
Abstract
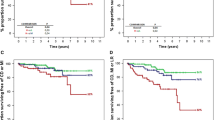
Background. Thrombolysis has reduced early and longterm mortality by about 20%; sometimes, however, there is a re-occlusion of the infarct related artery or an unsuccessful thrombolysis. In these situations, there is a possible increase in detrimental events in the follow-up. Objectives. The aim of the study was to compare the prognostic value of dobutamine echocardiography (DET) and ECG exercise test (EET)in pts submitted to thrombolysis. Methods. One hundred and fifty-one pts, with acute uncomplicated myocardial infarction, were enrolled. The pts were able to perform EET and had a sufficient echocardiographic window; 58 had anterior myocardial infarction (38%), 79 had inferior (52%), 2 had lateral (1%), 12 had non-Q (8%). EET was performed with an initial load of 25 Watt, and thereafter, 25 W every two minutes. DET was performed with step-wise infusion every three minutes (5, 10, 20, 30 and 40 mcg/kg/min.). If the target heart rate was not reached, a further dose of 40 mcg/kg/min. together with atropine 0.25-1 mg was administered, in the absence of signs and symptoms of ischemia. Results. During a mean (± SD) follow-up period of 8 ± 4.5 months (range 1–23), 16 spontaneous events happened (4 deaths, 5 non-fatal re-infarctions, 7 unstable angina). One-hundred and three EET (68%) were negative for ongoing ischaemia, while 48 were positive, 79 DET (52%) were negative for ongoing ischaemia and 72 were positive (48%). Statistical results: DET and EET had a sensitivity of 41% and 54%, a specificity of 57% and 74%, a positive predictive value of 7% and 14%, a negative predictive value of 91% and 95%, an accuracy of 56% and 73%. Kaplan-Maier survival curves demonstrated that patients with Peak Wall motion > 1.8 and EET score > 3, had the higher risk of spontaneous events. Conclusion. A few spontaneous events happened in the follow-up. These data demonstrate that patients treated with thrombolysis are not at high risk of spontaneous events. DET and EET, therefore, have had a high negative predictive value. For this reason, we can conclude that pts with negative tests can be considered at low risk and do not need any further investigations.
Similar content being viewed by others

References
Simoons ML, Vos J, Tijssen JGP, Vermeer F, et al. Longterm benefit of early thrombolytic therapy in patients with acute myocardial infarction: 5 year follow up of a trial conducted bythe interuniversity Cardiology institute of the Netherlands. J Am Coll Cardiol 1989; 14: 1609-1615.
The GUSTO angiographic investigators. The effects of tissue plasminogen activator, streptochinase or both on coronary artery patenty, ventricular function and survival after acute myocardial infarction. N England J Med 1993; 329: 1615-22.
White HJ, French JK, Hamer AW, Brown MA, Williams BF, Ormiston JA, Cross DB. Frequent re-occlusion of patient infarct related arteries between 4 weeks and 1 Year: effects of antiplatelet therapy. J Am Coll Card 1995; 25: 218-33.
Schaer DH, Ross AM, Wassermann AG. Reifarction, recurrent angina and re-occlusion after thrombolytic therapy. Circulation 1987; 76 suppl. II: 57-62.
Mejier A, Verhengt WF, Van Eenige MJ, et al. Left ventricular function at 3 months after successful thrombolysis. Impact of re-occlusion without re-infarction on ejection fraction, regional function and remodelling. Circulation 1994; 90: 1706-1714.
Kulick DL, Shahbudin H, Rahimtoola MB. Risk stratification in survivors of acute myocardial infarction: routine cardiac catheterization and angiography is a reasonable approach in most patients. Am Heart J 91: 642-651.
Miller TD, Christian T, Taliercio CP, Zinsmeier AR, Gibbons RJ. Severe exercise-induced ischemia does not identify high risk patients with normal left ventricular function and one-two vessel coronary artery disease. J Am Coll Cardiol 1994; 23: 219-224.
Bigger JT Jr, Heller CA, Wenger FM. Risk stratification after acute myocardial infarction. Am J Cardiol 1978; 42: 202-210.
The Multicenter Postinfarction Research Group. Risk stratification and survival after acute myocardial infarction. N Engl J N Med 1983; 309: 331-336.
Volpi A, De Vita C, Franzosi MG, Geraci E, Maggioni AP, Mauri F, Negri E, Santoro E, Tavazzi L, Tognoni G. Determinants of 6-month mortality in survivors of myocardial infarction after thrombolysis. Results of Gissi-2 data base. Circulation 1993; 88: 416-429.
Arnold AER, Simoons ML, Detry JMR, Von Essen R, Vande Werf F, Deckers JW, Lubsen J, Verstraete M. For the European Cooperative Study Group. Prediction of mortality following hospital discharge after thrombolysis in acute myocardial infarction: is there a need for coronary angiography? Eur Heart J 1993; 14: 3016-315.
Feit F, Mueller HS, Braunwald E, Ross R, Hodges M, Herman MV, Knatterud GL, and the Timi Research Group. Thrombolysis in myocardial infarction (TIMI)phase 2 trial outcome comparison of a conservative strategy in community versus tertiary hospitals. J Am Coll Cardiol 1991; 16: 1529-1534.32
The TIMI Study Group: comparison of invasive and conservative strategies after treatment with intravenous tissue plasminogen activator in acute myocardial infarction: results of the Thrombolysis in Myocardial Infarction (TIMI) Phase II Trial. N Engl J Med 1989; 320: 618.
Gibson RS, Watson DD, Craddock GB, Crampton RS, Kaiser DL, Denny MJ, Beller G. Prediction of cardiac events after uncomplicated myocardfial infarction: a prospective study comparing predischarge exercise thallium 201 scintigraphy and coronary angiography. Circulation 1983; 68: 321-336.
Villella A, Maggioni AP, Villella M, Giordano A, Turazza FM, Santoro E, Franzosi MG, on behalf of Gissi2 Investigators. Prognostic significance of maximal exercise testing after myocardial infarction treated with thrombolitic agents: the Gissi 2 data base. Lancet 1995; 346: 523-529.
Bolognese L, Sarasso G, Aralda D, Bongo AS, Rossi L, Rossi P. High dose dipyridamole echocardiography early after acute myocardial infarction:correlation with exercise testing and coronary angiography. J Am Coll Cardiol 1989; 14: 357-363.
Smart SC, Sawada SG, Ryan T, Segar SD, Bourdillon PDV, Feigenbhaum H. Dobutamine echocardiography identifies residual stenosis and multivessel disease after thrombolysis in myocardial infarction. J Am Coll Cardiol 1991; 17 (supp.): 277A.
Moss AJ, Benhorin J. Prognosis and management after a first myocardial infarction. N Engl J Med 1990; 322: 743-753.
Bigi R, Occhi G, Fiorentini C, Partesana N, Bandini P, Sponzilli C, Inglese L. Dobutamine stress echocardiography for the identification of multivessel disease after acute myocardial infarction: the importance of test end-point. Int J Cardiol 1995; 50: 51-60.
Picano E, Landi P, Bolognese L, Chiaranda' G, Chiarella F, Seveso G, Sclavo MG, Gandolfo N, Previtali M, Orlandini A, Margaria F, Pirelli S, Magaya O, Minardi G, Bianchi F, Marini C, Raciti M, Michelassi C, Severi S, Distante A, on behalf of the Epic study group. The prognostic value of dipyridamole-echocardiography early after uncomplicated infarction: a large scale multicenter trial. Am J Med 1993; 95: 608-618.
Chiarella F., Domenicucci S, Bellotti P, Bellone P, Scarsi G., Vecchio C., In hospital prognostic value of dipyridamole echocardiographic test performed three days after acute myocardial infarction: feasibility, tollerability, safety and in hospital prognostic value. Eur Heart J 1994; 15: 842-850.
Mazeika PK, Nadazdin A, Oakley CM. Dobutamine stress echocardiography for detection and assessment of coronary artery disease. J Am Coll Cardiol 1992; 19: 1203-1211.
Theroux P, Waters DD, Halphen C, Debaisieux JC, Mizgala HF. Prognostic value of exercise testing soon after myocardial infarction. N Engl J Med 1989; 30: 341-352.
Van Daele M, Mc Neill AJ, Fioretti PM, Salustri A, Pozzoli M, El Said M, Reijs A, Mc Falls E, Slagboom T, Roelandt J. Prognostic value of dipyridamole sestamibi single-photon emission computed tomography and dipyridamole stress echocardiography for new cardiac events after an uncomplicated myocardial infarction. J Am Soc Echocardiogr 1994; 7: 370-380.
Previtali M, Poli A, Lanzarini L, Fetiveau R, Mussini A, Ferrario M.. Dobutamine stress echocardiography for assessment of myocardial viability and ischemia in acute myocardial infarction treated with thrombolysis. Am J Cardiol 1993; 72: 124-130.
Neskovic An, Popovic Ad, Babic R, Marinkovic J, Obradovic V. Positive high dose dipyridamole echocardiography test after acute myocardial infarction is an excellent predictor of cardiac events. Am Heart J 1995; 129: 31-9.
Miller Td, Gersh BJ, Christian Tf, Bailey KR, Gibbons RJ. Limited prognostic value of thallium 201 exercise treadmill testing early after myocardial infarction in patients treated with thrombolysis. Am Heart J 1995; 130: 259-66.
Predictors of nonfatal reinfarction in survivors of myocardial infarction after thrombolysis Results of the Gruppo Italiano per lo studio della sopravvivenza nell'infarto del miocardico (GISSI 2) data base. Volpi A, De Vita C, Franzosi MG, Geraci E, Maggioni AP, Mauri F, Negri E, Santoro E, Tavazzi L, Tognoni G.: J Am Coll Cardiol 1994.
Rajdeep S, Khattar SK, Basu, Usha RR, Senior A, Lahiri. Prognostic value of predischarge exercise testing, ejection fraction, and ventricular ectopic activity an acute myocardial infarction treated with streptochinase. Am J Cardiol 1996; 78: 136-141.
De Feyter PJ, Van Eenige MJ, Dighton Dh, Visser FC, De Jong J, Roos JP. Prognostic value of exercise testing, coronary angiography, and left ventricular 6-8 weeks, after myocardial infarction. Circulation 1982; 66: 527-536.
Galati A, Coletta C, Ricci R, Sestili A, Aspromonte A, Fera MS, Re F, Ceci V. Valore prognostico del test ecodobutamina in 152 pazienti affetti da recente infarto del miocardio. Cardiovasc Imag 1996; 8: 209.
Coletta C, Galati A, Greco G, Burattini M, Ricci R, Carunchio A, Fera MS, Bordi L, Ceci V. Prognostic value of high dose dipyridamole echocardiography in patients with chronic coronary artery disease and preserved left ventricular function. J Am Coll Card 1995; 26: 887-94.
Fioretti P, Brower R, Simoons M, et al. Prediction of mortality during the first year after the acute myocardial infarction from clinical variables and stress test at hospital discharge Am J Cardiol 1985; 55: 1313-8.
Boccanelli A, Piazza V, Greco C, Zanchi E, Cecchetti C, Pontillo D, Pellanda JJ, Risa A, Baragli D, Prati PL. Valore diagnostico e sicurezza del test Eco-Dobutamina nella diagnosi di coronaropatia. Giorn Ital di Cardiol 1993; 23: 19-29.
Ricci R, Galati A, Coletta C, Greco G, Bordi L, Lumia F, Ceci V. Valore prognostico del test ecodobutamina in pazienti con cardiopatia ischemica: confronto con il test da sforzo. Giorn Ital di Card 1996; 26: 187-199.
Sicari R, Picano E, Landi P, et al. Prognostic value of Dobutamine-Atropine Stress Echocardiography early after acute myocardial infarction. J Am Coll Card 1997; 29: 254-60.
Shiller NB, Shah PM, Crawford M, et al. Reccomendations for quantitation of the left ventricle by two-dimensional echocardiography. (American Society of Echocardiography Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms). J Am Coll Cardiol 1995; 26: 26-32.
Greco CA, Salustri A, Seccareccia F, Ciavatti M, Biferali F, Valtorta C, Guzzardi G, Falcone M, Palamara A. Prognostic value of dobutamine echocardiography early after uncomplicated acute myocardial infarction: a comparison with exercise electrocardiography. J Am Coll Cardiol 1997; 29: 261-7.
Carlos ME, Smart SC, Wynsen JC, Sagar KB. Dobutamine stress echocardiography for risk stratification after myocardial infarction. Circulation 1997; 95: 1402-1410.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Galati, A., Bigis, R., Coletta, C. et al. Multicenter trial on prognostic value of inducible ischaemia, assessed by dobutamine stress echocardiography and exercise electrocardiography test, in patients with uncomplicated myocardial infarction, treated with thrombolytic therapy. Int J Cardiovasc Imaging 14, 155–162 (1998). https://doi.org/10.1023/A:1006061101594
Issue Date:
DOI: https://doi.org/10.1023/A:1006061101594