
Abstract
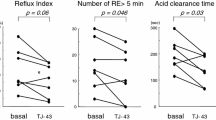
Proton pump inhibitors are the mainstay of medical management in gastroesophageal reflux disease. Although they provide relief from most symptoms, refluxmay persist.Wehypothesize that omeprazole does not reduce the total amount of gastroesophageal reflux but simply alters its pH characteristics. Six asymptomatic volunteers had combined 24-hour impedance pH monitoring before and after 7 days of omeprazole (20 mg BID). Multichannel intraluminal impedance was used to identify reflux episodes, which were classified as acid (pH < 4), weak acid (pH > 4 but decrease > 1 pH unit) and nonacid (pH > 4 and decrease<1 pHunit) bypH measurements 5 cmabove the lower esophageal sphincter (LES). A gastric pH sensor located 10 cm below the LES was used to verify the action of omeprazole. Impedance detected a total of 116 reflux episodes before and 96 episodes after omeprazole treatment. The median number of reflux episodes (18 versus 16, P = 0.4), median duration of reflux episodes (4.7 versus 3.6 minutes, P = 0.5), and total duration of reflux episodes (27.2 versus 42.4 minutes, P = 0.5) per subject were similar before and after omeprazole. Acid reflux episodes were reduced from 63% before to 2.1% after omeprazole (P = 0.0001), whereas nonacid reflux episodes increased (15% to 76%, P = 0.0001). Weak acid reflux episodes did not change (22.4% to 21.8%, P = 1.0). The proportion of reflux episodes greater than pH 4 increased from 37% to 98% (P = 0.0001). In normal subjects, omeprazole treatment does not affect the number of reflux episodes or their duration; rather it converts acid reflux to less acid reflux, thus exposing esophagus to altered gastric juice. These observations may explain the persistence of symptoms and emergence of mucosal injury white on proton pump inhibitor therapy.
Similar content being viewed by others

References
Wetscher GJ, Glaser K, Hinder RA, Perdikis G, Klingler P, Bammer T, et al. Respiratory symptoms in patients with gastroesophageal reflux disease following medical therapy and following antireflux surgery. Am J Surg 1997;174:639–642.
Oberg S, Johansson J, Wenner J, Johnsson F, Zilling T, von Holstein CS, et al. Endoscopic surveillance of columnarlined esophagus: frequency of intestinal metaplasia detection and impact of antireflux surgery. Ann Surg 2001;234:619–626.
Devault KR, Castell DO. Updated guidelines for the diagnosis and treatment of gastroesophageal reflux disease. Am J Gastroenterol 1999;94:1434–1442.
Johnson LF, DeMeester TR. Twenty-four-hourpH monitoring of the distal esophagus. A quantitative measure of gastroesophageal reflux. Am J Gastroenterol 1974;62:325–332.
Tutuian R, Vela MF, Balaji NS, Wise JL, Murray JA, Peters JH, et al. Esophageal function testing with combined multichannel intraluminal impedance and manometry: multicenter study in healthy volunteers. Clin Gastroenterol Hepatol 2003;1:174–182.
Shay S, Vela M, Tutuian R, Balaji N, Wise J, Adhami T, et al. Twenty-four hour multichannel intraluminal impedance and pH (24h MII-pH): a multicenter report of normal values from 45 healthy volunteers. Gastroenterology 2002;122:A-577.
Skopnik H, Silny J, Heiber O, Schulz J, Rau G, Heimann G. Gastroesophageal reflux in infants: evaluation of a new intraluminal impedance technique. J Pediatric Gastroenterol Nutr 1996;23:591–598.
Sifrim D, Holloway R, Silny J, Xin Z, Tack J, Lerut A, et al. Acid, nonacid, and gas reflux in patients with gastroesophageal re.ux disease during ambulatory 24-hour pH-impedance recordings. Gastroenterology 2001;120:1588–1598.
Tutuian R, Vela MF, Shay SS, Castell DO. Multichannel intraluminal impedance in esophageal function testing and gastroesophageal reflux monitoring. J Clin Gastroenterol 2003;37:206–215.
Wenzl TG, Silny J, Schenke S, Peschgens T, Heimann G, Skopnik H. Gastroesophageal reflux and respiratory phenomena in infants: status of the intraluminal impedance technique. J Pediatr Gastroenterol Nutr 1999;28:423–428.
Wenzl TG, Schenke S, Peschgens T, Silny J, Heimann G, Skopnick H. Association of apnea and nonacid gastroesophageal reflux in infants: investigations with the intraluminal impedance technique. Pediatr Pulmonol 2001;31:144–149.
DeMeester TR. Barrett’s esophagus: the process of intestinalization. Probl Gen Surg 2001;18:31–42.
Chandrasoma PT, Der R, Dalton P, Kobayashi G, Ma Y, Peters J, et al. Distribution and significance of epithelial types in columnar-lined esophagus. Am J Surg Pathol 2001;25:1188–1193.
Fitzgerald RC, Omary MB, Triadafilopoulos G. Dynamics effects of acid on Barrett’s esophagus: an ex vivo proliferation and differentiation model. J Clin Invest 1996;98:2120–2128.
Theodorou D, Streets C, Chandrasoma P, Balaji NS, Bruce D, Gattolin A, et al. Comparison of the pH and the intestinal metaplasia density across long segment Barrett’s esophagus. Gastroenterology 2002;122:A-51.
Vela MF, Camacho-Lobato L, Srinivasan R, Tutuian R, Katz PO, Castell DO. Simultaneous intraesophageal impedance and pH measurement of acid and nonacid gastroesophageal reflux: effect of omeprazole. Gastroenterology 2001;120:1599–1606.
Cucchiara S, Minella R, Campanozzi A, Salvia G, Borrelli O, Ciccimarra E, et al. Effects of omeprazole on mechanisms of gastroesophageal reflux in childhood. Dig Dis Sci 1997;42:293–299.
Decktor DL, Krawet SH, Rodriguez SL, Robinson M, Castell DO. Dual site ambulatory pH monitoring: a probe across the lower esophageal sphincter does not induce gastroesophageal reflux. Am J Gastroenterol 1996;91:1162–1166.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Tamhankar, A.P., Peters, J.H., Portale, G. et al. Omeprazole does not reduce gastroesophageal reflux: new insights using multichannel intraluminal impedance technology. J Gastrointest Surg 8, 888–896 (2004). https://doi.org/10.1016/j.gassur.2004.08.001
Issue Date:
DOI: https://doi.org/10.1016/j.gassur.2004.08.001