
Abstract
Study Design
Retrospective review of prospective data.
Objective
To delineate a curve threshold where further delay of surgery significantly increased the risks for patients with cerebral palsy (CP) scoliosis.
Summary of Background Data
Two approaches exist in the management of CP scoliosis: a proactive one where surgery is recommended once there is a risk of progression (Cobb > 50°) and a reactive one where surgery is recommended after the patient/caregiver may have significant challenges caused by a large deformity.
Methods
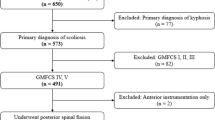
A prospectively collected CP scoliosis surgical registry was queried for patients with minimum two years of follow-up. Three groups were delineated based on the distribution of curve magnitudes: <70° (proactive), 70°–90°, and >90° (reactive). Radiographic, surgical, and quality of life outcome data were compared between the groups using analysis of variance and chi-square analyses.
Results
There were 38 patients in the <70° group, 44 in the 70°—90° group, and 42 in the >90° group. They were similar in age. The >90° group had significantly longer operative time (p < .001), a higher percentage of anterior/posterior procedures (31% vs 5%), and a higher infection rate requiring I&D (16.7%) than the other groups (<70°: 5.3%; 70°–90°: 6.8%; p < .05). The percentage blood volume loss was significantly higher in the >90° group compared to <70°. There were no differences in length of hospitalization or intensive care unit stay. Preoperatively, the Caregiver Priorities and Child Health Index of Life with Disabilities (CPchild) QOL score was significantly higher for the <70° group. At two years, the <70° and 70°–90° groups reached similar QOL scores, whereas the >90° trended toward a lower postoperative QOL.
Conclusions
Being proactive (Cobb <70°) has no advantage in terms of decreasing risks or improving outcomes compared to curves 70°–90°. However, delaying surgery to a curve greater than 90° increases the risk of infection, blood loss, and the need for anterior/ posterior procedures. Ideally, surgery should be recommended for curves less than 90°.
Similar content being viewed by others


References
Lonstein J. Spine deformities due to cerebral palsy. In: Weinstein S, editor. The pediatric spine: principles & practice. 2nd ed. Philadelphia, PA: Lippincott, Williams, & WIlkens; 2001. p. 797–807.
Tsirikos A. Development and treatment of spinal deformity in patients with cerebral palsy. Indian J Orthop 2010;44:148–58.
Karampalis C, Tsirikos AI. The surgical treatment of lordoscoliosis and hyperlordosis in patients with quadriplegic cerebral palsy. Bone Joint J 2014;96–B:800–6.
Thomson JD, Banta JV. Scoliosis in cerebral palsy: an overview and recent results. J Pediatr Orthop B 2001;10:6–9.
Comstock CP, Leach J, Wenger DR. Scoliosis in total-body-involvement cerebral palsy. Analysis of surgical treatment and patient and caregiver satisfaction. Spine (Phila Pa 1976) 1998;23:1412–24; discussion 24–5.
Thometz JG, Simon SR. Progression of scoliosis after skeletal maturity in institutionalized adults who have cerebral palsy. J Bone Joint Surg Am 1988;70:1290–6.
Narayanan UG, Fehlings D, Weir S, et al. Initial development and validation of the Caregiver Priorities and Child Health Index of Life with Disabilities (CPCHILD). Dev Med Child Neurol 2006;48: 804–12.
Samdani AF, Belin EJ, Bennett JT, et al. Major perioperative complications after spine surgery in patients with cerebral palsy: assessment of risk factors. Eur Spine J 2016;25:795–800.
Sharma S, Wu C, Andersen T, et al. Prevalence of complications in neuromuscular scoliosis surgery: a literature meta-analysis from the past 15 years. Eur Spine J 2013;22:1230–49.
Toovey R, Harvey A, Johnson M, et al. Outcomes after scoliosis surgery for children with cerebral palsy: a systematic review. Dev Med Child Neurol 2017;59:690–8.
Lonstein JE, Akbarnia A. Operative treatment of spinal deformities in patients with cerebral palsy or mental retardation. An analysis of one hundred and seven cases. J Bone Joint Surg Am 1983;65:43–55.
Modi HN, Suh SW, Yang JH, et al. Surgical complications in neuromuscular scoliosis operated with posterior-only approach using pedicle screw fixation. Scoliosis 2009;4:11.
Jain A, Sponseller PD, Shah SA, et al. Incidence of and risk factors for loss of 1 blood volume during spinal fusion surgery in patients with cerebral palsy. J Pediatr Orthop 2017;37:e484–7.
Sponseller PD, Shah SA, Abel MF, et al. Infection rate after spine surgery in cerebral palsy is high and impairs results: multicenter analysis of risk factors and treatment. Clin Orthop Relat Res 2010;468:711–6.
Tsirikos AI, Chang WN, Dabney KW, et al. Comparison of parents’ and caregivers’ satisfaction after spinal fusion in children with cerebral palsy. J Pediatr Orthop 2004;24:54–8.
Author information
Authors and Affiliations
Corresponding author
Additional information
Author disclosures: SMH (none), BY (grants from Setting Scoliosis Straight Foundation, during the conduct of the study; grants and personal fees from K2M and DePuy Synthes Spine; personal fees from NuVasive, Medtronic, Orthopediatrics, Stryker, and Globus; grants from Setting Scoliosis Straight Foundation, outside the submitted work; in addition, BY has a patent K2M with royalties paid), PDS (grants from Setting Scoliosis Straight Foundation, during the conduct of the study; personal fees from DePuy Synthes Spine and Globus, outside the submitted work), CEB (grants from Setting Scoliosis Straight Foundation, during the conduct of the study), SAS (grants from Setting Scoliosis Straight Foundation and from DePuy Synthes Spine and K2M in support of Harms Study Group research, during the conduct of the study; personal fees from DePuy Synthes Spine, K2M, and NuVasive, outside the submitted work), JA (grants from Setting Scoliosis Straight Foundation, during the conduct of the study), MFA (grants from Setting Scoliosis Straight Foundation, during the conduct of the study), FM (grants from Setting Scoliosis Straight Foundation, during the conduct of the study), PON (grants from Setting Scoliosis Straight Foundation, during the conduct of the study; grants and other from Setting Scoliosis Straight Foundation and Scoliosis Research Society; other from Rady Children’s Specialists; grants, personal fees, and nonfi-nancial support from DePuy Synthes Spine and K2M; grants from EOS imaging and NuVasive; personal fees from Thieme Publishing and Cubist; other from Electrocore and International Pediatric Orthopedic Think Tank; grants, nonfinancial support, and other from Orthopediatrics; grants and nonfinancial support from Alphatech, outside the submitted work; in addition, PON has a patent “Anchoring Systems and Methods for Correcting Spinal Deformities” (8540754) with royalties paid to DePuy Synthes Spine, a patent “Low Profile Spinal Tethering Systems” (8123749) licensed to DePuy Spine, Inc., a patent “Screw Placement Guide” (7981117) licensed to DePuy Spine, Inc., a patent “Compressor for Use in Minimally Invasive Surgery” (7189244) licensed to DePuy Spine, Inc., and a patent “Posterior Spinal Fixation Pending” to K2M).The study was conducted at Rady Children’s Hospital, San Diego, CA.IRB approval was obtained for this study.
Rights and permissions
About this article

Cite this article
Hollenbeck, S.M., Yaszay, B., Sponseller, P.D. et al. The Pros and Cons of Operating Early Versus Late in the Progression of Cerebral Palsy Scoliosis. Spine Deform 7, 489–493 (2019). https://doi.org/10.1016/j.jspd.2018.09.002
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1016/j.jspd.2018.09.002