
Abstract
Fabry disease is an X-linked recessive genetic disorder of glycosphingolipid metabolism, due to deficiency of the lysosomal enzymeα-galactosidase A. The disease is characterized by the progressive intracellular lysosomal accumulation of neutral glycosphingolipids throughout the body, including the cardiovascular system.
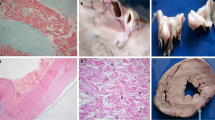
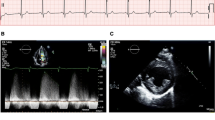
It has been reported that cardiac involvement could be the sole manifestation of the disease in some patients. Myocardial abnormalities are characterized mainly by left ventricular (LV) wall thickening without significant cavity dilatation, the most frequent abnormal structural pattern being concentric LV hypertrophy (LVH). In some patients the disease mimics a typical hypertrophic obstructive cardiomyopathy. According to our experience, systolic function is largely preserved in a large majority of affected individuals. In contrast, mild to moderate impairment of diastolic filling is a relatively common finding, representing probably the most important cause of dyspnoea in patients with Fabry disease. However, in a relatively large population of affected patients, severe diastolic dysfunction, typical of restrictive cardiomyopathy, was not found. Valvular structural abnormalities are frequent due to valvular infiltration. In several patients, hypertrophy of papillary muscles and/or systolic anterior motion of the mitral leaflets associated with LV outflow obstruction may aggravate the mitral valve dysfunction. We did not confirm the previously reported high prevalence of mitral valve prolapse. Valvular regurgitation seems to be relatively frequent but mostly non-significant. Electrocardiographic changes in Fabry disease are multiple and include at rioventricular (AV) conduction abnormalities (abbreviation of the P-R interval or AV blocks), signs of LVH and repolarization abnormalities. Our observations suggest that conduction defects and repolarization changes are present predominantly in subjects with LV structural abnormalities. Cardiac symptoms inpatients with Fabry disease include shortness of breath on effort (related to LV diastolic dysfunction), vasospastic and/or exertional angina pectoris (due to LVH, endothelial dysfunction and/or fixed coronary artery stenosis) and syncope (related to AV blocks or LV outflow obstruction). The extent of cardiac involvement, in particular LV mass assessment, could represent an ideal surrogate endpoint for evaluating the efficacy of specific therapies.
Similar content being viewed by others

REFERENCES
Bass JL, Shrivastava S, Grabowski GA, Desnick RJ, Moller JH (1980) The M-mode echocardiogram in Fabry's disease. Am Heart J 100(6 Pt 1): 807–812.
Becker AE, Schooorl R, Balk AG, van der Heide RM (1975) Cardiac manifestations of Fabry's disease. Report of a case with mitral insufficiency and electrocardiographic evidence of myocardial infarction. Am J Cardiol 36: 829–835.
Cantor WJ, Butany J, Iwanochko M, Liu P (1998a) Restrictive cardiomyopathy secondary to Fabry's disease. Circulation 98: 1457–1459.
Cantor WJ, Daly P, Ieuanochko M, Clarke JTR, Cusimano RL, Butany J (1998b) Cardiac transplantation for Fabry's disease. Can J Cardiol 14: 81–84.
Cohen IS, Fluri-Lundeen J, Wharton TP (1983) Two dimensional echocardiographic similarity of Fabry's disease to cardiac amyloidosis: a function of ultrastructural analogy. J Clin Ultrasound 11: 437–441.
Devereux RB, Koren MJ, de Simone G, Roman MJ, Laragh JH (1992) Left ventricular hypertrophy as a measure of preclinical hypertensive disease. Am J Hypertens 5: 175S-181S.
Efthimiou J, McLelland J, Betteridge DJ (1986) Short PR intervals and tachyarrhythmias in Fabry's disease. Postgrad Med J 62: 285–287.
Elleder M, Bradová V, Šmíd F, et al (1990) Cardiocyte storage and hypertrophy as a sole manifestation of Fabry's disease. Report on a case simulating hypertrophic non-obstructive cardiomyopathy. Virchows Arch A Pathol Anat Histopathol 417: 449.
Eng CM, Desnick RJ (1994) Molecular basis of Fabry disease. Mutations and polymorphisms in the human alpha-galactosidase A gene. Hum Mutat 3: 103–111.
Germain D, Poenaru L (1999) Fabry disease: identification of novel alpha-galactosidase A mutations and molecular carrier detection by use of fluorescent chemical cleavage of mismatches. Biochem Biophys Res Comm 257: 708–713.
Goldman ME, Cantor R, Schwartz MF, Baker M, Desnick RJ (1986) Echocardiographic abnormalities and disease severity in Fabry's disease. J Am Coll Cardiol 7: 1157–1161.
Hillsley RE, Hernandez E, Steenbergen C, Bashore TM, Harrison JK (1995) Inherited restrictive cardiomyopathy in a 74-year old woman. A case of Fabry's disease. Am Heart J 129: 199–202.
Ikari Y, Kuwako K, Yamaguchi T (1992) Fabry's disease with complete AV block: histological evidence of involvement of the conduction system. Br Heart J 68: 323–325.
Linhart A, Palecek T, Bultas J, et al (2000a) New insights in cardiac structural changes in patients with Fabry's disease. Am Heart J 139: 1101–1108.
Linhart A, Palecek T, Bultas J, et al (2000b) Endothelin-1 is associated with advanced clinical symptoms and end-organ involvement in patients with Fabry's disease. Eur Heart J 21: 492.
Matsui S, Murakami E, Takekoshi N, Nakatou H, Enyama H, Takeda F (1989) Myocardial tissue characterization by magnetic resonance imaging in Fabry's disease. Am Heart J 117: 472–474.
Mehta J, Tuna N, Moller JH, Desnick RJ (1978) Electrocardiographic and vectocardiographic observations in Fabry's disease. Adv Cardiol 21: 220–222.
Murata R, Takatsu H, Noda T, et al (1999) Fifteen-year follow up of a heterozygous Fabry's disease patient associated with pre-excitation syndrome. Intern Med 38: 476–481.
Nakao S, Takenaka T, Maeda M, et al (1995) An atypical variant of Fabry's disease in men with left ventricular hypertrophy. N Engl J Med 333: 288–293.
Pochis WT, Litzow JT, King BG, Kenny D (1994) Electrophysiologic findings in Fabry's disease with a short PR interval. Am J Cardiol 74: 203–204.
Rosenberg DM, Ferrans VJ, Fulmer JD, et al (1980) Chronic airflow obstruction in Fabry's disease. Am J Med 68: 898–904.
Roudebush CP, Foerster JM, Bing OHL (1973) The abbreviated PQ interval of Fabry's disease. N Engl J Med 289: 357–358.
Sakuraba H, Yanagawa Y, Igarashi T, et al (1986) Cardiovascular manifestations in Fabry's disease. A high incidence of mitral valve prolapse in hemizygotes and heterozygotes. Clin Genet 29: 276–283.
von Scheidt W, Eng CM, Fitzmaurice TF, et al (1991) An atypical variant of Fabry's disease with manifestations confined to the myocardium. N Engl J Med 324: 395–399.
Sheth KJ, Thomas JP (1982) Electrocardiograms in Fabry's disease. J Electrocardiol 15: 153–156.
Suzuki M, Goto T, Kato R, Yamauchi K, Hayashi H (1990) Combined atrioventricular block and sinus node dysfunction in Fabry's disease. Am Heart J 120: 438–440.
Tanaka H, Adachi K, Yamashita Y, Toshima H, Koga Y (1998) Four cases of Fabry's disease mimicking hypertrophic cardiomyopathy. J Cardiol 18: 705–718.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Linhart, A., Lubanda, JC., Palecek, T. et al. Cardiac manifestations in Fabry disease. J Inherit Metab Dis 24 (Suppl 2), 75–83 (2001). https://doi.org/10.1023/A:1012428009627
Issue Date:
DOI: https://doi.org/10.1023/A:1012428009627