
Abstract
The aim of this study was to identify the optimal position on the chest wall to place an implant able cardioverter defibrillator in a two-electrode system, consisting of a right ventricular electrode and active can.
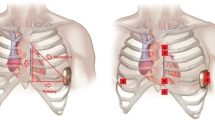
Methods and Results: Defibrillation thresholds (DFT) were measured in 10 anaesthetised pigs (weight 33–45kg). An Angeflex™ lead was introduced transvenously to the right ventricular apex. The test-can (43cc) was implanted submuscularly in each of four locations: left pectoral (LP), right pectoral (RP), left lateral (LL) and apex (A). The sequence in which the four locations were tested was randomized. Ventricular fibrillation (VF) was induced using 60Hz alternating current. Rectangular biphasic shocks were delivered 10 seconds after VF induction. The DFT was measured using a modified four-reversal binary search. The results of the four configurations were: LP, 14.6± 4.0J; RP, 18.8± 4.2J; LL, 14.7± 4.1J; A, 14.9± 3.1J. Repeated measures analysis of variance showed that the DFT of RP was significantly higher than LP, LL and A (p < 0.05).
Conclusions: Implanting an active can in the RP position increases the DFT by 29% compared to LP, LL and A sites. The can position on the left thorax does not appear to have a significant influence on DFT.
Similar content being viewed by others


References
Gill RM, Sweeney RJ, Reid PR. The defibrillation threshold: a comparison of anesthetics and measurement methods. Pacing. Clin. Electrophysiol 1993;16:708–714.
Heil JE, Lin Y, Derfus DL, Lang DJ. Impact of ICD electrode position on transvenous defibrillation thresholds. (abstract). Pacing. Clin. Electrophysiol 1998;18(4):873.
Saksena S, DeGroot P, Krol RB, Raju R, Mathew P, Mehra R. Low-energy endocardial defibrillation using an axillary or a pectoral thoracic electrode location. Circulation 1998;88:2655–2660.
Natale A, Sra J, Geiger MJ, Newby K, Akhtar M, Pacifico A. Right side implant of the unipolar single lead defibrillation system. Pacing. Clin. Electrophysiol 1997;20:1910–1912.
Jensen SM, Pietersen A, Chen X. Implantation of active can implantable defibrillators in the right pectoral position. Pacing. Clin. Electrophysiol 1998; 21:476–477.
Epstein AE, Kay GN, Plumb VJ, Voshage-Stahl L, Hull ML. Elevated defibrillation threshold when right-sided venous access is used for nonthoracotomy implantable defibrillator lead implantation. The Endotak Investigators. J Cardiovasc Electrophysiol 1995; 6:979–986.
Flaker GC, Tummala R, Wilson J. Comparison of right-and left-sided pectoral implantation parameters with the Jewel active can cardiodefibrillator. The World Wide Jewel Investigators. Pacing. Clin. Electrophysiol 1998;61:447–451.
Chen PS, Wolf PD, Claydon FJ, et al. The potential gradient field created by epicardial defibrillation electrodes in dogs. Circulation 1986;74:626–636.
Tang AS, Wolf PD, Afework Y, Smith WM, Ideker RE. Three-dimensional potential gradient fields generated by intracardiac catheter and cutaneous patch electrodes. Circulation 1992;85:1857–1864.
Gold JH, Schuder JC, Stoeckle H. Ventricular defibrillation with myocardial electrodes in the dog, calf, pony, and pig. Med Instrum 1980;14:19–22.
Crick SJ, Sheppard MN, Ho SY, Gebstein L, Anderson RH. Anatomy of the pig heart: comparisons with normal human cardiac structure. J Anat. 1998;1939:105–119.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Roberts, P.R., Allen, S., Betts, T. et al. Increased Defibrillation Threshold with Right-sided Active Pectoral Can. J Interv Card Electrophysiol 4, 245–249 (2000). https://doi.org/10.1023/A:1009882016469
Issue Date:
DOI: https://doi.org/10.1023/A:1009882016469