
Abstract
Study Design
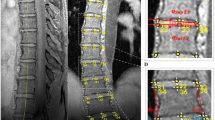
The aim of this study was to measure contributions of individual vertebra and disc wedging to coronal Cobb angle in the growing scoliotic spine using sequential magnetic resonance imaging (MRI). Clinically, the Cobb angle measures the overall curve in the coronal plane but does not measure individual vertebra and disc wedging. It was hypothesized that patients whose deformity progresses will have different patterns of coronal wedging in vertebrae and discs to those of patients whose deformities remain stable.
Methods
A group of adolescent idiopathic scoliosis (AIS) patients each received two to four MRI scans (spaced 3–12 months apart). The coronal plane wedge angles of each vertebra and disc in the major curve were measured for each scan, and the proportions and patterns of wedging in vertebrae and discs were analyzed for subgroups of patients whose spinal deformity did and did not progress during the study period.
Results
Sixteen patients were included in the study; the mean patient age was 12.9 years (standard deviation 1.7 years). All patients were classified as right-sided major thoracic Lenke Type 1 curves (9 type 1A, 4 type 1B, and 3 type 1C). Cobb angle progression of ⩾5° between scans was seen in 56% of patients. Although there were measurable changes in the wedging of individual vertebrae and discs in all patients, there was no consistent pattern of deformity progression between patients who progressed and those who did not. The patterns of progression found in this study did not support the hypothesis of wedging commencing in the discs and then transferring to the vertebrae.
Conclusion
Sequential MRI data showed complex patterns of deformity progression. Changes to the wedging of individual vertebrae and discs may occur in patients who have no increase in Cobb angle; therefore, the Cobb method alone may be insufficient to capture the complex mechanisms of deformity progression.
Similar content being viewed by others


References
Cobb J. Outline for the study of scoliosis. Instr Course Lect Am Acad Orthop Surg 1948;5:261–75.
Schick D. Computed tomography radiation doses for paediatric scoliosis scans. Unpublished internal report commissioned by Paediatric Spine Research Group from Queensland Health Biomedical Technology Services, Brisbane, Australia, 2004.
Pace N, Ricci L, Negrini S. A comparison approach to explain risks related to x-ray imaging for scoliosis, 2012 SOSORT award winner. Scoliosis 2013;8:11.
Presciutti SM, Karukanda T, Lee M. Management decisions for adolescent idiopathic scoliosis significantly affect patient radiation exposure. Spine J 2014;14:1984–90.
Levy AR, Goldberg MS, Mayo NE, et al. Reducing the lifetime risk of cancer from spinal radiographs among people with adolescent idiopathic scoliosis. Spine 1996;21:1540–7.
Stokes IA, Aronsson DD. Disc and vertebral wedging in patients with progressive scoliosis. J Spinal Disord 2001;14:317–22.
Scherrer SA, Begon M, Leardini A, et al. Three-dimensional vertebral wedging in mild and moderate adolescent idiopathic scoliosis. PLoS One 2013;8:e71504.
Modi HN, Suh SW, Song HR, et al. Differential wedging of vertebral body and intervertebral disc in thoracic and lumbar spine in adolescent idiopathic scoliosis—a cross sectional study in 150 patients. Scoliosis 2008;3:11.
Clin J, Aubin C-É, Lalonde N, et al. A new method to include the gravitational forces in a finite element model of the scoliotic spine. Med Biol Eng Comput 2011;49:967–77.
Will RE, Stokes IA, Qiu X, et al. Cobb angle progression in adolescent scoliosis begins at the intervertebral disc. Spine 2009;34:2782–6.
Taylor TK, Ghosh P, Bushell GR. The contribution of the intervertebral disk to the scoliotic deformity. Clin Orthop Relat Res 1981:79-90.
Risser JC. The Iliac apophysis; an invaluable sign in the management of scoliosis. Clin Orthop Relat Res 1958;11:111–9.
Keenan BE, Izatt MT, Askin GN, et al. Segmental torso masses in adolescent idiopathic scoliosis. Clin Biomech (Bristol, Avon) 2014;29:773–9.
Schmitz A, Konig R, Kandyba J, et al. Visualisation of the brace effect on the spinal profile in idiopathic scoliosis. Eur Spine J 2005;14:138–43.
Lenke LG, Betz RR, Harms J, et al. Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am 2001;83:1169–81.
Charles YP, Dimeglio A, Canavese F, Daures JP. Skeletal age assessment from the olecranon for idiopathic scoliosis at Risser grade 0. J Bone Joint Surg Am 2007;89:2737–44.
Tan KJ, Moe MM, Vaithinathan R, Wong HK. Curve progression in idiopathic scoliosis: follow-up study to skeletal maturity. Spine 2009;34:697–700.
Soucacos PN, Zacharis K, Gelalis J, et al. Assessment of curve progression in idiopathic scoliosis. Eur Spine J 1998;7:270–7.
Weinstein SL, Ponseti IV. Curve progression in idiopathic scoliosis. J Bone Joint Surg Am 1983;65:447–55.
Author information
Authors and Affiliations
Corresponding author
Additional information
Author disclosures
BEK (none); MTI (none); GNA (none), RDL (none); DDB (none); MJP (none); CJA (none).
Rights and permissions
About this article

Cite this article
Keenan, B.E., Izatt, M.T., Askin, G.N. et al. Sequential Magnetic Resonance Imaging Reveals Individual Level Deformities of Vertebrae and Discs in the Growing Scoliotic Spine. Spine Deform 5, 197–207 (2017). https://doi.org/10.1016/j.jspd.2016.10.002
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1016/j.jspd.2016.10.002