
Abstract
Surgical retreatment is a predictable treatment option for teeth with post-treatment apical periodontitis. The main objective is to eliminate and prevent bacterial infection in the root canal system from causing an inflammatory reaction in the periradicular tissue.
Similar content being viewed by others


Indications
Apical periodontitis
Blocked root canals
Presence of posts, ledges, or broken instruments
Presence of foreign body in the periapical tissues
Radicular cyst
Extraradicular infection
Surgical exploration/diagnostics
Materials/instruments
Surgical operating microscope
Local anesthesia
Epinephrine
Cotton pellet
Aluminum chloride or ferric sulfate
Mineral trioxide aggregate (MTA)
Ultrasonic tips
Surgical burs
Saline
Surgical sutures
Procedure
To choose the treatment option a thorough clinical and radiographic examination, including adjacent and opposing teeth, should be performed. Along with the other basic assessments, following considerations should also be made during surgical retreatment planning [1]:
Technical considerations
Surgical retreatment should be considered when orthograde retreatment fails to control the infection or cannot be undertaken due to blocked canals caused by dystrophic calcifications or iatrogenic errors such as ledges, broken instruments and presence of posts (Fig. 1).

a Radiograph of the upper left first molar with a fractured instrument in the mesiobuccal root diagnosed with symptomatic apical periodontitis. b Immediately postoperatively. c A 1-year follow-up
Biological considerations
Surgical retreatment is indicated when a persistent infection is suspected after root canal treatment [2]. The presence of extraradicular infection [3], radicular cyst or a foreign body in the periapical tissues can cause endodontic failure by triggering an inflammatory response [4]. A local deep pocket is also an aggravating factor for the prognosis. As part of the diagnostic examination, a surgical exploration may be an alternative for excluding a vertical root fracture from a sinus tract formation originating from an endodontic lesion (Fig. 2).

a Upper right second premolar with a deep pocket located buccal. b An exploration is done to inspect the root surface. c A vertical fracture line seen after removing the soft tissue and staining with methylene blue
Anatomical considerations
The accessibility of the site of infection should be judged preoperatively. Periapical radiographs should be carefully evaluated in different angulations for planning and performing treatment (Fig. 3).

An upper molar with a symptomatic apical periodontitis. a The radiographs show a periapical radiolucency and fractured instrument in the apical third of the mesiobuccal root. b With a mesial eccentric radiographs, the root-filled canal in the mesiobuccal root moves from the X-rays, not centralized in the canal, indicating a second untreated canal
In the lower jaw, proximity to the mandibular nerve and/or a thick cortical bone buccal to the tooth may limit the accessibility. In upper jaw, the accessibility to the palatal root is limited surgically especially for the second maxillary molars.
Surgical treatment on teeth with apex or a periapical lesion in close apposition to the maxillary sinus should be carefully performed.
Medical considerations
There are no absolute medical contraindications to endodontic surgery. However, there are several medical conditions and medications that cause a depressed immune system, where surgical intervention is contraindicated until white blood cell count and antibody levels become normal. Patients with increased risk for bleeding need special attention. Patients with haemophilia or impaired liver function should only be treated after consultation and in agreement with the patient’s physician. Medication with antiplatelet and anticoagulant agents increase the bleeding time intra- and postoperatively. Surgical treatment is possible in most cases but need certain treatment protocols.
Endodontic surgery technique
Today’s state-of-the-art in surgical endodontic retreatment is a minimal invasive microsurgical approach which is described in the following:
-
To gain access to the root, a horizontal incision is given either including the papilla or cutting through the base of papilla. Submarginal incision is often recommended to minimize the risk of gingival recession in the esthetic zone. Subsequently, a full-thickness flap is raised.
-
The highly vascularized granulation tissue in the bone crypt is removed.
Hemostasis is achieved using local anesthesia containing epinephrine. Aluminium chloride or ferric sulfate can also be used for controlling bone crypt hemorrhage. If more severe bleeding occurs, electrocauterization may be considered.
-
Root resection is performed to eliminate infected ramifications, lateral canals and contaminated dentin.
A root resection of 3 mm (mm) apically is sufficient to remove most of the infected ramifications and lateral canals. It is performed in a 90° angle to the long axis of the root. This minimizes any leakage that can occur through cut dentinal tubules. Retrograde root-end cavities are prepared by ultrasonic tips in exposed canal orifices. MTA is used for root-end filling (Fig. 4).
Fig. 4 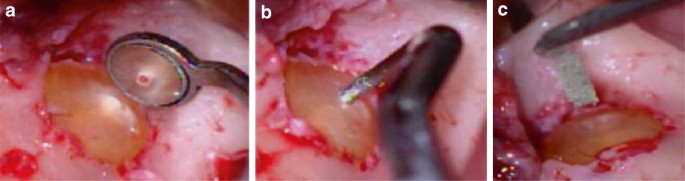
Single-rooted maxillary incisor treated by surgical retreatment using microsurgical technique. a The resected root and canal with gutta-percha seen in the micro-mirror and microscope (×6) with good haemostatic control. b Retrograde preparation with a contra-angled ultrasonic tip (3 mm). c Application of the retrograde filling (MTA)
-
The wound surface is thoroughly irrigated with the saline and the wound is closed using surgical sutures for optimal healing. Surgical sutures should hold the edges of a flap in apposition until the wound has healed sufficiently to withstand the normal functional stresses and resist reopening.
Resorbable or non-resorbable threads in diameters 5–0 or 6–0 and three-eighths reverse-cutting or tapered needle are used. The sutures are removed after 7–14 days.

Pitfalls and complications
-
Pain and swelling after surgical treatment.
-
Secondary infection of the surgical site.
-
An insult to blood vessels.
-
Lack of control of possible coronal leakage and carious lesions under restorations.
-
Limited access to the root canal full length.
-
Limited possibility to use chemical disinfection.
References
Kvist T (ed) (2017) Apical periodontitis in root-filled teeth surgical retreatment. https://doi.org/10.1007/978-3-319-57250-5_7
Nair PN (2006) On the causes of persistent apical periodontitis: a review. Int Endod J 39(4):249–281
Ricucci D, Siqueira JF Jr (2008) Apical actinomycosis as a continuum of intraradicular and extraradicular infection: case report and critical review on its involvement with treatment failure. J Endod 34(9):1124–1129
Stockdale CR, Chandler NP (1988) The nature of the periapical lesion—a review of 1108 cases. J Dent 16(3):123–129
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Jonasson, P., Ragnarsson, M.F. Surgical endodontic retreatment. Clin Dent Rev 2, 17 (2018). https://doi.org/10.1007/s41894-018-0027-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s41894-018-0027-3