
Abstract
Purpose
Caring for patients with low-acuity conditions in Emergency Departments (ED) is often thought to cost more than treating those patients in other ambulatory settings. Understanding the relative cost of care between settings has critical implications for healthcare policy and system design.
Methods
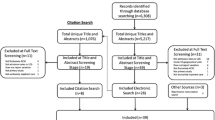
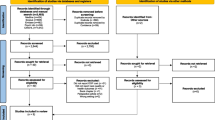
We conducted a systematic review of papers comparing the cost of care for low-acuity and ambulatory care sensitive conditions in ED and other outpatient settings. We searched PubMed, EMBASE, CINAHL, and Web of Science for peer reviewed papers, plus Google for grey literature. We conducted duplicate screening and data extraction, and quality assessment of included studies using an adapted SIGN checklist for economic studies. We calculated an unweighted mean charge ratio across studies and summarized our findings in narrative and tabular format.
Results
We identified one study comparing costs. 18 studies assessed physician or facility charges, conducted in the United States, United Kingdom, and Canada, including cohort analyses (5), charge analyses (5), survey (1), and database searches (5) assessing populations ranging from 370 participants to 60 million. Charge ratios ranged from 0.60 to 13.45 with an unweighted mean of 4.20. Most (12) studies were of acceptable quality.
Conclusion
No studies since 2001 assess the comparative costs of ED versus non-ED care for low-acuity ambulatory conditions. Physician and facility charges for ED care are higher than in other ambulatory settings for low-acuity conditions. Empirical evidence is lacking to support that ED care is more costly than similar care in other ambulatory settings.
Résumé
Objectifs
La prise en charge des patients souffrant d'affections de faible gravité dans les services d'urgence est souvent considérée comme plus coûteuse que la prise en charge de ces mêmes patients dans d'autres structures ambulatoires. Comprendre le coût relatif des soins entre les différents environnements a des implications cruciales pour la politique des soins de santé et la conception des systèmes.
Méthodes
Nous avons procédé à un examen systématique des documents comparant le coût des soins pour les affections à faible gravité et les affections sensibles aux soins ambulatoires dans les services d'urgence et dans d'autres établissements de soins ambulatoires. Nous avons effectué des recherches dans PubMed, EMBASE, CINAHL et Web of Science pour les articles évalués par des pairs, ainsi que dans Google pour la littérature grise. Nous avons procédé à une double sélection et à une extraction des données, ainsi qu'à une évaluation de la qualité des études incluses à l'aide d'une liste de contrôle SIGN adaptée aux études économiques. Nous avons calculé un ratio moyen non pondéré pour l'ensemble des études et avons résumé nos conclusions sous forme de texte et de tableau.
Résultats
Nous avons identifié une étude comparant les coûts. 18 études ont évalué les frais des médecins ou des établissements, menées aux États-Unis, au Royaume-Uni et au Canada, y compris des analyses de cohortes (5), des analyses de frais (5), des enquêtes (1) et des recherches dans des bases de données (5) évaluant des populations allant de 370 participants à 60 millions de personnes. Les taux d'imputation allaient de 0,60 à 13,45, avec une moyenne non pondérée de 4,20. La plupart des études (12) étaient de qualité acceptable.
Conclusion
Depuis 2001, aucune étude n'a évalué les coûts comparatifs des soins aux urgences par rapport aux soins hors urgences pour les affections ambulatoires de faible gravité. Les honoraires des médecins et des établissements pour les soins aux urgences sont plus élevés que dans d'autres structures ambulatoires pour les affections de faible gravité. Il n'existe pas de données empiriques permettant d'affirmer que les soins aux urgences sont plus coûteux que des soins similaires dispensés dans d'autres structures ambulatoires.
Similar content being viewed by others

Data availability
This research does not contain any original data.
References
Stroupe KT, et al. Health-care Costs of Inner-City Patients with Asthma. J of Asthma. 1999;36(8):645–55.
Galarraga J, et al. Costs associated with ambulatory care sensitive conditions across hospital-based settings. Acad Emerg Med. 2015;22(2):172–81.
Morgan, et al. Non–emergency department (ED) interventions to reduce ED utilization a systematic review. Acad Emerg Med. 2013;20(10):969–85.
Hsuan C. Emergency Departments in the United States treating high proportions of patients with ambulatory care sensitive conditions: a retrospective cross-section analysis. BMC Health Serv Res. 2022;22(1):854.
Canadian Institute for Health Informaton. Sources of Potentially Avoidable Emergency Department Visits. Health System Performance. 2014. https://secure.cihi.ca/free_products/ED_Report_ForWeb_EN_Final.pdf. Accessed 5 Dec 2022.
Billings J, et al. Impact of socio-economic status on hospital use in New York City. Health Affairs (Millwood). 1993;12(1):172–3.
Finkler S. The distinction between cost and Charges. Ann Intern Med. 1982;96(1):102–9.
Huserau D, et al. Consolidated health economic evaluation reporting standards (CHEERS) statement. Int J Technol Health Care. 2013;29(2):117–22.
Scottish Intercollegiate Guideline Network. Methodology Checklist 6: Economic Evaluations. 2012. https://www.sign.ac.uk/what-we-do/methodology/checklists/. Accessed 13 July 2022.
Showstack J. The cost of providing nonurgent care in emergency departments. Ann Emerg Med. 2005;45(5):493–4.
Mathews A. When Hospital Fees Catch You Off Guard. The Wall Street Journal, 25 November 2009. https://www.wsj.com/articles/SB10001424052748703819904574555723216593610. Accessed 7 Feb 2023.
Bamezai A, Melnick GA, Nawathe A. The cost of an ED visit and its relationship to ED volume. Ann Emerg Med. 2005;45(5):483–90.
Chen A, Muralidharan M. Algorithms identifying low-acuity emergency department visits: a review and validation study. Health Serv Res. 2022;57(4):979–89.
Acknowledgements
Thank you to Robyn Butcher, Information Specialist, who helped guide our research group in developing the search terms and conducting the search.
Funding
None.
Author information
Authors and Affiliations
Contributions
GS, JB, ASD and AMO: conceived the study and designed the search. AMO: supervised the conduct of the search and data collection. ASD, NI, SB and CLA: provided advice on study design and analysis. GS, JB and AMO: drafted the manuscript, and all the authors contributed substantially to its revision.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Stephen, G., Burton, J., Detsky, A.S. et al. Limited evidence that emergency department care is more costly than other outpatient settings for low-acuity conditions: a systematic review. Can J Emerg Med 25, 387–393 (2023). https://doi.org/10.1007/s43678-023-00477-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43678-023-00477-3
Keywords
- Emergency medicine
- Emergency services
- Low acuity
- Ambulatory
- Primary care
- Outpatient
- Clinic
- Family medicine
- Emergency department
- Cost
- Charges
- Marginal cost
- Economics
- Systematic review