
Abstract
Purpose
Traditional pulmonary function testing can be difficult for both the subject and the test administrator and are dependent on the subject’s effort and ability to follow directions. An alternative to traditional pulmonary function testing is the kinematic analysis of the chest wall. Kinematic analysis is a reliable and accurate method to evaluate pulmonary function testing that does not have the restrictions of traditional methods. It is the purpose of this study to present a new model for measuring chest motion during pulmonary function testing of children with adolescent idiopathic scoliosis (AIS) and able-bodied children.
Procedures
Traditional pulmonary function testing and kinematic assessment of the chest wall was measured simultaneously during a flow volume loop and maximum voluntary ventilation test. Fifteen children with AIS and 15 able-bodied children were measured. Differences between the two groups (AIS and able-bodied) and the two testing methods (traditional and kinematic testing) were analyzed. Correlations for the two testing methods and interclass coefficients for the kinematic analysis were measured.
Findings
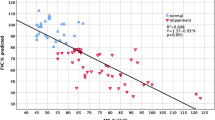
There were no significant differences between the control group and the scoliosis group when comparing data from traditional and kinematic assessments. When comparing the differences between the traditional and kinematic data collection methods, there were significant differences for the flow volume loop and maximum voluntary ventilation. For all significant parameters, the kinematic analysis demonstrated higher values. Moderate to high Pearson correlations were found between collection methods, and high to moderate interclass correlation coefficient values were found for the kinematic analysis of the chest wall.
Principal Conclusions
Kinematics of the chest wall can be used as a valuable resource in the future when measuring pulmonary function when a traditional method is not a viable option.
Similar content being viewed by others


References
Muniyappanavar N, Shivakumar J, Dixit P, et al. Impact of asymptomatic idiopathic scoliosis on pulmonary function. Natl J Physiol Pharma Pharmacol 2013;3: 153e7.
Tsiligiannis T, Grivas T. Pulmonary function in children with idio-pathic scoliosis. Scoliosis 2012;7: 1e7.
Leong J, Lu W, Luk K, et al. Kinematics of the chest cage and spine during breathing in healthy individuals and in patients with adolescent idiopathic scoliosis. Spine 1999;24:1310.
Newton P, Faro F, Gollogly S, et al. Results of preoperative pulmonary function testing of adolescents with idiopathic scoliosis. A study of six hundred and thirty-one patients. J Bone Joint Surg Am 2005;87A:1937e46.
Weinstein S, Zavala D, Ponseti I. Idiopathic scoliosis long term follow-up and prognosis in untreated patients. J Bone Joint Surg Am 1981;63A:702e11.
Dugdale A, Moeri M. Normal values of forced vital capacity (FVC), forced expiratory volume (FEV 1-0), and peak flow rate (PFR) in children. Arch Dis Child 1968;43: 229e34.
Kim Y, Lenke L, Bridwell K, et al. Pulmonary function in adolescent idiopathic scoliosis relative to the surgical procedure. J Bone Joint Surg Am 2005;87A:1534e41.
Jat KR. Spirometry in children. Prim Care Respir J 2013;22: 221e9.
Smith J, Aliverti A, Quaranta M, et al. Chest wall dynamics during voluntary and induced cough in healthy volunteers. J Physiol 2012;590: 563e74.
Boudarham J, Pradon D, Prigent H, et al. Optoelectronic plethysmog-raphy as an alternative method for the diagnosis of unilateral diaphragmatic weakness. Chest 2013;144: 887e95.
Boudarham J, Pradon D, Prigent H, et al. Optoelectronic vital capacity measurement for restrictive diseases. Respir Care 2013;58: 633e8.
Lanza F, Camargo A, Archija L, et al. Chest wall mobility is related to respiratory muscle strength and lung volumes in healthy subjects. Respir Care 2013;58: 2107e12.
LoMauro A, Pochintesta S, Romei M, et al. Rib cage deformities alter respiratory muscle action and chest wall function in patients with severe osteogenesis imperfecta. PLoS One 2012;7: 1e8.
Bruni G, Gigliotti F, Scano G. Use of Optoelectronic Plethysmography in Pulmonary Rehabilitation and Thoracic Surgery, Optoelectronics — Advanced Materials and Devices, Prof. Sergei Pyshkin (Ed.), ISBN: 978-953-51-0922-8, InTech.
Vieiraa D, Hoffmanb M, Pereirac D, et al. Optoelectronic plethys-mography: intra-rater and inter-rater reliability in healthy subjects. Respir Physiol Neurobiol 2013;189: 473e6.
Binazzia B, Innocenti Brunia G, Colia C, et al. Chest wall kinematics in young subjects with Pectus excavatum. Respir Physiol Neurobiol 2012;180: 211e7.
Lanini B, Bianchi R, Romagnoli I, et al. Chestwall kinematics in patients with hemiplegia. Am J Respir Crit Care Med 2003;168: 109e13.
Groote A, Wantier M, Cheron G, et al. Chest wall motion during tidal breathing. J Appl Physiol 1997;83: 1531e7.
Romagnoli I, Gigliotti F, Galarducci A, et al. Chest wall kinematics and respiratory muscle action in ankylosing spondylitis patients. Eur Respir J 2004;24: 453e60.
Aliverti A, Ghidoli G, Dellaca L, et al. Chest wall kinematic determinants of diaphragm length by optoelectronic plethysmography and ul-trasonography. J Appl Physiol 2003;94: 621e30.
Aliverti A, Stevenson N, Dellaca R, et al. Regional chest wall volumes during exercise in chronic obstructive pulmonary disease. Thorax 2004;59: 210e6.
Sanna A, Bertoli F, Misuri G, et al. Chest wall kinematics and respiratory muscle action in walking healthy humans. J Appl Physiol 1999;87: 938e46.
Vitale M, Matsumoto H, Bye M, et al. A retrospective cohort study of pulmonary function, radiographic measures, and quality of life in children with congenital scoliosis: an evaluation of patient outcomes after early spinal fusion. Spine 2008;33: 1242e9.
Solache-Carranco A, Sanchez-Bringas M. Evaluation of a respiratory rehabilitation program in children with scoliosis. Cir Cir 2012;80:11–7.
Koller H, Zenner J, Gajic V, et al. The impact of halo-gravity traction on curve rigidity and pulmonary function in the treatment of severe and rigid scoliosis and kyphoscoliosis: a clinical study and narrative review of the literature. Eur Spine J 2012;21: 514e29.
Korovessis P, Filos K, Georgopoulos D. Long-term alterations of respiratory function in adolescents wearing a brace for idiopathic scoli-osis. Spine 1996;21: 1979e84.
Bianchi R, Gigliotti F, Romagnoli I, et al. Chest wall kinematics and breathlessness during pursed-lip breathing in patients with COPD. Chest 2004;125: 459e65.
Emans J, Caubet J, Ordonez C, et al. The treatment of spine and chest wall deformities with fused ribs by expansion thoracostomy and insertion of vertical expandable prosthetic titanium ribs. Spine 2005;30:S58e68.
Beydon N, Davis S, Lombardi E, et al. An official American Thoracic Society/European Respiratory Society statement: pulmonary function testing in preschool children. Am J Respir Crit Care Med 2007;175: 1304e45.
Author information
Authors and Affiliations
Corresponding author
Additional information
Author disclosures: HW (none), JW (none), JK (none), SA (none), TM (none), HI (none).
Rights and permissions
About this article

Cite this article
White, H., Wallace, J., King, J. et al. A Prospective Comparison of Pulmonary Function Using Traditional and Kinematic Measures in Children With and Without Adolescent Idiopathic Scoliosis. Spine Deform 3, 554–559 (2015). https://doi.org/10.1016/j.jspd.2015.04.002
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1016/j.jspd.2015.04.002