
Abstract
Purpose
With the day-to-day advances in science and technology, perioperative practices are also evolving and include high-quality evidence that improves surgical outcomes. We inspected the perioperative trends in major elective gynecological and oncological surgeries performed by various surgeons practicing in the field of gynecological and oncological surgery in India.
Methods
A ‘39-questions’ questionnaire was developed on the basis of the recently published ERAS society recommendations for the major gynecological and oncological surgeries using Google Forms© and was sent to the various consultants practicing gynecology or surgical oncology across major cancer centers across India. The results of the first 100 responses were noted and analyzed.
Results
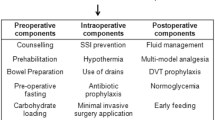
Response rate was 83.3%. 83 surgical and 17 gynecological oncologists participated from 59 different institutions. It was observed that many surgeons were adhering to the latest evidence-based practices like pre- and postoperative education, prehabilitation, DVT prophylaxis, use of MIS, multimodal analgesia, and regular audit. However, there were also some areas where traditional practices were still prevalent which included mechanical bowel preparation, keeping patients fasting overnight, no carbohydrate loading, unnecessarily keeping IP drains and NG tubes for longer times, and refraining from starting orally within 24 h of surgery.
Conclusions
While most Indian oncological surgeons were adhering to the latest evidence-based practices, they were still lagging behind in certain aspects and traditional practices were being carried forward. With increasing awareness among surgeons, the latest guidelines should be followed for better surgical results.
Similar content being viewed by others


References
Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg. 2017;152:292–8.
Nelson G, Altman AD, Nick A, et al. Guidelines for pre- and intra-operative care in gynecologic/oncology surgery: enhanced Recovery After Surgery (ERAS®) society recommendations–Part I. Gynecol Oncol. 2016;140:313–22.
Nelson G, Altman AD, Nick A, et al. Guidelines for postoperative care in gynecologic/oncology surgery: enhanced Recovery After Surgery (ERAS®) society recommendations–part II. Gynecol Oncol. 2016;140:323–32.
Nelson G, Bakkum-Gamez J, Kalogera E, et al. Guidelines for perioperative care in gynecologic/oncology: enhanced Recovery After Surgery (ERAS) Society recommendations -2019 update. Int J Gynecol Cancer. 2019;29(4):651–68.
Kehlet H, Buchler MW, Beart RW Jr, et al. Care after colonic operations is it evidence-based? Results from a multinational survey in Europe and the United States. J Am Coll Surg. 2006;202(1):45–54.
Lassen K, Hannemann P, Ljungqvist O, et al. Patterns in current perioperative practice: survey of colorectal surgeons in five northern European countries. BMJ. 2005;330(7505):1420–1.
Arsalani-Zadeh R, Ullah S, Khan S, et al. Current pattern of perioperative practice in elective colorectal surgery; a questionnaire survey of ACPGBI members. Int J Surg. 2010;8(4):294–8.
Kisielewski M, Rubinkiewicz M, Pędziwiatr M, et al. Are we ready for the ERAS protocol in colorectal surgery? Wideochir Inne Tech Maloinwazyjne. 2017;12(1):7–12.
Angioli R, Plotti F, Capriglione S, et al. The effects of giving patients verbal or written pre-operative information in gynecologic oncology surgery: a randomized study and the medical-legal point of view. Eur J Obstet Gynecol Reprod Biol. 2014;177:67–71.
Silver JK, Baima J. Cancer prehabilitation: an opportunity to decrease treatment-related morbidity, increase cancer treatment options, and improve physical and psychological health outcomes. Am J Phys Med Rehabil. 2013;92:715–27.
Minnella EM, Bousquet-Dion G, Awasthi R, et al. Multimodal prehabilitation improves functional capacity before and after colorectal surgery for cancer: a five-year research experience. Acta Oncol. 2017;56:295–300.
Cao F, Li J, Li F. Mechanical bowel preparation for elective colorectal surgery: updated systematic review and meta-analysis. Int J Colorect Dis. 2012;27:803–10.
Dahabreh IJ, Steele DW, Shah N, et al. Oral mechanical bowel preparation for colorectal surgery: systematic review and meta- analysis. Dis Colon Rectum. 2015;58:698–707.
Pineda CE, Shelton AA, Hernandez-Boussard T, et al. Mechanical bowel preparation in intestinal surgery: a meta-analysis and review of the literature. J Gastrointest Surg. 2008;12:2037–44.
Slim K, Vicaut E, Launay-Savary M-V, et al. Updated systematic review and meta-analysis of randomized clinical trials on the role of mechanical bowel preparation before colorectal surgery. Ann Surg. 2009;249:203–9.
Smith MD, McCall J, Plank L, et al. Preoperative carbohydrate treatment for enhancing recovery after elective surgery. Cochrane Database Syst Rev. 2014;8:CD009161.
Roig JV, Garcia-Fadrique A, Redondo C, et al. Perioperative care in colorectal surgery: current practice patterns and opinions. Colorectal Dis. 2009;11:976–83.
Sweetland S, Green J, Liu B, et al. Duration and magnitude of the postoperative risk of venous thromboembolism in middle aged women: prospective cohort study. BMJ. 2009;339:b4583.
Bratzler DW, Dellinger EP, Olsen KM, et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Surg Infect. 2013;14:73–156.
Darouiche RO, Wall MJ, Itani KMF, et al. Chlorhexidine–alcohol versus povidone-iodine for surgical-site antisepsis. N Engl J Med. 2010;362:18–26.
Nelson R, Edwards S, Tse B. Prophylactic nasogastric decompression after abdominal surgery. Cochr Database Syst Rev. 2007;8:CD004929.
Prete A, Yan Q, Al-Tarrah K, et al. The cortisol stress response induced by surgery: a systematic review and meta-analysis. Clin Endocrinol. 2018;89:554–67.
Walker JL, Piedmonte MR, Spirtos NM, et al. Laparoscopy compared with laparotomy for comprehensive surgical staging of uterine cancer: gynecologic Oncology Group study LAP2. J Clin Oncol. 2009;27:5331–6.
Cutillo G, Maneschi F, Franchi M, et al. Early feeding compared with nasogastric decompression after major oncologic gynecologic surgery: a randomized study. Obstet Gynecol. 1999;93:41–5.
Wischmeyer PE, Carli F, Evans DC, et al. American Society for enhanced recovery and perioperative quality initiative joint consensus statement on nutrition screening and therapy within a surgical enhanced recovery pathway. Anesth Analg. 2018;126:1883–95.
Dawes AJ, Sacks GD, Russell MM, et al. Preventable readmissions to surgical services: lessons learned and targets for improvement. J Am Coll Surg. 2014;219:382–9.
Duzgun O. Evaluation of enhanced recovery after following a surgical protocol for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for peritoneal carcinomatosis. Med Arch. 2019;73(5):331–7.
Bisch SP, Wells T, Gramlich L. Enhanced recovery after surgery (ERAS) in gynecologic oncology: system-wide implementation and audit leads to improved value and patient outcomes. Gynecol Oncol. 2018;151:117–23.
Author information
Authors and Affiliations
Contributions
The concept and design of the study were created by both authors. Literature search, data acquisition, and analysis were performed by both. The manuscript was prepared by Ankit Dhiman. The same was edited and reviewed by M D Ray. Overall responsibility and corresponding author is M D Ray.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflict of interest.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Dhiman, A., Ray, M.D. Enhanced Recovery After Gynecological/Oncological Surgeries: Current Status in India. Indian J Gynecol Oncolog 18, 127 (2020). https://doi.org/10.1007/s40944-020-00458-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40944-020-00458-9