
Abstract
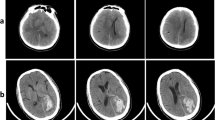
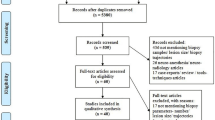
As little consensus exists on the postoperative care of patients undergoing stereotactic biopsy, we sought to establish a new algorithm for their postoperative management. First, we surveyed active members of the AANS/CNS Section on Tumors to determine national practice patterns for patients after stereotactic biopsy. Second, we retrospectively reviewed 84 consecutive stereotactic biopsy procedures at our institution to assess the potential benefit of routine computed tomography (CT) scanning and intensive care unit (ICU) monitoring. Finally, we prospectively applied this new algorithm in 54 patients to assess its validity. Of 629 surgeons, 263 (42%) responded; they were experienced neurosurgeons (mean 15 years in practice) who performed more than 10 stereotactic biopsies per year. Most surgeons (59%) routinely ordered postoperative CT scans, and the remainder ordered scans based on specific indications. Patients were transferred from the recovery room to a special care unit (47%), regular room (47%), or home (6%). In our retrospective review, 81 patients underwent 84 stereotactic biopsy procedures; 79 underwent postoperative CT scanning and all 81 were monitored overnight in the ICU. Among five (6%) patients who experienced intraoperative hemorrhage, two (2%) underwent craniotomy to control arterial bleeding. Three (4%) patients developed new neurological deficits, which occurred within 2 h of surgery. In both groups, CT scans were helpful in excluding hemorrhage that would require re-operation. In the remaining patients (90%), findings on routine postoperative CT did not alter patient management and ICU monitoring appeared unnecessary because neurological complications occurred within 2 h postoperatively. We confirmed these results in the prospective study of 54 patients undergoing stereotactic biopsy without routine postoperative CT scanning or ICU monitoring. In contrast with national practice patterns reported, we recommend that CT scanning and ICU monitoring be reserved for patients who have intraoperative hemorrhage or new deficits after surgery. All other patients can be monitored for 2 h in the recovery room and transferred to a regular hospital room without a postoperative CT scan.
Similar content being viewed by others

References
Apuzzo MLJ, Chandrasoma PT, Cohen D, Zee CS, Zelman V: Computed imaging stereotaxy. Experience and perspective related to 500 procedures applied to brain masses. Neurosurgery 20: 930–937, 1987
Apuzzo MLJ, Sabshin JK: Computed tomographic guidance stereotaxis in the management of intracranial mass lesions. Neurosurgery 12: 277–285, 1983
Bernstein M, Parrent AG: Complications of CT-guided stereotactic biopsy of intra-axial brain lesions. J Neurosurg 81: 165–168, 1994
Bouvier G, Couillard P, Leger SL, Lesage J, Rotent F, Beique RA: Stereotactic biopsy of cerebral space occupying lesions. Appl Neurophysiol 46: 227–230, 1983
Bullard DE: Role of stereotaxic biopsy in the management of patients with intracranial lesions. Neurol Clin 3: 817–830, 1985
Coffey RJ, Lunsford LD: Stereotactic surgery for mass lesions of the midbrain and pons. Neurosurgery 17: 12–18, 1985
Mundinger F: CT stereotactic biopsy for optimizing the therapy of intracranial processes. Acta Neurochir Suppl 3S: 70–74, 1985
Niizuma H, Otsuki T, Yonemitsu T, Kitahara M, Katakura R, Suzuki J: Experiences with CT-guided stereotaxic biopsies in 121 cases. Acta Neurochir Suppl 42: 157–160, 1988
Ostertag CB, Mennel HD, Kiessling M: Stereotactic biopsy of brain tumors. Surg Neurol 14: 275–283, 1980
Poza M, Perez-Espejo MA, Martinez-Lage JF, Esteban JA, Climent V, Sola J: Intracranial tumor biopsy - CT-guided stereotactic surgery. Appl Neurophysiol 48: 482–487, 1985
Ranjan A, Rajshekhar V, Joseph T, Chandy MJ, Chandi SM: Non-diagnostic CT-guided stereotactic biopsies in a series of 407 cases. Influence of CT morphology and operator experience. J Neurosurg 79: 839–844, 1993
Field M, Witham TF, Flickinger JC, Kondziolka D, Lunsford LD: Comprehensive assessment of hemorrhage risks and outcomes after stereotactic brain biopsy. J Neurosurg 94: 545–551, 2001
Kulkarni AV, Guha A, Lozano A, Bernstein M: Incidence of silent hemorrhage and delayed deterioration after stereotactic brain biopsy. J Neurosurg 89: 31–35, 1998
Bhardwaj RD, Bernstein M: Prospective feasibility study of outpatient stereotactic brain lesion biopsy. Neurosurgery 51: 358–364, 2002
Hall WA: The safety and efficacy of stereotactic biopsy for intracranial lesions. Cancer 82: 1749–1755, 1997
Kaakaji W, Barnett GH, Bernhard D, Warbel A, Valaitis K, Stamp S: Clinical and economic consequences of early discharge of patients following supratentorial stereotactic brain biopsy. J Neurosurg 94: 892–898, 2001
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Warnick, R.E., Longmore, L.M., Paul, C.A. et al. Postoperative management of patients after stereotactic biopsy: results of a survey of the AANS/CNS Section on Tumors and a single institution study. J Neurooncol 62, 289–296 (2003). https://doi.org/10.1023/A:1023315206736
Issue Date:
DOI: https://doi.org/10.1023/A:1023315206736