
Abstract
The novel COVID-19 outbreak is a major public health challenge that quickly turned into an economic recession of great proportions. This pandemic poses a trade-off between health and the economy where social distancing, quarantines, and isolation shut down demand and supply chains across the USA. This paper analyzes the impact of COVID-19 on illness and death among older adults and communities of color with low socioeconomic status in New York City. To achieve this goal, fractional logit models are used to capture changes in the novel virus’ morbidity and mortality rates at the neighborhood level. Median income, race/ethnicity, age, household crowding, and socially interactive employment explained the disproportionate exposure and fatalities across the city. We also employ a variable related to telehealth/telemedicine to sustain that technology goods along with government intervention as a provider of social goods can ameliorate existing health disparities. There is a need for evidence-based data on the economic costs and social benefits of COVID-19 relief programs.
Similar content being viewed by others


Introduction
Infectious disease outbreaks spread rapidly across countries and get deep into nations reaching urban and rural communities, often affecting the most vulnerable populations across race/ethnicity, socioeconomic status, and age. We argue that COVID-19 had a strong negative impact on domestic economies worldwide and that the use of health technologies is instrumental in reversing this adverse trend. During the previous decade, the global pandemic caused by the influenza A (H1N1) strain reinforced a discussion about the control of future pandemics. A lot of studies emphasize that an effective global response is related to how healthcare technology is distributed, including vaccines and the support of low-income countries (Fineberg 2015; Ross et al. 2015). Furthermore, the role of health disparities and how pandemics most affect vulnerable populations was indicated from the H1N1 pandemic (Balter et al. 2010; Quinn et al. 2011). Large metropolitan concentrations provide infinite scenarios for the spread of pulmonary viruses such as the Severe Acute Respiratory Syndrome CoronaVirus 2 (SARS-CoV-2) which causes CoronaVirus Disease 2019 (COVID-19). The SARS-CoV-2 strain is a viral infection causing respiratory illnesses that can lead to death, particularly for older adults with pre-existing conditions (Guo et al. 2020; Hamed 2020; Driggin et al. 2020). This virus is highly transmissible from person to person through aerosolized respiratory droplets and may cause death in a median time of 18.5 days since the time of the infection among people with severe underlying medical conditions (Zhou et al. 2020). The first case of COVID-19 was identified in Wuhan, China, but the virus moved fast across the rest of the world, including the USA. Worldwide, the number of confirmed cases and the number of total deaths are both increasing at alarming rates, particularly affecting the developed countries plus India, Mexico, and Brazil. As of September 2020, the USA alone accounted for more than 23% of the diagnoses and about 21% of the deaths globally. New York, New Jersey, and Massachusetts are the states with the highest mortality rates per 100,000 inhabitants (Center for Disease Control and Prevention (CDC) 2020; Coronavirus Resource Center at John Hopkins University 2020).
The human cost of COVID-19 epitomizes the vulnerability of the social fabric and the fragility of the economic structure to health shocks. This epidemic started as a public health concern of unusual high morbidity and mortality rates and rapidly turned into a sui generis pandemic which induced a recession of sizable dimensions. COVID-19 poses a trade-off between disease and the economy: an increasing number of cases and deaths associated with this novel virus triggers social distancing and travel restrictions to decrease community transmission, slowing down economic activity. Restrictions on social and interpersonal contact have caused severe reductions in aggregate demand, high unemployment, and household income losses. Isolation and enforced quarantines have reduced the likelihood of new infections but caused severe aggregate demand and aggregate supply shocks across the US markets. In this trade-off between health and economics, medical technologies along with targeted government policy are key to reducing the negative impact of COVID-19 and can expedite economic recovery. The federal government mandated a nationwide ban on travel from or to China on January 31, 2020, even though the number of confirmed cases was very low. The World Health Organization declared COVID-19 a global epidemic on March 11, 2020, and recommended isolation and social distancing for people with mild respiratory symptoms, even for areas with no cases reported at the time (Cucinotta and Vanelli 2020). However, on March 20, 2020, the New York State government mandated closing down non-essential business triggering a drastic reduction in economic activity; however, public transportation remained open.
Similar to other epidemics, for this novel COVID-19 outbreak, big differences have been recorded in the impact across the various neighborhoods of a metropolis, such as New York City, that motivate our study. The NYC Department of Health and Mental Hygiene (DHMH) (2020) reported that the most affected zip codes were located in underserved communities of color, such as working-class Hispanics and African Americans with low income.
Health, Technology, and Socioeconomic Disparities of COVID-19
In a globalized society, a large proportion of the world population live in densely crowded urban areas connected by air travel, high-speed roads, and extensive mass transportation that fosters the spread of communicable diseases (Zheng et al. 2020). There is evidence of the emergence of inequities associated with the social determinants of health as a result of the COVID-19 epidemic (Gollust et al. 2020; Benitez et al. 2020; Baumer et al. 2020). Previous studies have established the multifactorial nature of disparities associated with the rise of epidemics, including those related to airborne diseases such as the Influenza A type H1N1 (Kumar et al. 2012; Quinn et al. 2011; Blumenshine et al. 2008). Parallel to the HIV epidemic (DelaCruz and Karpiak 2015; DelaCruz et al. 2020), income inequality, differentials in exposure, and social stratification in New York City (NYC) enabled the rapid spread of COVID-19 and exacerbated existing health disparities among vulnerable populations. Both epidemics asymmetrically affected low-income neighborhoods where Blacks, Hispanics, and older adults disproportionately face negative health outcomes and experienced comorbidities that increase their risk for COVID-19. Additionally, population density, mass transportation, and the examination of health inequalities using zip code data in the absence of demographic and socioeconomic cross-sectional information have been associated with COVID-19 (Chen and Krieger 2020; Zhao et al. 2020).
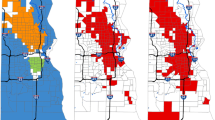
Cumulative morbidity and mortality indicators show that the number of positive COVID-19 cases was near 250,000, hospitalizations around 60,000, and confirmed deaths were almost 20,000 in NYC as of September 2020 (Fig. 1). The highest of these statistics occurred in low-income communities located in northern Manhattan, the Bronx, Brooklyn, and Queens. When stratifying COVID-19 cases, hospitalizations and deaths per 100,000 people by race/ethnicity, it is noticeable that these rates were higher among Hispanics and Blacks compared to Whites and Asians citywide (Fig. 2). Likewise, Fig. 3 shows a 7-day (date noted and the six prior days) moving average of the virus and antibody testing data; testing increased sharply throughout the timeframe of this study with an evident decline in the number of positive cases experienced during the last months. However, testing was higher in wealthy areas of Manhattan compared to any other borough in NYC. Hispanics experienced disproportionately negative impact regarding COVID-19 testing, cases, hospitalization, and deaths than any other ethnic/racial group nation- and citywide (Macias-Gil et al. 2020; Ojinnaka et al. 2020).

COVID-19 cumulative cases, hospitalizations, and deaths

COVID-19 cases, hospitalizations, and deaths by race/ethnicity

COVID-19 testing in NYC. Source: NYC Health (https://www1.nyc.gov/site/doh/covid/covid-19-data.page). Rate per 100,000 people
To investigate the relationship between the disease and its determinants, our model focuses on the first wave of COVID-19’s morbidity and mortality over the first 4 months spanning up to the beginning of July 2020 in NYC. Due to the lack of reliable demographic and socioeconomic data on COVID-19, we used neighborhood information from the DHMH and the US Census Bureau (United States Census Bureau (USCB) 2020) to estimate the impact of the virus on vulnerable populations across race/ethnicity, age, and socioeconomic status. Table 1 shows that the average number of cases per 100,000 was 2702 (SD = 904.1). The wealthy neighborhoods of Battery Park and TriBeCa were the least affected with cases below 700 per 100,000 people while the poorest, working-class zip codes of Bronx, Brooklyn, Staten Island, and Queens had more than 4000 events per 100,000 people. The mean number of deaths per 100,000 people was 214.0 (SD = 114.2) and the share of those who tested positive for the virus was 9.5% (SD = 3.6%). As expected, the average death rate and the percentage of positive cases were the lowest for Battery Park and TriBeCa and the highest for many zip codes in the abovementioned boroughs. Figure 4 displays scatter plots with positive correlations between morbidity rates and the share of Hispanics and Blacks per zip code with a coefficient of 31% and 30%, respectively. Conversely, the share of Asians and the number of COVID-19 cases in each zip code are negatively correlated with a coefficient of − 21%. These graphs suggest that Hispanics and Blacks were more likely to be exposed to the disease than Asians.

Scatter plots of morbidity rate and ethnicity. Source: US Census Bureau
Medical technologies have clearly bettered the quality of life of individuals and the population, but it is also known that it may contribute to health disparities (Timmermans and Kaufman 2020). The debate over the effects regarding the adoption of new technologies replicating socioeconomic status and social inequities in health is far from over (Weiss et al. 2018; Acemoglu 2002). The technology addresses disparities by improving the quality of medical care and healthcare delivery, which is important during public health crises and major epidemics. Health technologies associated with disease treatment and information have been instrumental in saving lives and improving quality of life (Gonzalez 2018; Williams et al. 2019). Furthermore, technological advances in health are driven by private investments that often contribute to escalating medical costs. Positive externalities arising from the creation of private medical goods can be complemented with the provision of social goods through government regulation and spending. The benefits of supplying public goods would outweigh the already high costs of the COVID-19 pandemic by far. Our study focuses only on the use of telemedicine within the group of technologies. Telemedicine, as the delivery of high-level medical care remotely, has emerged strongly during the COVID-19 pandemic. But the use of these new digital platforms where healthcare providers can continue serving their patients through virtual visits spotlights disparities induced by different degrees of familiarity with the use of internet. A lot of studies analyze data from healthcare systems in New York City with telemedicine services, and disparities in geography are identified (Chunara et al. 2021; Koziatek et al. 2020; Lam et al. 2021).
Methods
This study quantifies the impact of COVID-19 on morbidity and mortality in 178 zip codes across the 5 boroughs of NYC. We identify features that caused and magnified health disparities arising from differentials in exposure to the disease associated with income, race/ethnicity, type of profession, the average number of occupants per room, and the share of the employed population who used public transportation or carpool for their commuting. The econometric model predicts that disparate illness and death rates were shaped by gaps in income, household crowding, use of public transportation, and racial/ethnic differences similarly to other studies regarding pandemics (Blumenshine et al. 2008; Almagro and Orane-Hutchinson 2020). The empirical parsimonious model was based on a fractional logit model, which is used to directly model the fractional outcomes “percentage of cases” (morbidity rate) and “percentage of deaths” (mortality rate) across NYC zip codes. To ensure that the relative disease rates in NYC did not change drastically over the first wave within zip codes, the model was tested at different times within this period. We find that these results do not significantly differ from results for cumulative data as of July 9th 2020. The equations below show the dependent variables on the left-hand side representing the percentage of cases and deaths after the period of the first wave.
where \({\lambda }_{i}\) is the zip code mortality rate measured as the number of deaths per 100,000 population and \({p}_{i}\) is the zip code morbidity rate measured as the number of positive tests per 100,000 population on the left-hand sides of Eqs. (1), and (2) respectively. The right-hand side variables represent the determinants of illness and death associated with COVID-19. These two equations include the logarithm of the median income by zip code to analyze the socioeconomic status and geographic distribution of infection rates. COVID-19 was primarily associated to low-income individuals who live in those neighborhoods. Both models have a dummy variable for Black and Hispanic zip codes (minority neighborhoods) that takes the value 1 when either the proportion of Hispanics or Blacks is more than 29.1% and 24.3% respectively and zero otherwise. According to the US Census Bureau, these shares represent the total proportion of Hispanics and Blacks in NYC. We also include a binary variable for age by zip code to express where the share of people 65 years and older is more than 15%, i.e., the average number of this age group in NYC areas, and to account for the association between age and the number of deaths. Older adults are a risky group for COVID-19 because they usually experience chronic illnesses (such as hypertension, diabetes, or obesity) associated with in-hospital mortality (Cummings et al. 2020). The Center for Disease Control and Prevention (2020) reported that the median age for a person to die from a COVID-19-related infection was 71 years. The first wave of the pandemic went through a national lockdown, but many industries were able to manage working from home (Bartik et al. 2020). A variable expressing the share of people working in industries with either a high level of physical proximity and social engagement and/or low digital intensity that reflects the pace of technology was included to proxy the contribution of professions to COVID-19’s exposure. High-risk industries in our model include manufacturing, education, health social services, entertainment, art, recreation, food services, and wholesale and retail trade. Likewise, household crowding as the share of dwellings with more than 1.5 occupants per room and the share of the employed population who use public transportation or carpool for their commuting has been used in the model.
A demographic variable about gender is included in our model. We employ this variable to further explore gender differences on the COVID-19 exposure related to morbidity. The variable is defined as a dummy by indicating zip codes where the female population is the majority. Furthermore, as previous studies indicate, the proportion of female employees is lower in high teleworkable occupations compared to low-degree teleworkable occupations, and women along with minorities are more likely to become unemployed at the beginning of the pandemic (Gezici and Ozay 2020).
We use data from patients in a large healthcare system with robust telemedicine dimension, New York University Langone Health. At NYU Langone Health, virtual care services were provided to more than 90,000 patients at the beginning of the pandemic’s first wave in New York City. The data come from a recently published article, and we work with two periods (Chunara et al. 2021). The first period is from exactly 1 year before the outbreak, March 19 to April 30, 2019, while the second is from the same period in 2020 at the beginning of the pandemic in NYC, March 19 to April 30, 2020. We identify the zip codes with a change of more than 500 telemedicine patients between the two periods. For most of these zip codes, the change is more than 1% of the total population between the two periods. During the first period (2019), there are 354,133 patients with a NYC home zip code who accessed care. Out of these patients, only 900 accessed healthcare through telemedicine. During the second period (2020), there are 140,184 patients, with most of them being telemedicine patients. The telemedicine patients are 90,991 from all the NYC zip codes for March 19 and April 30, 2020.
Results
The regression results are presented in Table 2 and reported a strong significant (p > 0.01) relationship of these factors. Thus, people living in minority neighborhoods were 35.3% more likely to get sick (OR = 1.353, 95%CI = 1.220, 1.502) and 39.8% more likely to die (OR = 1.398, 95%CI = 1.184, 1.651) from the virus compared to non-minority neighborhoods. Similarly, the odds of exposure and dying from SARS-CoV-2 for zip codes, where the proportion of elderly people is above the average, is 19.9% (OR = 1.199, 95%CI = 1.098, 1.308) and 51.9% higher (OR = 1.519, 95%CI = 1.315, 1.754) respectively. Although the probability of prematurely dying increases with age, severe COVID-19 illness can lead to hospitalization and death among adults of any age.
People were 15.99 times (OR = 15.985, 95%CI = 2.311, 107.634) more likely to get exposed to the virus when the share of households with more than 1.5 occupants per room increases by 1% in a zip code. In most COVID-19-affected zip codes of NYC, the median household income fell below $25,000, the share of Blacks and Hispanics was higher than the average, and the percentage of adults 65 years and older was significant. As expected, the effect of income is significantly negative; low-income neighborhoods were more likely to be affected by the disease compared to higher-income zip codes that had 14.40% lower odds (OR = 0.856, 95%CI = 0.740, 0.990) of exposure to the disease and 44.1% lower odds (OR = 0.559, 95%CI = 0.473, 0.661) of death. Similarly, commuting is significant and negatively correlated with the cumulative number of infections during the first wave of COVID-19. In some studies, the use of subway and buses has been identified as a source for the fast spread of the virus (Sy et al. 2020; Fathi-Kazerooni et al. 2020). In our study, the variable commuting has a negative and significant coefficient. The variable used in our model expresses people’s commuting habits before the lockdown and perhaps is not representative of the percentage of people who used public transportation or carpool by zip code during the first wave of the pandemic and lockdown. Other possible explanations of this negative association have been discussed in other studies as well (Furth 2020; Wei et al. 2020). For instance, public transportation–dependent people adopt safety habits for commuting because traveling within the city seems dangerous with the fear of asymptomatic spread. Also, these people have a geographically limited and determined circle of contact.
A factor inducing a widespread of the virus is related to the type of profession and expresses an aspect of work-related inability to social distance other than commuting (Bartik et al. 2020; Beland et al. 2020). This is associated with the way workers perform their duties. Socially distanced work is more feasible in industries requiring more specialized skills and thus better paid. Unlike the variable commuting, the coefficient of the variable that expresses the proportion of employees in high-risk industries per zip code is significantly positive.
Finally, Table 3 summarizes the result across variable levels. In this new specification, minority neighborhood was stratified by Asian, Black, and Hispanic, showing a negative coefficient for Asians and positive otherwise. The lower rates of morbidity for Asians compared to Whites have been identified in the COVID-19 literature (Almagro and Orane-Hutchinson 2020). A possible explanation can be related to their socioeconomic status in New York. Perhaps vulnerable Asians in New York are less likely to get tested and treated, because of lack of health insurance and cultural barriers. This can be supported by Table 3 where the coefficient for Asians is insignificant and negative for the morbidity model, while for the mortality model the coefficient is positive and significant. This should be further explored in future studies. Age was also stratified into age categories; the share of older adults 65 + is the only variable with positive significant coefficients in the mortality model compared to other age groups. In the base model, we include only the highest level of household crowding (proportion of households with 1.5 occupants per room or more) as appears in the second specification. In the second specification, the gender variable expresses the proportion of the female population per zip code. There is an increased number of non-dummy variables for this specification. Contrary to our base model, the result of income is not significant, likely indicating the income differences across the other dependent variables’ strata. In the base model, the test decision of household crowding shows an odd ratio with a wide 95% confidence interval, which indicates high dispersion and a less certain conclusion. Moreover, these stratified results support the choice of variables and the initial arguments regarding health disparities.
Discussion
The human, social, and economic cost of COVID-19 is elevated. The macroeconomic losses attributable to COVID-19 are massive and continue to rise, which jeopardizes the wellbeing of individuals (Kawohl and Nordt 2020). This disease poses a trade-off between public health and economic activity; flattening the pandemic curve deepens the recession since the demand and supply chains are interrupted. Containment policies to avoid COVID-19 spread, such as social distancing and travel restrictions, have reduced the chances of economic recovery. Full or partial lockdowns are unsustainable in the long run and have produced unintended consequences such as higher illness and death rates and increases in poverty (Han et al. 2020). The response to the pandemic has been focused on restoring physical health and avoiding death, but mental health illnesses have been increasingly reported (Vindegaard and Benros 2020; Torales et al. 2020). This pandemic disproportionately affected communities of color, low-income individuals, and older adults in NYC. Due to its high transmissibility, the virus caused wide-ranging infection and fatality rates across the city very fast, triggering social distancing, quarantines, and self-isolation that shut down key economic sectors such as tourism, transportation, construction, education, and hospitality. Besides disability and death, the end point of COVID-19 was high unemployment rates and massive losses of income (Nicola et al. 2020). Data from the Federal Reserve Bank of St. Louis (2020) shows that the Gross Domestic Product declined 31.4%, unemployment reached 14.7%, and real personal income declined 8.7% in the second quarter of 2020. Likewise, projected COVID-19-related cost of hospitalization could range between $9.6 and $16.9 billion US dollars by the end of 2020 (Avalere 2020).
Starting even before the H1N1 pandemic, many studies discussed targeted policies and emphasized socioeconomic and racial/ethnic disparities (Quinn et al. 2011; Blumenshine et al. 2008; Almagro and Orane-Hutchinson 2020; Quinn and Kumar 2014). Our work supports this previous literature. Motivated by our results, community-based policy recommendations can be proposed. For instance, a culturally appropriate risk communication policy through trusted community channels at the beginning of the pandemic. Perhaps considering granting financial aid to specific social groups within a community and improving medical care for socially disadvantaged populations through a network of community-based clinics.
Additionally, our empirical model complements the existing literature by emphasizing that technology disparities are important. Policymakers at all levels should consider how to promote virtual healthcare services in underserved populations and thus minimize their cost during a novel pandemic. Health technologies in the form of testing, vaccines, therapeutics, and information can improve health status, reduce existing disparities, and be economically advantageous for society at large. Medical innovation is key to achieve lower disease rates and a safe reopening of the markets. Emerging medical advances arising from more expensive and complex procedures will greatly benefit the middle- to high-income populations, creating a barrier towards the poor in terms of affordability and access (Dzau and Balatbat 2018). Medical technologies in the form of pharmaceuticals, vaccines, or telehealth combined with the public provision of social goods can ameliorate the negative effects of an epidemic. Governance and regulation can foster the creation and distribution of technology as public goods, which is socially desirable and cost beneficial. For instance, telehealth, the use of telecommunication technologies to provide HIPAA (Health Insurance Portability and Accountability Act) compliant health services from remote locations, can deliver high-quality care, be used as a screening tool to avoid overcrowded clinical settings, and help decrease the exposure of first responders (medical staff), which can be critical during a health crisis. The use of digital technologies would ameliorate the impact on health systems caused by COVID-19. Yet, Hispanics, Blacks, and patients 65 years and older have lower odds of using telehealth, compared to other groups (Weber et al. 2020).
The race among pharmaceutical companies in the search for antiviral treatment and vaccines is showing promising results such as the emergency use of the Pfizer-BioNTech COVID-19 vaccine, which is being distributed in the USA through the inter-governmental Operation Warp Speed (US Food and Drug Administration 2020; US Department of Health and Human Services 2020). Due to the lack of diversity in vaccine and pharmaceuticals clinical trials, “the direct effects of genetic or biologic host factors remain unknown” (Chastain et al. 2020) across ethnicity, race, and age. The cost-savings and cost-benefits derived from the use of technology as social goods among vulnerable populations are relevant. The success of technologies depends on how effectively an innovation can be employed across members of society (Kruse et al. 2017). Due to state and city mandates, businesses are operating below capacity in NYC pushing up government programs such as unemployment insurance, Temporary Assistance for Needy Families or State- and local-funded Safety Net Assistance, food stamps, and Medicaid (Center for NYC Affairs 2020). Potential shortcoming of this study is that cross-sectional socioeconomic and demographic data on COVID-19 is not publicly available; moreover, the reported morbidity may be underestimated because children and young adults are more likely to be asymptomatic patients and not counted as positive cases. From the policy- and decision-making perspective, there is a need for more evidence-based data regarding the economic costs and social benefits of medical technologies and government intervention associated with the implementation of COVID-19 programs.
Conclusions
This study adds empirical data to the mounting evidence that racial/ethnic minorities are at elevated risk for COVID-19. The novel coronavirus pandemic compromised the health and welfare of millions of Americans and took the US economy to depths not experienced since the Great Depression. In NYC, economic activity was substantially reduced due to mandatory lockdowns and social distancing. Low-income neighborhoods, jobs associated with intense social interaction, the number of people living in an apartment, and the use of collective transportation are factors that promoted high rates of infection and death from COVID-19 among Hispanics, Blacks, and older adults. Furthermore, we exhibit that medical treatment with digital technologies can ameliorate the effect of the pandemic. Identifying disadvantaged communities and understanding the factors distressing them are instrumental in managing future crises as well. Understanding epidemiological and socioeconomic conditions that fostered the high rates of morbidity and mortality across race/ethnicity and geographical areas could help policymakers to manage the impact of future pandemics.
References
Acemoglu D. Technology and inequality. NBER Reporter Online, National Bureau of Economic Research; 2002. pp. 12–16, http://hdl.handle.net/10419/61816.
Almagro M, Orane-Hutchinson A. JUE Insight: the determinants of the differential exposure to COVID-19 in New York city and their evolution over time. J Urban Econ. 2020;103293:0094–1190. https://doi.org/10.1016/j.jue.2020.10329.
Avalere. 2020, retrieved from https://avalere.com/insights/COVID19-hospitalizations-projected-to-cost-up-to-17b-in-us-in-2020 on 8/30/2020.
Balter S, Gupta LS, Lim S, Fu J, Perlman SE. Pandemic (H1N1) 2009 surveillance for severe illness and response, New York, New York, USA, April-July 2009. Emerg Infect Dis. 2010;16:1259–64.
Bartik AW, Cullen ZB, Glaeser EL, et al. What jobs are being done at home during the COVID19 crisis? Evidence from firm-level surveys. Working Paper 27422. National Bureau of Economic Research; 2020. https://doi.org/10.3386/w27422.
Baumer Y, Farmer N, Premeaux TA, et al. Health disparities in COVID19: addressing the role of social determinants of health in immune system dysfunction to turn the tide. Front Public Health. 2020;8:559312. https://doi.org/10.3389/fpubh.2020.559312.
Beland LP, Brodeur A, Wright T. The short-term economic consequences of COVID19: exposure to disease, remote work and government response. IZA Inst Labor Econ. 2020. DP No. 13259, April 2020.
Benitez J, Courtemanche C, Yelowitz A. Racial and ethnic disparities in COVID19: evidence from six large cities. J Econ Race Policy. 2020;1–19. https://doi.org/10.1007/s41996-020-00068-9.
Blumenshine P, Reingold A, Egerter S, et al. Pandemic influenza planning in the United States from a health disparities perspective. Emerg Infect Dis. 2008;14(5):709–15.
Center for Disease Control and Prevention (CDC). 2020. Retrieved from https://covid.cdc.gov/ on 8/30/2020.
Center for NYC Affairs, retrieved from http://www.centernyc.org on 12/1/2020.
Chastain DB, Osae SP, Henao-Martinez AF, et al. Racial disproportionality in COVID clinical trials. New Engl J Med. 2020;383:e59. https://doi.org/10.1056/NEJMp2021971.
Chen JT, Krieger N. Revealing the unequal burden of COVID19 by income, race/ethnicity, and household crowding. US county versus zip code analyses. J Public Health Manag Pract. 2020. https://doi.org/10.1097/PHH.0000000000001263.
Chunara R, Zhao Y, Chen J, Lawrence K, Testa PA, Nov O, Mann DM. Telemedicine and healthcare disparities: a cohort study in a large healthcare system in New York City during COVID-19. J Am Med Inform Assoc. 2021;28(1):33–41. https://doi.org/10.1093/jamia/ocaa217.
Coronavirus Resource Center at John Hopkins University, retrieved from https://coronavirus.jhu.edu on 11/01/2020.
Cucinotta D, Vanelli M. WHO declares COVID19 a pandemic. Acta Biomed.2020; 91(1): 157–160. https://doi.org/10.23750/abm.v91i1.9397.
Cummings MJ, Baldwin MR, Abrams D, et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID19 in New York City: a prospective cohort study. Lancet. 2020;395(10239):1763–70. https://doi.org/10.1016/S0140-6736(20)31189-2.
DelaCruz JJ, Karpiak SE, Brennan-Ing. Health outcomes for older hispanics with HIV in New York City using the Oaxaca decomposition approach. GJ Health Sci. 2015;7(1):133–43. https://doi.org/10.5539/gjhs.v7n1p133.
DelaCruz JJ, Brennan-Ing M, Kakolyris A, Martinez O. The cost-effectiveness of mental health treatment in the lifetime of older adults with HIV in New York City: a Markov approach . Pharmacoeconomics – Open. 2020. https://doi.org/10.1007/s41669-020-00238-3.
Driggin E, Madhavan MV, Bikdeli B, et al. Cardiovascular considerations for patients, health care workers, and health systems during the COVID19 pandemic. J Am Coll Cardiol. 2020;75(18):2352–71. https://doi.org/10.1016/j.jacc.2020.03.031.
Dzau VJ, Balatbat CA. Health and societal implications of medical and technological advances. Sci Transl Med. 2018;10(463):eaau4778. https://doi.org/10.1126/scitranslmed.aau4778.
Fathi-Kazerooni S, Rojas-Cessa R, Dong Z, Umpaichitra V. Correlation of subway turnstile entries and COVID19 prevalence and deaths in New York City. Infect Dis Model. 2020. https://doi.org/10.1016/j.idm.2020.11.006.
Federal Reserve Bank of St Louis (FRED, 2020), retrieved from https://fred.stlouisfed.org on 8/25/2020.
Fineberg HV. Pandemic preparedness and response–lessons from the H1N1 influenza of 2009. N Engl J Med. 2015;370(14):1335–42. https://doi.org/10.1056/NEJMra1208802 (Erratum. In: N Engl J Med. 2015 Jan 8;372(2):197).
Furth S. Automobiles seeded the massive coronavirus epidemic in New York City. 2020, retrieved from https://marketurbanism.com/2020/04/19/automobiles-seeded-the-massivecoronavirus-epidemic-in-new-york-city/ on 10/10/20.
Gezici A, Ozay O. An intersectional analysis of COVID-19 unemployment. J Econ Race Policy. 2020;3:270–81.
Gollust SE, Vogel RI, Rothman A, et al. Americans’ perceptions of disparities in COVID19 mortality: results from a nationally-representative survey. Prev Med. 2020;141:106278. https://doi.org/10.1016/j.ypmed.2020.106278.
Gonzalez BD. Promise of mobile health technology to reduce disparities in patients with cancer and survivors. JCO Clin Cancer Inform. 2018;2:1–9. https://doi.org/10.1200/CCI.17.00141.
Guo YR, Cao QD, Hong ZS, et al. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID19) outbreak - an update on the status. Milit Med Res. 2020;7(11). https://doi.org/10.1186/s40779-020-00240-0.
Hamed MA. An overview on COVID19: reality and expectation. Bull Natl Res Center. 2020;44(1):86. https://doi.org/10.1186/s42269-020-00341-9.
Han E, JinTan MM, Turk E, et al. Lessons learnt from easing COVID19 restrictions: an analysis of countries and regions in Asia Pacific and Europe. Lancet. 2020. https://doi.org/10.1016/S0140-6736(20)32007-9.
Kawohl W, Nordt C. COVID19, unemployment and suicide. Lancet Psychiatry. 2020;7(5):389–90. https://doi.org/10.1016/S2215-0366(20)30141-3.
Koziatek CA, Rubin A, Lakdawala V, Lee DC, Swartz J, Auld E, Smith SW, Reddy H, Jamin C, Testa P, Femia R, Caspers C. Assessing the impact of a rapidly scaled virtual urgent care in New York City during the COVID-19 pandemic. J Emerg Med. 2020;59(4):610–8. https://doi.org/10.1016/j.jemermed.2020.06.041.
Kruse CS, Krowski N, Rodriguez B, et al. Telehealth and patient satisfaction: a systematic review and narrative analysis. BMJ Open. 2017;7:e016242. https://doi.org/10.1136/bmjopen-2017-016242.
Kumar S, Quinn SC, Kim KH, et al. (2012), “The impact of workplace policies and other social factors on self-reported influenza-like illness incidence during the 2009 H1N1 pandemic.” Am J Public Health. 2012;102(1):134–40.
Lam M, Leyden D, Platt SL. Geocode maps spotlight disparities in telehealth utilization during the COVID-19 pandemic in New York City. Telemed J E Health. 2021;27(3):251–3. https://doi.org/10.1089/tmj.2020.0297.
Macias-Gil R, Marcelin JR, Zuniga-Blanco B, et al. COVID19 pandemic: disparate health impact on the Hispanic/Latinx population in the United States. J Infect Dis. 2020;222(10):1592–5. https://doi.org/10.1093/infdis/jiaa474.
Nicola M, Alsafib Z, Sohrabic C, et al. The socio-economic implications of the coronavirus pandemic (COVID19): a review. Int J Surg. 2020;78:185–93. https://doi.org/10.1016/j.ijsu.2020.04.018.
NYC Department of Health and Mental Hygiene (DHMH). 2020. Retrieved from https://www1.nyc.gov/site/doh/covid/COVID19-data.page on 9/24/2020.
Ojinnaka CO, Adepoju OE, Burgess AV, et al. Factors associated with COVID-related mortality: the case of Texas. J Racial Ethn Health Disparities. 2020; 1–6. https://doi.org/10.1007/s40615-020-00913-5.
Quinn SC, Kumar S, Freimuth VS, et al. Racial disparities in exposure, susceptibility, and access to health care in the US H1N1 influenza pandemic. Am J Public Health. 2011;101(2):285–93.
Quinn SC, Kumar S. Biosecurity and bioterrorism: biodefense strategy, practice, and science. 2014;12(5). https://doi.org/10.1089/bsp.2014.0032.
Ross GPA, Growe SM, Tyndall MW. Planning of the next global pandemic. Int J Infect Dis. 2015;38:89–94.
Sy KTL, Martinez ME, Rader B, et al. Socioeconomic disparities in subway use and COVID19 outcomes in New York City. medRxiv. 2020; https://doi.org/10.1101/2020.05.28.20115949.
Timmermans S, Kaufman R. Technologies and health inequities. Ann Rev Sociol. 2020;46:583–602. https://doi.org/10.1146/annurev-soc121919-054802.
Torales J, O’Higgins M, Castaldelli-Maia JM, et al. The outbreak of COVID19 coronavirus and its impact on global mental health. Int J Soc Psychiatry. 2020;66(4):317–20. https://doi.org/10.1177/0020764020915212.
United States Census Bureau (USCB, 2020), retrieved from https://www.census.gov/quickfacts/newyorkcitynewyork on 10/01/2020
US Department of Health and Human Services, retrieved from https://www.hhs.gov/sites/default/files/strategy-for-distributing-covid-19-vaccine.pdf on 12/12/2020
US Food and Drug Administration, retrieved from https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/pfizer-biontech-covid-19-vaccine on 12/1/2020
Vindegaard N, Benros ME. COVID19 pandemic and mental health consequences: systematic review of the current evidence. Brain Behav Immunol. 2020;89:531–42. https://doi.org/10.1016/j.bbi.2020.05.048.
Weber E, Miller SJ, Astha V, et al. Characteristics of telehealth users in NYC for COVID-related care during the coronavirus pandemic. J Am Med Inform Assoc. 2020. https://doi.org/10.1093/jamia/ocaa216.
Wei JT, Liu YX, Zhu YC, et al. “Impacts of transportation and meteorological factors on the transmission of COVID19”, Int J Hyg Environ Health; 230:113610. DOI. 2020. https://doi.org/10.1016/j.ijheh.2020.113610.
Weiss D, Rydland HT, Oversveen E, et al. Innovative technologies and social inequalities in health: a scoping review of the literature. PLoS ONE. 2018;13(4): e0195447. https://doi.org/10.1371/journal.pone.0195447.
Williams F, Oke A, Zachary I. Public health delivery in the information age: the role of informatics and technology. Perspect Public Health. 2019;139(5):236–54. https://doi.org/10.1177/1757913918802308.
Zhao S, Zhuang Z, Ran J, et al. The association between domestic train transportation and novel coronavirus (2019-nCoV) outbreak in China from 2019 to 2020: a data-driven correlational report. Travel Med Infect Dis. 2020;33:101568. https://doi.org/10.1016/j.tmaid.2020.101568.
Zheng R, Xu Y, Wang W, et al. Spatial transmission of COVID19 via public and private transportation in China. Travel Med Infect Disease. 2020;34: 101626. https://doi.org/10.1016/j.tmaid.2020.101626.
Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID19 in Wuhan, China: a retrospective cohort study. Lancet. 2020; 395(10229). https://doi.org/10.1016/S0140-6736(20)30566-3.
Acknowledgements
We wish to thank the Editor and two anonymous referees for their comments and suggestions that helped us improve substantially the quality of our paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kakolyris, A., DelaCruz, J.J. & Giannikos, C.I. COVID-19, Race/Ethnicity, and Age: the Role of Telemedicine to Close the Gaps on Health Disparities. J Econ Race Policy 5, 241–251 (2022). https://doi.org/10.1007/s41996-021-00089-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41996-021-00089-y