pattern of mortality and morbidity from radical cystectomy. BJU Int 2000; 85: 427–430.
Stein JP, Lieskovsky G, Cote R, Groshen S, Feng AC, Boyd S, Skinner E, Bochner B, Thangathurai D, Mikhail M, Raghavan D, Skinner DG. Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1054 patients. Jr Clin Oncol 2001; 19: 666–675.
Pagano F, Bassi P, Galetti TP, Meneghini A, Milani C, Artibani W, Garbeglio A. Results of contemporary radical cystectomy for invasive bladder cancer: a clinico-pathologic study with emphasis on the inadequacy of the tumour, node and metastasis classification. J Urol 1991; 145: 45–50.
Malkowicz SB, Nichols P, Lieskovsky G et al. The role of radical cystectomy in the management of high grade superficial bladder cancer (Pa, P1, PIS and P2). J Urol 1990; 144: 641–644.
Amling CL, Thrasher JB, Frazier HA et al. Radical Cystectomy for stages Ta, Tis and T1 transitional cell carcinoma of the bladder. J Urol 1994; 151: 31–36.
Stockle M, Alken P, Engelmann U, Jacobi GH, Riedmiller H, Hohenfellner R. Radical cystectomy – often too late Eur Urol 1987; 13: 361–367.
Sobin LH, Wittekind Ch, eds. TNM Classification of Malignant Tumours, 6th edn. New York: Wiley, 2002.
Lamm DL, Blumenstein BA, Crissman JD et al. Maintenance bacillus Calmette-Guerin immunotherapy for recurrent TA, T1, and carcinoma in situ transitional cell carcinoma of the bladder: a randomized Southwest Oncology Group Study J Urol 2000; 163: 1124–1129.
Herr HW, Schwalb DM, Zhang ZF et al. Intravesical bacillus Calmette-Guerin therapy prevent tumour progression and death from superficial bladder cancer: ten year follow-up of a prospective randomized trial. J Clin Oncol 1995; 13: 1404–1408.
Abel PD, Hall RR, Williams G. Should pT1 transitional cell cancers of the bladder still be classified as superficial? Br J Urol 1988; 62: 235.
Herr HW. Tumour progression and survival in patients with T1G3 bladder tumours: 15-year outcome. Br J Urol 1997; 80: 762–765.
Vicente MP, Laguna D, Duarte F et al. Carcinoma in Situ as a prognostic factor for G3 pT1 bladder tumours. Br J Urol 1991; 68: 380–382.
Mufti GR, Virdi, JS, Hall MH. Long-term follow-up of intravesical epodyl therapy for superficial bladder cancer. Br J Urol 1990; 65: 32–35.
Dalbagni G, Genega E, Hashibe M et al. Cystectomy for bladder cancer: a contemporary series. J Urol 2001; 165: 1111–1116.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Masood, S., Sriprasad, S., Palmer, J. et al. T1G3 bladder cancer – Indications for early cystectomy. Int Urol Nephrol 36, 41–44 (2003). https://doi.org/10.1023/B:UROL.0000032688.37789.7c
Issue Date:
DOI: https://doi.org/10.1023/B:UROL.0000032688.37789.7c