
Abstract
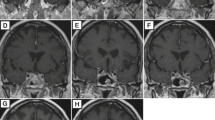
Pituitary gland is an uncommon site of a primary cancer. Of more than 600 cases of pituitary tumors seen at the KFSH&RC between 1975 to 1998 only 3 patients had primary pituitary cancer. We have previously reported a case of pituitary fibrosarcoma arising as a rare complication of external radiotherapy (ERT) for GH-secreting pituitary adenoma (PA) [1]. We report now 2 cases of ACTH-producing primary pituitary carcinoma (ACTH-PPC); their follow-up data provide information on the natural history of this cancer. Patient #1; a 46 year old lady with Cushing's disease (CD) presented with an enlarged right cervical lymph node (LN) 2 years after having undergone a partial hypophysectomy through transsphenoidal surgery (PHYPX/TSS) and ERT for an invasive pituitary tumor. Patient #2; a 26 year old man presented with CD and underwent bilateral adrenalectomy (ADx) and pituitary ERT. Thirty-nine months later he developed Nelson's syndrome and a PHYPX/TSS was performed. Incidentally discovered hepatic metastases in this patient and an excisional biopsy of the LN in patient #1 showed histological features very similar to the pituitary tumor, and they stained strongly positive for ACTH. Perinuclear spherical hyalinized cytoplasmic inclusions were seen in the LN biopsy that corresponded to bundles of type 1 microfilaments (specific for pituitary ACTH-producing cells) seen by electron microscopy. A whole body 18-Fluoro-2-Deoxy-D-Glucose positron emission (FDG-PET) scanning, showed an intense uptake in the neck mass. A trial of octreotide did not change the exceedingly high levels of ACTH in patient #2, further supporting the diagnosis of ACTH-PPC. The clinical course of 102 months prior to his demise showed continued progression of the primary and the metastatic tumor. Patient #1, is alive at 15 months follow-up; hypercortisolemia is controlled using ketoconazole. ACTH-PPC should be entertained in a patient with CD presenting with persistent cervical lymphadenopathy. The clinical course in our patients suggests that the emergence of PC may involve a proliferative continuum from a pre-existing PA to an invasive tumor, culminating in a carcinoma. Adjunctive events such as ERT/ADx may predispose to the evolution of PC in genetically susceptible individuals. Because ERT is an effective treatment for PA its use will continue; it is important to be aware of the possible complication of primary pituitary carcinoma.
Similar content being viewed by others

References
Ahmed M, Kanaan I, Rifai A, Tulbah A, Ghannam N. Clinical case seminar: An unusual treatment-related complication in a patient with growth hormone secreting pituitary tumor. J Clin Endocrinol Metab 1997;82:2816–2820.
Kaiser FE, Orth DN, Kiyoshi M, Oppenheimer JH. A pituitary parasellar tumor with extracranial metastases and high, partially reversible levels of adrenocorticotropin and related peptides. J Clin Endocrinol Metab 1983;57:649–653.
Pernicone PJ, Scheithauer BW, Sebo TJ, Kovacs KT, Hovarth E, Young WF, Lloyd RV, Davis DH, Guthrie BL, Schoene WC. Pituitary carcinoma: A clinicopathological study of 15 cases. Cancer 1997;79:804–812.
Kaltas GA, Grossman AB. Malignant pituitary tumors. Pituitary 1998;1:69–81.
Carthwright DM, Miller TR, Nasr AJ. Fine-needle aspiration biopsy of pituitary carcinoma with cervical lymph node metastases: A report of two cases and review of the literature. Diagn Cytopathol 1994;11:68–73.
Fachnie JD, Zafar MS, Mellinger RC, Chason JL, Kahkonen DM. Pituitary carcinoma mimics ectopic adrenocorticotropin syndrome. J Clin Endocrionol Metab 1980;50:1062–1065.
Stewart PM, Carey MP, Graham CT, Wright AD, London DR. Growth hormone secreting pituitary carcinoma: A case report and literature review. Clin Endocrinol 1992;37:189–194.
Wilson DF. Pituitary carcinoma occurring as middle ear tumor. Otolaryngol Head Neck Surg 1982;90(5):665–666.
Yamashita S, Izumi M, Nagataki S. Acromegaly and pituitary carcinoma. Ann Intern Med 1992;117:1057.
Lubke D, Wolfgang S, Carcinomas of the pituitary; de~nition and review of the literature. Gen Diagn Pathol 1995; 141:81–92.
Mount Castle RB, Roof BS, Mayfield RK, Morders DB, Sagel J, Biggs PL, Rawe SE. Case Report: Pituitary adrenocarcinoma in an acromegalic patient. Response to bromocriptine and pituitary testing. A review of the literature on 36 cases of pituitary carcinoma. Am J Med Sci 1989; 298:109–118.
Nawata H, Higuchi K, Ikuyms S, Kato K, Ibayashi J, Mimura K, Sueishi K, Zingami H, Imura H. Corticotropin-releasing hormone and adrenocorticotropin-producing pituitary carcinoma with metastases to the liver and lung in a patient with Cushing's disease. J Clin Endocrinol Metab 1990;71:1068–1073.
Jamjoom A, Moss T, Coakham H, Jamjoom AZ, Anthony P. Cervical lymph nodes metastases from a pituitary carcinoma. Br J Neurosurg 1994;8:87–92.
Luzi P, Miracco C, Lio R, Malandrini A, Piovani S, Venezia SG, Tosi P. Endocrine inactive pituitary carcinoma metastasizing to cervical lymph nodes: A Case Report. Hum Pathol 1987;8:90–92.
Nelson DH, Meakin JW, Dealy JB, Matson DD, Emerson K, Thorn GW. ACTH-producing tumor of the pituitary gland. N Engl J Med 1958;259:161.
Jenkins PJ, Trainer PJ, Plowman PN, Shand WS, Grossman AB, Wass JAH, Besser GM. The long-term outcome after adrenalectomy and prophylactic radiotherapy in adrenocorticotropin-dependent Cushing's syndrome. J Clin Endocrinol Metab 1994;79:165–171.
Manolas KJ, Farmer HM, Wilson HK, Kennedy L, Joplin GF, Montgomery DAD, Kennedy TL, Welbourn RB. The pituitary before and after adrenalectomy for Cushing's syndrome. World J Surg 1984;8:374–387.
Burch WM. Cushing's disease. Arch Intern Med 1985; 145:1106–1111.
Sarne DH. Medical treatment of pituitary tumors and hypersecretory states. In: Becker KL, ed. Principles and Practice of Endocrinology and Metabolism. J.B. Lippincott Co., 1990: 206.
Pei L, Melmed S, Scheithauer B, Kovacs K, Prager D. H-ras mutations in human pituitary carcinoma metastases. J Clin Endocrinal Metab 1994;78:842–846.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Ahmed, M., Kanaan, I., Alarifi, A. et al. ACTH-Producing Pituitary Cancer: Experience at the King Faisal Specialist Hospital & Research Centre. Pituitary 3, 105–112 (2000). https://doi.org/10.1023/A:1009957824871
Issue Date:
DOI: https://doi.org/10.1023/A:1009957824871