
Abstract
The impact of COVID-19 pandemic put the Italian health system into a test. In the period between September 2020 and June 2021, a weekly average of 114 SARS-CoV-2 infections were recorded in Forlì-Cesena province (north of Italy), with a maximum of 330 cases per week in March 2021; in the same months, the Internal Medicine Unit of Cesena M. Bufalini Hospital managed 954 COVID-19 patients. To allow the management of these patients, the ward was divided into areas at different intensity of care, with a maximum of 39–47 beds and 19–24 in ordinary and sub-intensive area, respectively. Patients had an average age of 66 years, and 62% of the total was female; prevalent comorbidities were arterial hypertension (53%), smoking habit (28.7%), obesity (27.9%), uncomplicated (10%), and complicated diabetes (9%). On the total, 339 patients were hospitalized in sub-intensive area, subjected to non-invasive ventilatory support. Hospitalization lasted about 7 days in the ordinary ward and 13 days in the sub-intensive area. One hundred six patients died. In the considered period, the mean percentage of deaths compared to hospitalizations in Italy was equal to 22.21%; in our experience, the overall mortality rate was 11%. Our organizational model, which included different intensity areas in the same ward and various specialist skills, as the ability to manage non-invasive ventilation and bedside ultrasound, allowed flexible management of the “complex” COVID patient. Even the mortality rate may be the result of this model. These features mark what modern Internal Medicine should be like.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
The end of 2019 will be remembered for the beginning of the pandemic caused by SARS-CoV-2 virus, responsible for the disease called COVID-19 (coronavirus disease 2019) [1].
In Italy, as of January 1, 2022, a total of 137,513 people died because of COVID-19 [2].
The impact of the pandemic, in terms of infection, access to the emergency room and need for hospitalization and/or home care, has put a strain on the national health system.
In the months between October 2020 and April 2021, the pressure exerted on medical departments and intensive care units required a considerable effort from the physicians involved. Alongside intensive care units, Internal Medicine units assumed a crucial role.
The results of a survey promoted by the FADOI (Federation of Associations of Hospital Doctors on Internal Medicine) showed that the employment rate of SARS-CoV-2 patients in Internal Medicine wards, already in November 2020 alone, was 67%. Furthermore, excluding intensive care occupations and considering only medical departments, employment was 75% [3].
This was made possible by the redevelopment, operated by the government, of 4225 beds in the semi-intensive area, especially in Internal Medicine wards [4].
This article shows the organization and results of an integrated management model at multiple levels of intensity in Internal Medicine ward during the pandemic emergency that can fit into the ongoing reflections on the debate and proposals for health care reorganization including Internal Medicine units.
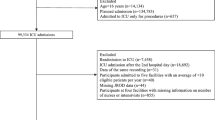
We conducted a retrospective analysis on data collected about hospitalized COVID-19 patients in Internal Medicine ward of the Bufalini Hospital in Cesena (north of Italy, Forlì-Cesena province) in the period between September 2020 and early June 2021 (“second wave”).
M. Bufalini hospital is a community hospital of 450 beds, 32 of which in Internal Medicine ward; it coverages an area of 130,000 inhabitants. This hospital is specialized in trauma and medical emergencies. Infectious Diseases and Pneumology specializations are present as outpatient services; the pulmonologist specialists are part of the Internal Medicine team.
In the analyzed period, a weekly average of 114 SARS-CoV-2 infections was recorded in the province, with a maximum of 330 cases per week in March 2021 [5].
Information was collected from computerized medical records, regarding personal data, comorbidities, need for hospitalization in the sub-intensive area and type of ventilatory device used, length of hospitalization, transfer to other departments, or death. Patient information was anonymized and de-identification prior to analysis. The study was conducted according to the General Data Protection Regulation (RGDP-regulation (EU) 2016/679 of the European parliament and of the council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data and repealing Directive 95/46/EC (General Data Protection Regulation)).
Since September 2020, 11–16 beds of sub-intensive intensity and 21–29 beds of medium intensity setting have been put, until a maximum of 19–24 in the sub-intensive area and 39–47 in the medium intensity during the worse phase of pandemic wave, from February to April 2021 (Fig. 1).

Organization model in M. Bufalini Hospital for the assistance of patients suffering from SARS-CoV-2 during the period between September 2020 and June 2021
Management was led by internist physicians with the support of specialists from other wards (Surgery, Orthopedics, Urology, Radiology, Cardiology, Infectious diseases, etc.).
There were about 2 doctors in medium intensity area and 3–4 doctors in sub-intensive area in the morning and then 2 doctors for the afternoon and night shift; the nursing equipment of 3 units for each shift was implemented.
There were also about 40–60 beds of low-medium intensity COVID care in Geriatric Unit; 8 beds of sub-intensive care were managed by intensivists, who were already management ICU beds.
Patients with moderate illness, defined as evidence of lower respiratory disease (clinical and imaging assessment) and requiring low-flow oxygen, were admitted to the medium intensity area [6].
Patients with severe SARS-CoV-2 pneumoniae, as defined by guidelines, were admitted to the sub-intensive area [6].
In the sub-intensive area, the patients were subjected to continuous multiparametric monitoring, dedicated nursing care, non-invasive ventilatory support (non-invasive ventilatory (NIV), high flow nasal cannula (HFNC), continuous positive airway pressure (CPAP) with mask or helmet).
In the medium intensity area, the oxygen support was delivered by nasal cannula, simple mask, or venturi mask.
When the clinical conditions were improving, firstly for a down-staging in oxygen support, patients were transferred from sub-intensive to the medium intensity area or to Geriatric Unit; vice versa patients were transferred to a higher level of care if they worsened, e.g., sub-intensive care or ICU managed by intensivists (Fig. 1).
In the sub-intensive area, periodic bedside lung ultrasound was performed to monitor the phase of pneumonia and to address the weaning [7, 8]. Echocardiography and vascular Doppler ultrasound at bedside were performed to rule out some complications (e.g., thromboembolism).
Between the competences routinely applied, we report the management of delirium in the elderly patients, the acute and chronic pain, the glycemic decompensation, as well as the remodulation of antihypertensive therapy, the management of malnutrition, pressure sores, and physical deconditioning.
On the basis of an internal agreement, a protocol was drawn up to allow only one family member to access the patient’s room, in exceptional conditions resulting from clinical situation (e.g., end of life).
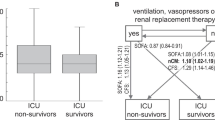
From September 2020 to June 2021, the Internal Medicine ward managed a total of 954 COVID-19 patients whose 339 patients (36%) were hospitalized in its sub-intensive area. The medium of P/F of patients admitted in the sub-intensive area was 200. In the sub-intensive area, in relation to the degree of respiratory failure and compliance, 25.47% of patients underwent HFNC, 22.54% CPAP, and 6.30% NIV. Hospitalization lasted about 7 days in the ordinary ward and 13 days in the sub-intensive area. Patients transferred to ICU or its sub-intensive area were about 9.3%.
Patients had an average age of 66 years, and 62% of the total was female; comorbidities are reported in Fig. 2.

Main comorbidities among hospitalized patients
In the sub-intensive area, 67.2% was female, with a mean age of 68 years; 32.2% of these had a history of smoking, 36% of obesity, 59.2% of arterial hypertension, 11.5% for ischemic heart disease, 45% for uncomplicated diabetes, and 34% for complicated diabetes. A medium of 3–4 lung ultrasound exam was performed per patient.
Considering Charlson Comorbidity Index (CCI) [9], the average value was equal to 19.9 for sub-intensive patients and 2.2 for those hospitalized in medium intensity area.
About mortality, 106 patients, equal to 11% of the total, died: 6.3% in medium and 20% in the sub-intensive area (further differentiation is reported in Table 1).
Seventy-one was female, with an average age of 77 years. The clinical features of the deceased patients were history of arterial hypertension (68.5%), smoking habit (36.2%), obesity (23.3%), ischemic heart disease (16.9%), complicated diabetes (16.1%), diabetes without chronic complications (10%), localized or hematological cancer (17.7%), and dementia (20%).
In deceased people, medium CCI was 28.3 points.
Patients with COVID-19 are complex such as internist patients, with advanced age, burdened by comorbidities, and polypharmacy. COVID-19 turned out to be a multi-organ disease albeit with predominantly pulmonary involvement; it required a management of all collateral issues, from a slow and challenging respiratory weaning, neuro-psychological consequences, nutritional support, and physical rehabilitation, such as the management of pre-existing comorbidities.
The reorganizational model built to deal with the pandemic, which included areas at different levels of care in the same ward and different specialized skills, as the ability to manage ventilotherapy and bedside ultrasound, united by a homogeneous approach to teamwork, allowed flexible management of the “complex” COVID patient.
During the period from September 2020 to June 2021, in our experience, the overall mortality rate of COVID-19 patients was 11% when the average patient death rate in Italy has been equal to 22.2% [10], and 20.5% in our region (Emilia-Romagna), also including the rate of mortality in ICU [10]. Information about other Italian Internal Medicine Unit are not available; this limits the possibility to make comparisons and conclusions on our data.
With these limits, we believe that the lower mortality rate compared to the national data, even with patients with similar characteristics, may be secondary to the clinical management and to the number of doctors involved.
It is not a causality that both in Italy than in other countries with similar health system, most COVID-19 patient management has been led by internists.
Cogliati et al. wrote about the experience between Internal Medicine and Emergency Medicine team at Luigi Sacco Hospital, one of the hospitals most affected by the pandemic wave in northern Italy, to guarantee many COVID wards opened in few days, with a teamwork cooperation and sharing skills and experiences [11].
Agostino Di Ciaula et al., concerning their experience in a big hospital in the south of Italy, demonstrated the important role of the internists in guiding all stages of the disease, as “front-line selection of patients, management of the disease and complications, tight coordination with other specialties, according to specific requirements” [12].
As of November 2021, the COVID-19 patient registry of the Spanish Society of Internal Medicine was already collecting data on more than 25,000 patients [13].
Internal Medicine wards have been primarily involved in the management of COVID-19 due to their intrinsic characteristic to handle polypathology at various levels of disease intensity and the post-acute sequelae of infection for their vocation to the management of chronicity [12, 14].
Y. Jamilloux wrote that many internists have developed specific skills in infectiology, resuscitation, emergency medicine, immunology, geriatrics (…), useful for all-round patient care in order to consent to the French health system of being able to count on doctors and services capable of quickly adapting to new or exceptional medical situations [15].
There has been an active debate about the best COVID-19 emergency health reorganization. The intensivist has certainly had a central role in guiding and managing this type of respiratory failure, together with the emergency medicine and pneumology, as well as the nursing of the critical respiratory patient. However, the emergency had forced to new organizations, as the creation of other sub intensive areas with integrated management [16].
If the ICU and the Emergency Medicine wards are the suitable setting for patients with severe acute respiratory failure and need for immediate stabilization, the sub-intensive Internal Medicine areas could be more effective as a step-down, for management of chronic patients with more comorbidities needing time to achieve a stable balance [16].
In Italy, Internal Medicine is considered a basic specialty: for a 32-bed module, there are 5 doctors and 17 nursing staff, with a consequent doctor/patient ratio of 0.15 and a nurse/patient ratio of 0.53 [17].
This proportion does not reflect the current needs and the variation of the type of hospitalized patient, with the risk of reduced medical and nursing staff, even more at the risk of burn-out.
After these evidence of a central role of Internal Medicine Unit during SARS-CoV-2 pandemic, the main Italian Internal Medicine societies, FADOI and SIMI (Italian Society of Internal Medicine), have presented to national and regional health institutions a document about the need for the implementation (structural, technological, staff) of Internal Medicine sub-intensive care areas throughout the national territory [18].
The pandemic has upset the way we work, but, in the same way, it has taught us how a future Internal Medicine ward should be: a ward at different levels of intensity (medium intensity and sub-intensive), managed by doctors (adequate number) with different skills and with suitable instrumentation for an integrated management of the internal complex patient. It is time to rethink and redeem Internal Medicine specialty.
Data Availability
Computerized medical records.
Code Availability
Not applicable.
References
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. Erratum in: Lancet. 2020 Jan 30. https://doi.org/10.1016/S0140-6736(20)30183-5.
Characteristics of COVID-19 patients dying in Italy. Available from: https://www.epicentro.iss.it/en/coronavirus/sars-cov-2-analysis-of-deaths. Accessed 20 Oct 2021.
FADOI COVID day. Available from: https://www.fadoi.org/press-room/fadoi-covid-day/. Accessed 30 Nov 2020.
Sanità e protezione civile (2020) Available from: https://www.mef.gov.it/covid-19/Sanita-e-Protezione-Civile/. Accessed 29 Sept 2020.
Epicentro, epidemiology for public health, COVID-19. Available from: https://www.epicentro.iss.it/en/.
Clinical spectrum of SARS-CoV-2 infection. Last Updated: October 19, 2021. Available from: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/.
Allinovi M, Parise A, Giacalone M, et al. Lung ultrasound may support diagnosis and monitoring of COVID-19 pneumonia. Ultrasound Med Biol. 2020;46(11):2908–17. https://doi.org/10.1016/j.ultrasmedbio.2020.07.018.
Magnani E, Mattei L, Paolucci E, Magalotti G, Giacalone N, Praticò C, Praticò B, Zani MC. Lung ultrasound in severe COVID-19 pneumonia in the sub-intensive care unit: beyond the diagnostic purpose. Respir Med Case Rep. 2020;31:101307. https://doi.org/10.1016/j.rmcr.2020.101307.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–83. https://doi.org/10.1016/0021-9681(87)90171-8.
Italia – percentuale di deceduti su ricoveri nel periodo compreso tra il 18 settembre 2020 ed il 2 giugno 2021. Dati COVIDSTAT, ISS INFN. Available from: https://covid19.infn.it/iss/.
Cogliati C, Ceriani E, Brambilla AM. When internal and emergency medicine speak to each other: organization in the time of COVID. Intern Emerg Med. 2020;15:891–2. https://doi.org/10.1007/s11739-020-02380-6.
Di Ciaula A, Palmieri VO, Migliore G, Portincasa P. COVID-19, internists and resilience: the north-south Italy outbreak. Eur J Clin Invest. 2020;50:e13299. https://doi.org/10.1111/eci.13299.
Sociedad Espa ̃nola de Medicina Interna. Registro SEMI COVID-19. Available from: https://www.fesemi.org/investigacion/proyectos/registro-semi-covid-19. Accessed 29 Nov 2021.
Martín-Garrido I, Medrano-Ortega FJ. Más allá de la infección aguda por SARS-CoV-2: un nuevo desafío para la Medicina Interna [Beyond acute SARS-CoV-2 infection: A new challenge for Internal Medicine]. Rev Clin Esp. 2022;222(3):176–179. Spanish. https://doi.org/10.1016/j.rce.2021.09.005.
Jamilloux Y, Lega J-C. La médecine interne dans la pandémie à SARS-CoV-2. Rev Méd Interne. 2020;41(5):301–302. ISSN 0248–8663. https://doi.org/10.1016/j.revmed.2020.04.003.
Agnoletti V, Russo E, Circelli A, Benni M, Bolondi G, Martino C, Santonastaso DP, Brogi E, PraticÒ B, Coccolini F, Fugazzola P, Ansaloni L, Gamberini E. From intensive care to step-down units: managing patients throughput in response to COVID-19. Int J Qual Health Care. 2021;33(1):mzaa091. https://doi.org/10.1093/intqhc/mzaa091.
Gazzetta ufficiale della repubblica italiana (GU Serie Generale n.225 del 24–09–1988). Available from: https://www.gazzettaufficiale.it/eli/gu/1988/09/24/225/sg/pdf. Accessed 24 Sept 1988.
Modello organizzativo e funzionale di un reparto di medicina interna, SIMI 22 settembre 2021. Available from: https://www.simi.it/news/modello-organizzativo-medicina-interna. Accessed 22 Sept 2021.
Author information
Authors and Affiliations
Contributions
Tortola, Magnani, and Sambo took care about editing and writing; Tortola, Giorgini, and Pazzaglini took care of data collection; Zani and Montaguti were the referents and creators of the wars subdivision.
Corresponding author
Ethics declarations
Ethical Approval
For this type of study, formal consent is not required.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Covid-19
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Tortola, D., Magnani, E., Giorgini, E. et al. Managing Complexity: The Experience of an Italian Internal Medicine Unit During the SARS-CoV-2 Pandemic, Looking to the Future. SN Compr. Clin. Med. 4, 233 (2022). https://doi.org/10.1007/s42399-022-01320-z
Accepted:
Published:
DOI: https://doi.org/10.1007/s42399-022-01320-z