
Abstract
Background: Detection and misclassification of rapidly conducted atrial fibrillation (AF) and marked sinus tachycardia by implantable cardioverter defibrillators (ICD) can result in the delivery of inappropriate therapies. Continuous atrial sensing may improve the differentiation between supraventricular and ventricular tachycardia. The present approach is to implant a separate atrial pacing lead connected to a dual-chamber defibrillator. We hypothesized that a free-floating single-pass defibrillation lead reliably senses the atrial electrical activity. The aim of the study was to assess during implantation the efficacy of a custom-built free-floating single-pass defibrillation lead and to record sinus rhythm (SR), induced AF, and atrial flutter (Afl).
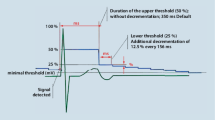
Methods: The free-floating single-pass defibrillation lead (Biotronik, Berlin, Germany) had an atrial bipole with 10 mm spacing and a distance between the atrial bipole and the electrode tip of 13.5, 15 or 17-cm. The lead was temporarily implanted in 15 patients during an ICD implantation. Fifteen seconds recordings were made during SR and after the induction of AF and Afl as well as during induced ventricular fibrillation. The amplitude and the time that the amplitude was less than 0.3 mV were assessed.
Results: The amplitude during SR (2.1 ± 1.4 mV) was significantly higher compared with the amplitudes for Afl (1.3 ± 0.5 mV; p < 0.02) and AF (0.7 ± 0.5 mV; p < 0.001). Low amplitudes were not observed during SR and rarely during Afl (1.6 ± 3.1%), but they were observed 19.9 ± 15.9% of the time during AF (p < 0.05). The correlation coefficients between SR and AF amplitudes were r = 0.25, between SR and Afl amplitudes r = 0.31, and between AF and Afl amplitudes r = 0.41. During the ventricular fibrillation conversion test 9 patients were in continuous SR. The P-wave amplitude before the induction of ventricular fibrillation was 2.1 ± 1.4 mV. The signal during ventricular fibrillation decreased to 1.1 ± 0.7 mV and increased immediately after the termination of ventricular fibrillation to 1.6 ± 0.8 mV.
Conclusions: The recorded unfiltered signals indicate that SR as well as AF and Afl can immediately be detected after the implantation of the new free-floating single-pass defibrillation lead. High signal amplitude during SR did not predict high amplitude during AF or Afl. During induced ventricular fibrillation the P-wave amplitude decreased intermittently.
Similar content being viewed by others


Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schuchert, A., Niehaus, M., Binner, L. et al. Feasibility of Atrial Sensing Via a Free-Floating Single-Pass Defibrillation Lead for Dual-Chamber Defibrillators. J Interv Card Electrophysiol 8, 209–214 (2003). https://doi.org/10.1023/A:1023921322671
Issue Date:
DOI: https://doi.org/10.1023/A:1023921322671