
Abstract
Purpose. Aerosolized cyclosporine (aCsA) has proven to be an effective therapy for refractory acute and chronic rejection in lung transplant (LTx) patients. The objective of this study is to evaluate the lung deposition and systemic absorption of aCsA after aerosolized cyclosporine administration in LTx patients in the immediate postoperative period.
Methods. Cyclosporine (CsA) was administered intravenously (1.0 mg/kg) to eight LTx patients, and multiple blood samples were collected over 24 h. At least 24 h later, aCsA (300 mg in propylene glycol) was administered to the same patients using nebulization and multiple blood samples were obtained again. Five patients had an additional inhalational gamma scintigraphy study with aCsA and 99MTc-labeled albumin to measure drug deposition.
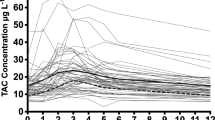
Results. Peak blood concentrations of CsA after aerosol administration ranged from 119-402 ng/ml, and concentrations at 24 h ranged from 9-48 ng/ml. The rate of decline in drug concentration in blood in the apparent elimination phase was notably slower after administration of aCsA than after IV infusion. Terminal disposition half life (t1/2 λz) values ranged from 4.1-9.9 h (mean 6.5 h) following IV administration and from 23.1 to 65.2 h (mean 40.7 h) following pulmonary administration, suggesting that drug absorption occurred throughout the 24-h sampling period following pulmonary administration. Deconvolution analysis indicated biphasic absorption of CsA from the lung in all patients, characterized by rapid initial absorption (absorption half-life 0.73 ± 0.38 h) over the first 4 to 6 h followed by slower, sustained absorption throughout the remainder of the sampling period (absorption half-life 16.2 ± 13.2 h). The absolute bioavailability of CsA after aerosol administration ranged from 5.4-11.2% (mean 8.2%) of the dose placed in the nebulizer. The total dose delivered to the lung estimated from scintigraphy ranged from 17.8-39.3 mg, and was in approximate agreement with the amount of drug absorbed, estimated using deconvolution. Essentially all drug deposited in the lungs was systemically absorbed.
Conclusions. This study documents that cyclosporine can be effectively delivered by aerosolization to the lung of transplant patients in the early postoperative period. Part of the cyclosporine deposited in the lung is absorbed rapidly into systemic circulation and a portion is absorbed slowly but completely over a prolonged period.
Similar content being viewed by others


REFERENCES
E. P. Trulock. Management of lung transplant rejection. Chest 103:1566-1576 (1993).
B. P. Griffith, R. L. Hardesty, J. M. Armitage, R. L. Kormos, G. C. Marrone, S. Duncan, I. Paradise, J. Dauber, and S. Yousem. Acute rejection of lung allografts with various immunosuppressive protocols. Ann. Thorac. Surg. 54:846-851 (1992).
I. Paradise, J. Dauber, S. Yousem, and B. P. Griffith. Airway obstruction and bronchiolitis obliterans after lung transplantation. Clin. Chest Med. 14:751-763 (1993).
S. Kesten, A. Maidenberg, T. Winton, and J. Maurer. Treatment of presumed and proven acute rejection following six months of lung transplant survival. Am. J. Respir. Crit. Care Med. 152:1321-1324 (1995).
A. T. Iacono, R. J. Keenan, S. R. Duncan, G. C. Smaldone, J. H. Dauber, I. L. Paradis, N. P. Ohori, W. F. Grgurich, G. J. Burckart, A. Zeevi, E. Delgado, T. G. O'Riordan, M. M. Zendarsky, S. A. Yousem, and B. P. Griffith. Aerosolized cyclosporine in lung recipients with refractory chronic rejection. Am. J. Respir. Crit. Care Med. 153:1451-1455 (1996).
A. T. Iacono, G. C. Smaldone, R. J. Keenan, P. Diot, J. H. Dauber, A. Zeevi, G. J. Burckart, and B. P. Griffith. Dose-related reversal of acute lung rejection by aerosolized cyclosporine. Am. J. Respir. Crit. Care Med. 155:1690-1698 (1997).
R. J. Keenan, A. T. Iacono, J. H. Dauber, A. Zeevi, S. Yousem, N. P. Ohori, G. J. Burchart, and B. P. Griffith. Treatment of refractory acute allograft rejection with aerosolized cyclosporine in lung transplant recipients. Ann. Thorac. Surg. 133:335-341 (1997).
T. G. O'Riordan, S. R. Duncan, G. J. Burckart, B. P. Griffith, and G. C. Smaldone. Production of an aerosol of cyclosporine as a prelude to clinical studies. J. Aerosol Med. 5:171-177 (1992).
T. G. O'Riordan, A. Iacono, R. J. Keenan, S. R. Duncan, G. J. Burckart, B. P. Griffith, and G. C. Smaldone. Delivery and distribution of aerosolized cyclosporine in lung allograft recipients. Am. J. Respir. Crit. Care Med. 151:516-521 (1995).
G. J. Burckart, R. J. Keenan, A. T. Iacono, and B. P. Griffith. Cyclosporine aerosol in lung transplantation. In S.A. Gruber, (ed.) Local Immunosuppression of Organ Transplants, R.G. Landes Company, Austin, Texas 1996 pp. 131-139.
S. Rohatagi, F. Calic, N. Harding, M.-L. Ozoux, J.-P. Bouriot, S. Kirkesseli, L. DeLeij, and B. K. Jensen. Pharmacokinetics, pharmacodynamics, and safety of inhaled cyclosporin A (ADI628) after single and repeated administration in healthy male and female subjects and asthmatic patients. J. Clin. Pharmacol. 40:1211-1226 (2000).
R. J. Ptachcinski, R. Venkataramanan, and G. J. Burckart. Clinical pharmacokinetics of cyclosporine. Clin. Pharmacokin. 11:107-132 (1986).
R. Kawau, K. Ochiau, A. de Fraissinette, K. Hoshiko, A. Nakashima, and N. Masuda. Pharmacokinetic assessment of pulmonary absorption and accumulation after inhalation of a cyclosporine derivative, IMM 125. Xenobio. Metabol. Dispos. 12:S104-S105 (1997).
S. M. McAllister, H. O. Alpar, Z. Teitelbaum, and D. B. Bennett. Do interactions with phospholipids contribute to the prolonged retention of polypeptides within the lung? Adv. Drug Deliv. Rev. 19:89-110 (1996).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Burckart, G.J., Smaldone, G.C., Eldon, M.A. et al. Lung Deposition and Pharmacokinetics of Cyclosporine After Aerosolization in Lung Transplant Patients. Pharm Res 20, 252–256 (2003). https://doi.org/10.1023/A:1022275222207
Issue Date:
DOI: https://doi.org/10.1023/A:1022275222207