
Abstract
Study Design
Retrospective case series.
Objectives
To describe the indications and outcomes of cervical fixation using modern instrumentation in a case series of pediatric Down syndrome (DS) patients.
Summary of Background Data
Cervical instability is the major cervical spine concern in children with DS. Although fixation techniques have advanced over the past quarter-century, the outcome of fixation with modern instrumentation for upper cervical instability in DS patients has not been thoroughly investigated.
Methods
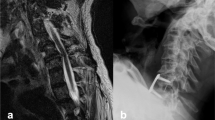
We searched the orthopedic database at our institution for patients with a diagnosis of DS who had undergone a cervical spine fusion between 2006 and 2017. Patient demographics, diagnoses, surgical indications, surgical details, and complications were recorded. Preoperative imaging was reviewed to determine atlanto-dens intervals and spinal cord signal changes. Postoperative radiographs or CT scans were reviewed to determine union.
Results
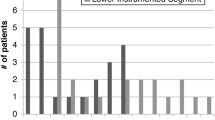
Twelve DS patients met our inclusion criteria. The mean age at surgery was 9.3 years (range 3.8–18.8 years). Patients with secondary causes of instability included 7 patients with os odontoideum and 1 patient with a pars fracture. Three patients (25%) were identified on asymptomatic screening, with none of these having cord signal changes on magnetic resonance imaging (MRI). Modern implants (screws, plates, cages) were used in every patient in our series. The mean number of levels fused was 1.9 (range 1–5). The overall complication rate was 41.7% (5/12). Four patients required repeat surgery for nonunion. All patients with adequate radiographic follow-up demonstrated union (11/11, 100%). One patient was lost to follow-up.
Conclusions
Fixation for cervical instability is a critical component of the management of DS. A minority of patients receiving surgery were identified through asymptomatic screening. There was a high complication risk associated with surgery in our study; however, the addition of rigid fixation has lessened the complication rate compared with previous studies.
Level of Evidence
Level IV.
Similar content being viewed by others

References
Brockmeyer D. Down syndrome and craniovertebral instability. Topic review and treatment recommendations. Pediatr Neurosurg 1999;31:71–7.
Pueschel SM, Scola FH. Atlantoaxial instability in individuals with Down syndrome: epidemiologic, radiographic, and clinical studies. Pediatrics 1987;80:555–60.
Micheli L, Stein C, O’Brien M, d’Hemecourt P. Spinal injuries and conditions in young athletes. New York, NY: Springer; 2014.
Wind WM, Schwend RM, Larson J. Sports for the physically challenged child. J Am Acad Orthop Surg 2004;12:126–37.
Doyle JS, Lauerman WC, Wood KB, Krause DR. Complications and long-term outcome of upper cervical spine arthrodesis in patients with Down syndrome. Spine (Phila Pa 1976) 1996;21:1223–31.
Nader-Sepahi A, Casey AT, Hayward R, et al. Symptomatic atlantoaxial instability in Down syndrome. J Neurosurg 2005; 103(3 suppl):231–7.
Segal LS, Drummond DS, Zanotti RM, et al. Complications of posterior arthrodesis of the cervical spine in patients who have Down syndrome. J Bone Joint Surg Am 1991;73:1547–54.
Smith MD, Phillips WA, Hensinger RN. Fusion of the upper cervical spine in children and adolescents. An analysis of 17 patients. Spine (Phila Pa 1976) 1991;16:695–701.
Anderson RC, Ragel BT, Mocco J, et al. Selection of a rigid internal fixation construct for stabilization at the craniovertebral junction in pediatric patients. J Neurosurg 2007;107(1 suppl):36–42.
Couture D, Avery N, Brockmeyer DL. Occipitocervical instrumentation in the pediatric population using a custom loop construct: initial results and long-term follow-up experience. J Neurosurg Pediatr 2010;5:285–91.
Haque A, Price AV, Sklar FH, et al. Screw fixation of the upper cervical spine in the pediatric population. Clinical article. J Neurosurg Pediatr 2009;3:529–33.
Ito K, Imagama S, Ito Z, et al. Screw fixation for atlantoaxial dislocation related to Down syndrome in children younger than 5 years. J Pediatr Orthop B 2017;26:86–90.
Jea A, Taylor MD, Dirks PB, et al. Incorporation of C-1 lateral mass screws in occipitocervical and atlantoaxial fusions for children 8 years of age or younger. Technical note. J Neurosurg 2007;107(2 suppl): 178–83.
Kuroki H, Kubo S, Hamanaka H, Chosa E. Posterior occipito-axial fixation applied C2 laminar screws for pediatric atlantoaxial instability caused by Down syndrome: report of 2 cases. Int J Spine Surg 2012;6:210–5.
Hwang SW, Gressot LV, Rangel-Castilla L, et al. Outcomes of instrumented fusion in the pediatric cervical spine. J Neurosurg Spine 2012;17:397–409.
Wang J, Vokshoor A, Kim S, et al. Pediatric atlantoaxial instability: management with screw fixation. Pediatr Neurosurg 1999;30:70–8.
Author information
Authors and Affiliations
Corresponding author
Additional information
Author disclosures: BWY (none), DJH (none), MRP (none), MT (none), MTH (other from Medtronics, outside the submitted work), MPG (other from Orthobullets, NuVasive, DePuy, Zimmer Biomet, Medtronic, Growing Spinal Study Group [GSSG], Children’s Spine Study Group [CSSG], and Harms Study Group [HSG], outside the submitted work).
IRB approval: This research was approved by our institutional IRB (IRB Number: P00020884).
Funding: No funding sources to disclose.
Rights and permissions
About this article

Cite this article
Yang, B.W., Hedequist, D.J., Proctor, M.R. et al. Surgical Fixation Using Screw-Rod Construct Instrumentation for Upper Cervical Instability in Pediatric Down Syndrome Patients. Spine Deform 7, 957–961 (2019). https://doi.org/10.1016/j.jspd.2019.03.002
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1016/j.jspd.2019.03.002