
Abstract
Study Design
Retrospective evaluation of cervical spine images from 2006–2012 for the purposes of “screening” children with Down syndrome for instability.
Objective
To determine whether a full series of cervical spine images including flexion/extension lateral (FEL) radiographs was needed to avoid missing upper cervical instability.
Summary of Background Data
The best algorithm, measurements, and criteria for screening children with Down syndrome for upper cervical instability are controversial. Many authors have recommended obtaining flexion and extension views. We noted that patients who require surgical stabilization due to myelopathy or cord compression typically have grossly abnormal radiographic measurements on the neutral upright lateral (NUL) cervical spine radiograph.
Methods
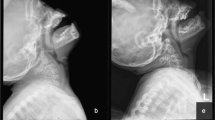
The atlanto-dental interval, space available for cord, and basion axial interval were measured on all films. The Weisel-Rothman measurement was made in the FEL series. Clinical outcome of those with abnormal measurements were reviewed. Sensitivity, specificity, and positive and negative predictive values of NUL and FEL radiographs for identifying clinically significant cervical spine instability were calculated.
Results
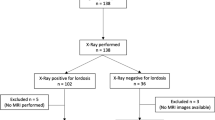
A total of 240 cervical spine series in 213 patients with Down syndrome between the ages of 4 months and 25 years were reviewed. One hundred seventy-two children had an NUL view, and 88 of these patients also had FEL views. Only one of 88 patients was found to have an abnormal atlanto-dental interval (≥6 mm), space available for cord at C1 (≤14 mm), or basion axial interval (>12 mm) on an FEL series that did not have an abnormal measurement on the NUL radiograph. This patient had no evidence of cord compression or myelopathy.
Conclusions
Obtaining a single NUL radiograph is an efficient method for radiographic screening of cervical spine instability. Further evaluation may be required if abnormal measurements are identified on the NUL radiograph. We also propose new “normal” values for the common radiographic measurements used in assessing risk of cervical spine instability in patients with Down syndrome.
Level of Evidence
Level IV.
Similar content being viewed by others

References
American Academy of Pediatrics, Committee on Sports Medicine and Fitness. Atlantoaxial instability in Down syndrome: subject review. Pediatrics 1995;96:151–4.
Burke SW, French HG, Roberts JM, et al. Chronic atlanto-axial instability in Down syndrome. J Bone Joint Surg Am 1985;67:1356–60.
Tredwell SJ, Newman DE, Lockitch G. Instability of the upper cervical spine in Down syndrome. J Pediatr Orthop 1990;10:602–6.
Spitzer R, Rabinowitch JY, Wybor KC. A study of the abnormalities of skull, teeth, and lenses in mongolism. Can Med Assoc J 1961;84:567.
Matsuda Y, Sano N, Watanabe S, et al. Clinical predictors and radiological reliability in subjects with Down’s syndrome. Spine 1995;20:2283–6.
Pueschel SM, Scola FH. Atlantoaxial instability in individuals with Down syndrome: epidemiologic, radiographic, and clinical studies. Pediatrics 1987;80:555–60.
Selby KA, Newton RW, Gupta S, et al. Clinical predictors and radiological reliability in atlantoaxial subluxation in Down’s syndrome. Arch Dis Child 1991;66:876–8.
American Academy of Pediatrics, Committee on Sports Medicine. Atlantoaxial instability in Down syndrome: subject review. Pediatrics 1984;74:152–4.
Wellborn CC, Sturm PF, Hatch RS, et al. Intra-observer reproducibility and inter-observer reliability of cervical spine measurements. J Pediatr Orthop 2000;20:66–70.
Karol LA, Sheffield EG, Crawford K, et al. Reproducibility in the measurement of atlanto-occipital instability in children with Down syndrome. Spine 1996;21:2463–8.
Oda T, Yonenobu K, Fujimura Y, et al. Diagnostic validity of space available for the spinal cord at C1 level for cervical myelopathy in patients with rheumatoid arthritis. Spine 2009;34:1395–8.
Harris JH, Carson GC, Wagner LK. Radiologic diagnosis of traumatic occipitovertebral dissociation. AJR Am J Roentgenol 1994;162:887–92.
Hakinson TC, Anderson RCE. Craniovertebral junction abnormalities in Down syndrome. Neurosurgery 2010;66A32–8.
Wiesel SW, Rothman RH. Occipitoatlantal hypermobility. Spine 1979;4:187–91.
Nakamura N, Inaba Y, Oba M, et al. Novel 2 radiographical measurements for atlantoaxial instability in children with Down syndrome. Spine 2014;39:E1566–74.
Gabriel KR, Mason DE, Carango P. Occipito-atlantal translation in Down’s syndrome. Spine 1990;15:997–1002.
Ferguson RL, Putney ME, Allen BL, et al. Comparison of neurological deficits with atlanto-dens intervals in patients with Down syndrome. J Spinal Disord 1997;10:246–52.
Harley EH, Collins MD. Neurologic sequelae secondary to atlantoaxial instability in Down syndrome. Implications in otolaryngologic surgery. Arch Otolaryngol Head Neck Surg 1994;120:159–65.
Powell JF, Woodcock T, Luscombe FE. Atlantoaxial subluxation in Down syndrome. Anaesthesia 1990;45:1049–51.
Rosenbaum DM, Blumhagen JD, King HA. Atlantooccipital instability in Down syndrome. AJR Am J Roentgenol 1986;146:1269–72.
Brockmeyer D. Down syndrome and craniovertebral instability. Topic review and treatment recommendations. Pediatr Neurosurg 1999;31:71–7.
Author information
Authors and Affiliations
Corresponding author
Additional information
Author disclosures: MB (Orthopaediatrics Inc, Nuvasive, Novadip, unrelated), JMB (Johnson&Johnson, unrelated), VB (none), WFK (none).
IRB approval: This study was approved by Seattle Children’s Hospital, PIROSTUDY13906.
Funding: There were no funding sources.
Rights and permissions
About this article

Cite this article
Bouchard, M., Bauer, J.M., Bompadre, V. et al. An Updated Algorithm for Radiographic Screening of Upper Cervical Instability in Patients With Down Syndrome. Spine Deform 7, 950–956 (2019). https://doi.org/10.1016/j.jspd.2019.01.012
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1016/j.jspd.2019.01.012