
Abstract
This review of the literature examines the problem of suicide and bullying from a developmental perspective with a focus on the unique characteristics of adolescence that may contribute to the bullying-suicide link. Adolescence is a time of peak physical health, yet can be a period of risky behavior and heightened emotionality. In this literature review, it is argued that a number of developmental factors leave adolescents especially vulnerable to suicidal behavior following exposure to bullying. This review highlights the importance of developmental factors in understanding the bullying-suicide link during adolescence. Adolescence, with an increase in emotionality, risk-taking, and an increased focus on peer relationships, is an at-risk period for the development of suicidality following exposure to bullying. Also highlighted are gender differences, special challenges facing LGBTQ adolescents, and recommendations for intervention and prevention.
Similar content being viewed by others


Introduction
Throughout this article, a review of the literature on the relationship between bullying and suicide will be undertaken with an emphasis on the uniqueness of adolescence and the developmental factors associated with this age group. To provide context, we first discuss recent statistics on suicide. In 2014, 42,773 people died by suicide at a rate of 13.4 per 100,000 (Drapeau and McIntosh 2015). Suicide, while ranking 10th in causes of death in the United States, is the 2nd leading cause of death for those classified as young (ages 15–24). For youth ages 15 through 24, a suicide occurs every 1 h and 44 min, though this timeframe decreases to 1 h and 35 min if those below the age of 15 are considered (Drapeau and McIntosh 2015). Globally, approximately one million people die annually of suicide, which is a rate of 16 per 100,000. That is one death every 40 s and is estimated to increase to one death every 20 s by 2020 (Suicide Statistics 2016). The international suicide rate for adolescents in countries who provide information to the World Health Organization (WHO) is 7.4 per 100,000 (based on 90 of 130 WHO members; Wasserman et al. 2005) and it is acknowledged that youth suicide rates are increasing at the greatest rate (Suicide Statistics 2016).
Although these numbers emphasize the far reaching impact of suicide, the following case studies are important to consider in order to highlight the very personal experience of suicide for individual adolescents, their families, and their communities. In the Fall of 2010 in New Jersey, USA, Tyler Clementi was a freshman at Rutgers University when he was outed as gay via cyber bullying (Ebbels 2010; Star Ledger Staff 2011). Shortly afterwards, he died by suicide. Tyler had returned to his dorm room one night with another man. There Tyler and the other man engaged in kissing which was broadcast by Tyler’s roommate, Dharun Ravi, using a webcam onto Twitter. When this became known to Tyler, he jumped to his death off of the George Washington Bridge, a suspension bridge connecting the states of New York and New Jersey. Following Tyler’s suicide, Ravi was convicted of numerous counts, including invasion of privacy, bias intimidation, and hindering prosecution. Ravi received 30 days in jail, 3 years of probation, 300 h of community service, a $10,000 fine and counseling on cyberbullying following his conviction (Zernike 2012).
Olivia Perryman, age 14, died by suicide in January 2016. Olivia was a resident of York Township, Pennsylvania, USA (Mason 2016). She had been the victim of cyberbullying, including “catfishing” which involves using a false identity online to befriend and trick. Olivia was also dealing with the loss of her father to a heroin overdose and her mother’s addiction issues. Child services had intervened due to Olivia’s repeated attempts to run away at the behest of the cyberbully, who lured her into believing she was talking to a young boy who cared for her.
Olivia Penpraze was 19 years of age when she made her final of several suicide attempts (Smith 2015). Olivia was a resident of Melbourne, Australia and had attempted suicide three times before her eventual death. Olivia documented her struggle with depression and suicidality on a video blog. Her final message was over 5 min long and documented her depression and suicide attempts on index cards held up for the audience to see. Olivia attributed her negative view of herself as stemming from the bullying she experienced when she was younger.
The above three cases, as well as a number of others, have attracted international attention to the link between bullying and suicide during adolescence. Research supports the anecdotal evidence derived from these tragic case studies, regarding the link between being the victim of peer bullying and suicide. Although bullying is not typically cited as the sole cause of suicidal risk, it clearly increases the likelihood of suicidal thoughts and attempts, especially in the presence of other social and psychological risk factors. Several review articles and large-scale studies exist, and they have carefully highlighted the devastating and finite public health threat of suicide as well as the links between bullying, victimization, and suicide (e.g., Holt 2015; Kim and Leventhal 2008; Reed et al. 2015). However, reviews of the bullying and suicide link have not focused specifically on the unique developmental considerations of adolescence. Adolescence is a time of multiple social and psychological transitions, characterized by changes to the family, school and home domains (Eccles et al. 1996, 2003a; Kloep et al. 2016). There is a heightened focus on peer relationships and peer acceptance (Brown and Braun 2013; Brown and Larson 2009); thus threats to one’s peer experiences and status during this time may be particularly challenging. These social and psychological transitions occur in the context of rapid, uneven brain development, leaving adolescents especially vulnerable to react to social infractions with impulsivity and short-sightedness (Shulman et al. 2016; Steinberg 2008). Suicide is the third leading cause of death among individuals aged 10–14, and the second leading cause of death for individuals aged 15–34 (National Center for Injury Prevention and Control. Center for Disease Control and Prevention 2015).
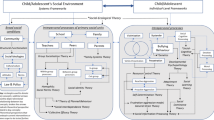
With the above issues in mind, the primary focus of the current review is to examine associations between bullying, psychopathology, and suicidal behavior during the unique developmental period of adolescence. First, the social, psychological, and cognitive changes of adolescence that are most relevant for a discussion of suicide from a developmental perspective will be reviewed using an integrated bioecological (Bronfenbrenner 1979; Bronfenbrenner and Morris 1998) and social-cognitive perspective (e.g., Bandura 1977, 1986; Eccles et al. 1993; Guerra and Huesmann 2004) that acknowledges the reciprocal influence of different levels of social and environmental systems on the adolescent’s changing individual characteristics and perspective. Next, after defining bullying and comparing and contrasting it to the overlapping construct of aggression, the relationship between bullying, psychopathology, and suicidal behavior during adolescence will be examined, as will the role of gender and sexual orientation in understanding bullying and suicide during adolescence. Finally, recommendations for future research and prevention will be made.
Adolescent Development
As adolescence begins, youth experience rapid biological, social, cognitive, and psychological transitions (e.g., Benner 2011; Dorn and Biro 2011; Lord et al. 1994; Simmons and Blyth 1987). Puberty, changes in peer and family relationships, and increases in cognitive and emotional sophistication occur at the same time that adolescents move from elementary to secondary school settings. This school transition exposes young adolescents to a wide range of new social and educational experiences at the same time as when many other aspects of their physical and psychological experiences are changing. If these new experiences are not well matched to adolescents’ developmental needs, negative social and psychological sequelae may occur (Eccles et al. 1991, 1993; Goldstein et al. 2005). As discussed in detail elsewhere (Eccles et al. 1993; Gillen-O’Neel and Fuligni 2013; Grolnick and Raftery-Helmer 2015; Roeser and Eccles 1998), adolescents do best socially and academically when their schools provide them with a context to engage actively and autonomously in their own learning, in a supportive and warm climate. Unfortunately, secondary schools do not uniformly provide adolescents with this type of experience. Despite contextual challenges inherent in the multiple transitions of early adolescents, most adolescents eventually adapt; however unfortunately some have a more difficult time.
Social Relationships
Another key social transition during adolescence is the shift in peer relationships, which take on increased salience during the early adolescent years (Buhrmester 1996; Levitt et al. 1993; Brown and Braun 2013; Brown and Larson 2009). Adolescents spend greater amounts of time with their peers, and begin to develop intimate peer relationships characterized by by trust, loyalty, and disclosure (Berndt and Perry 1990; Rubin et al. 2005). At the same time, exposure to victimization typically peaks in middle school (Olweus 1993; Whitney and Smith 1993), and students’ perceptions of school safety typically decline from elementary to middle school (Astor et al. 2001). The type of bullying that youth are exposed to evolves as well, with an increasing likelihood of victimization by means of cyber or relational forms (Barlett and Coyne 2014; Card et al. 2008). These forms of aggression, described in further detail below, tend to be more socially complex and challenging to navigate, as compared to the direct, physical and verbal forms of aggression that are more likely to present at earlier ages. Further, interest in romantic relationships begins during adolescence, with some forging new romantic and/or sexually intimate relationships. Dilemmas surrounding these newly developing romantic relationships and sexual interests begin to surface and can present substantial challenges for youth as they learn how to navigate these issues (Crouter and Booth 2006; Furman et al. 1999). These relationships are also subject to challenges with aggressive behavior and violence (e.g., Goldstein 2011; Lundgren and Amin 2015; Smith et al. 2015).
Family relationships are also dynamic during adolescence. Parent-adolescent conflict increases through early to mid-adolescence (Laursen et al. 1998), as adolescents and parents renegotiate issues regarding adolescent autonomy and behavior (Smetana 1995, 2000; Smetana and Asquith 1994). Adolescence is typically characterized by increasing autonomy from direct parental supervision and instruction (McElhaney et al. 2009; Zimmer-Gembeck et al. 2011). Teens desire this increased autonomy, and over time believe an increasing number of behaviors to be under their own jurisdiction rather than up to the rules and regulations of their parents or other adults (Darling et al. 2008; Smetana and Asquith 1994). Autonomy, to some extent at least, is desirable; adolescents who believe their parents to be too intrusive or restrictive are at risk for high susceptibility to peer pressure, associating with delinquent peers, and for engaging in problem behavior (Goldstein et al. 2005). However there are limits to the benefits of autonomy provision. When too much autonomy and freedom are given to teens, this also places them at an increased risk for problem behaviors and negative peer association (Dishion et al. 2003, 2004). Thus, parents must find a place of ever-changing balance between just enough autonomy and freedom to satisfy adolescents’ changing needs for self-direction and independence, without allowing for too much autonomy as to place their children at risk (Goldstein et al. 2005; Racz and McMahon 2011; Tilton-Weaver et al. 2013). This is not necessarily an easy balance to find, and it is one that ideally is adjusted with the social and developmental changes of the adolescent and her/his context. This ideal balance becomes even more complicated when adolescents struggle with behavioral or mental health challenges. If parents attempt to increase monitoring after they become knowledgeable about their child’s externalizing behavioral problems, adolescents may become even more reluctant to confide in their parents because they perceive this increased interest as an intrusion. Thus, they may be less likely to share emotional or psychological challenges that arise with their parents. Conversely, internalizing challenges can be less visible than externalizing concerns, thus parents may not have the same opportunity to reach out to their children who may be experiencing these types of difficulties.
These social transitions, coupled with increased cognitive sophistication and the drastic physical changes of puberty, create a situation of heightened vulnerability for young adolescents. Academic achievement and motivation decline (Eccles and Midgley 1989; Eccles et al. 2003b), behavioral and mental health problems increase (Graber and Sontag 2009; Loeber and Farrington 2000), and the peer-related challenges that youth face become more complex (Archer and Coyne 2005). Although many adolescents rebound from these problems, many do not. For some, the transition to adolescence marks the start of downward trajectories of achievement and behavioral and mental health (Eccles 2004; Lerner and Steinberg 2004; Wigfield et al. 2006), both of which increase the risk for suicidal thoughts and behaviors (Lewis et al. 1988; Evans et al. 2004).
Cognitive and Physiological Changes
Adolescence also brings with it a unique juxtaposition of an expanded scope of social and societal exploration and access coupled with increased drive for sensation seeking, impulsivity, and sensitivity to social cues. The combination of increased social access with cognitive and neurological immaturity paves the way for adolescents to engage in high-risk, impulsive behaviors (Shulman et al. 2016; Steinberg 2008). Of particular importance is the fact that, while adolescence brings on the occurrence of more abstract logic, for some it is also a period of enhanced self-focus or egocentrism (Elkind 1967). Egocentrism has been tied to depressive disorder (Baron and Hanna 1990), and the connection between egocentrism and suicidality was discussed by Everall et al. (2005). Specifically, the authors discuss how egocentrism can easily lead to negative feelings, criticisms, and low self-worth. Furthermore, the instinctual and emotional areas of the brain (i.e., limbic system) develop at a faster rate than the rational, emotional regulation areas of the brain (i.e., prefrontal cortex). Recent research has shown that the asynchronous development of the sensation and reward-seeking brain system with the impulse-regulating brain system is most mismatched during early and middle adolescence, increasing the likelihood of risky, unregulated behavior during this time period (Shulman et al. 2016). Due to these cognitive and psychological developments, coupled with the above discussed social changes and the hormonal changes associated with puberty, it is not uncommon for adolescence to be a time of heightened mood swings that are unfettered by the more regulated control of adulthood (Larson et al. 1980; Larson et al. 2002). Dahl (2004) described adolescence as akin to “starting turbo-charged engines with an unskilled driver” (Dahl 2004, p. 17). This creates a “health paradox” in which adolescence can be seen as a period of strength and resilience in most domains and yet morbidity and mortality increase. This increase in morbidity and mortality is not the result of illnesses such as cancer or heart disease, but it is rather a result of “difficulties in the control of behavior and emotion” (Dahl 2004, p. 3).
It is important to note that adolescents, as compared to younger children, have improved with regard to emotion regulation (Zeman et al. 2006). For example, the use of suppression diminishes with increasing age (Gullone et al. 2010). Suppression as a form of emotional regulation is associated with the experience of less positive affect (Gross and John 2003). Furthermore, McRae et al. (2012) examined the development of emotion regulation in late childhood, adolescence, and early adulthood. They found that, from late childhood through early adulthood, there is an increase in the ability to perform cognitive reappraisal. Reappraisal as an emotional regulation strategy is more common in adulthood and is associated with more positive affect compared to suppression (Gullone et al. 2010). However, as Zeman et al. (2006) point out, while shame and pride are present during childhood, they increase in intensity during adolescence. This may serve to heighten the sensitivity to social evaluation. With this heightened sensitivity to the evaluations of others, it may be that adolescence becomes a time of vulnerability to peer victimization.
These are not the only changes that are happening throughout this period, however. Throughout adolescence, the brain is undergoing increases in connectivity that influence how the various structures of the brain work in tandem. Evidence also suggests that during this period, teens have heightened emotionality due to a lack in regulation as a side-effect of differential development (Casey et al. 2010). Hormonal changes are also occurring at this time period, tied to sexual maturation and to stress responses, and can have profound impacts on the brain and behavior (Blakemore et al. 2010). These changes in the brain are related to the sleep cycle as well, ultimately increasing the likelihood of sleep deprivation because the increased wakefulness during the night does not coincide well with typical school schedules (Hansen et al. 2005). Sleep deprivation, in turn, places adolescents at an increased risk of depression and anxiety (Fuligni and Hardway 2006), and further taxes regulatory processes for thoughts and emotions (Baum et al. 2014).
Impulsivity and Suicide Risk
Considering the increase in impulsivity present in adolescence, the question of whether or not there is a relationship between impulsivity and suicidal behavior must now be addressed. Bridge et al. (2006), in a review of risk factors for suicidal behavior, discussed the role of impulsive aggression. Impulsive aggression, defined by Bridge et al. (2006, p. 378) as “a tendency to react to frustration or provocation with hostility or aggression,” has been linked to suicidal behavior by a number of studies (e.g., Apter et al. 1995; Beautrais et al. 1999; Bridge et al. 2006). Impulsivity has further been linked to suicidal behavior in numerous studies, though was usually mediated by a number of other risk factors (e.g., Kashden et al. 1993; Beautrais et al. 1999). More recently, Gvion and Apter (2011) reviewed the literature on aggression, impulsivity, and suicidal behavior. They concluded that, while there are inconsistencies and confusing findings given the interrelationship between aggression and impulsivity, the relationship between aggression, impulsivity, and suicidality is well-established. Ortin et al. (2012) examined the relationship between sensation seeking in adolescence and suicidality. Sensation seeking was related to both suicidal ideation and suicide attempt, even after controlling for depression and substance use.
In recognition of the link between impulsivity and suicide, the American Association of Suicidology includes “Recklessness” on the “IS PATH WARM” mnemonic that was devised to aid practitioners in identifying suicidal patients (Juhnke et al. 2007). Recklessness is defined by the question “does the client act recklessly or engage in risky activities, seemingly without thinking or considering potential consequences” (Juhnke et al. 2007, p. 1). Given that adolescence is a time of heightened recklessness (e.g., unsafe sex, unsafe driving; substance use experimentation; Smith et al. 2013; Steinberg 2008) it represents a developmental period in which suicide may be more likely, given the presence of other risk factors (e.g., peer victimization).
Given that impulsivity is linked to suicidal behavior, the question that now arises is how is impulsivity related to suicide? Several researchers have attempted to answer this question. Bridge et al. (2006) developed a developmental–transactional model of youth suicide meant to explain the pathways in which a number of risk factors lead to suicidal ideation and suicide attempts. Their model begins with the parents, citing the fact that many of the risk factors that youth exhibit are present as well in their parents and are inherited, either genetically or environmentally (Bridge et al. 2006). Their model stresses the role of depression in leading to suicidal ideation and from suicidal ideation to suicide attempt. However, impulsivity and aggression play the role of a moderator, affecting the likelihood of suicidal ideation leading to a suicide attempt, with higher impulsive aggression leading to an increased likelihood of attempt. Another model of suicidal behavior proposed by Bender et al. (2011) cites the role of impulsivity in increasing the acquired capability for suicide. The acquired capability for suicide is one element of the Interpersonal-Psychological Theory of Suicide (IPTS), proposed first by Joiner (2005) and then elaborated on by Van Orden et al. (2010). While someone may be motivated to die by suicide, it is only those who have acquired the capability to enact lethal self-harm who are actually capable of doing so, according to this model. Exposure to painful experience, repeated attempts at suicide, interpersonal violence, and numerous other factors lead to acquiring the capability for suicide. According to this model, it is this element of suicidal behavior that impulsivity is tied to. Impulsivity is related to the acquired capability for suicide and through it to suicidal behavior itself (Bender et al. 2011).
Aggressive Behavior, Bullying, and Victimization
Before examining links between victimization and suicide, some of the different types of victimization that adolescents may encounter will be discussed. In an attempt to better understand the very complex behaviors of aggression and bullying, researchers have established a number of ways in which to categorize these behaviors. First, it is important to distinguish aggression and bullying. The constructs are overlapping (but not identical) behaviors (e.g., Boxer et al. 2008; Olweus 1978; Olweus and Limber 2010); both involve an intent to harm another but they differ with regard to the pattern of harm and the relationship between the perpetrator and the victim. Bullying involves a repeated, reoccurring habit of perpetrating aggression against an individual where there is a power imbalance between the victim and the perpetrator. Thus, all aggressive behavior does not constitute bullying, although all bullying does involve aggression. This distinction tends to get more flexible in research on cyber aggression and cyberbullying, however, where the terms are often used interchangeably (Goldstein 2015). Nonetheless, it is critical that those interested in understanding the research on suicide and aggression/bullying carefully review researchers’ operational definitions to see exactly how the experience of victimization was measured.
The second important way in which aggression and bullying has been parsed in an effort to better predict and understand behavior has to do with the method of harm delivered. Sometimes referred to as the “forms” of aggression (Fite et al. 2008; Little et al. 2003), researchers have separated harmful behavior into the general categories of physical aggression (behavior where the act of harm is physical in nature as in the case of hitting, pushing, or weapon use) and relational aggression (behavior where the victim’s social relationships are targeted, as in the case of spreading rumors or peer exclusion; Crick 1995; Crick and Grotpeter 1995). Others also include verbal aggression (direct verbal insults and threats) and cyber aggression or cyberbullying (harm inflicted through electronic means such as text messaging, emails, or online social network attacks) as distinct forms of aggression, although there clearly could be overlap between the forms in a single incident (e.g., a relationally aggressive incident that occurs online or a physical threat occurring online; further elaborated on in Barlett and Coyne 2014). The consensus regarding the terminology for these different “forms” is not unanimous, however. For example, the term indirect aggression is used instead of relational aggression to refer to behaviors where the identity of the perpetrator is unknown (these behaviors are often relationally focused; Björkqvist 1994; Österman et al. 1999) and others still use the term social aggression to also include subtle non-verbal acts of intentional harm like eye-rolling or making a mean face; these are often relationally focused behaviors as well (Cairns et al. 1988; Underwood 2003). Others have also noted that sexual harassment—unwanted and repeated sexual attention or advances—should be considered in research on adolescents’ aggressive behavior and especially in prevention and intervention efforts targeting youth aggression (Goldstein et al. 2007).
Despite the extensive variety of behaviors, and the varied opinions in terms of how the behaviors should be labeled, what emerges from the literature on aggression, bullying, and victimization as a whole is that aggression is not a one-size fits all phenomenon. Different children use different methods to inflict harm, and sometimes the same child uses different modes of inflicting harm. The research suggests that youth who engage in, or are victimized by, one form of aggression often have experiences with other forms as well; initial evidence suggests that this may be particularly true for cyber aggression (Dempsey et al. 2011; Waasdorp and Bradshaw 2015). To add further complexity to an already multifaceted topic, victimization can occur based on a targeted focus of one aspect of the victim’s identity such as sexual orientation, weight, race, or religion (e.g., Birkett et al. 2009; Puhl et al. 2013), and this victimization can take on a variety of forms (physical, relational, verbal, cyber, or sexually harassing). Victimization by each of these forms of aggression has been linked independently to an increased risk for negative socioemotional outcomes (including suicidal thoughts and behaviors), and perceptions of personal wellbeing and safety (e.g., Bradshaw et al. 2015; Goldstein et al. 2008; Hinduja and Patchin 2010). It is notable that cyber victimization is typically something that can be viewed repeatedly by the victim as often the incident remains visible for some time following its initial presentation (e.g., a social media post that is not deleted, or a text message that can be repeatedly viewed), thus creating the possibility for continued and repeated revisiting on the part of the victim.
Bullying and Psychopathology During Adolescence
The link between bullying and adjustment during adolescence is well established. Although it is outside of the scope of this article to review this association fully, in the next section some illustrations of this association will be provided as well as a discussion of the links to suicidality. Arseneault et al. (2010), in a review of the literature on bullying victimization, found that there was strong evidence in the literature for an association between bullying and aversive mental health outcomes. Specifically, the authors pointed to research indicating that mental health problems, self-harm, violent behavior, and psychotic symptoms were supported as potential outcomes of bullying and that bullying independently contributed to a child’s mental health outcomes. Furthermore, there is evidence supporting the long-term impact of bullying experiences in childhood and adolescence and later mental health outcomes; many of the problems that arise due to bullying in childhood last until late adolescence (Arseneault et al. 2010). Takizawa et al. (2014) found that children who reported being the victims of bullying were more likely to report poor social, health, and economic outcomes four decades after exposure to the victimization. Using an adolescent sample, Moore et al. (2014) found that those who reported being the victim of peer aggression at 14 years of age were more likely to report depression and internalizing symptoms at follow-up at 17 years of age. Additionally, those who reported being the aggressor had an increased risk of reporting depression and harmful alcohol use at age seventeen. Finally, those who reported being victim-perpetrators were more likely to report externalizing behavior at age seventeen.
Lereya et al. (2015) examined two groups of children from existing longitudinal datasets in the United States and in the United Kingdom. In both cohorts, those who experienced maltreatment (i.e., physical, emotional, or sexual abuse, and/or severe maladaptive parenting) and bullying were at an increased risk of experiencing overall mental health problems, anxiety, and depression, whereas those who experienced only maltreatment were not. Additionally, in the UK sample, those who experienced maltreatment and bullying were at an increased risk of reporting self-harm (Lereya et al. 2015). When comparing the effects of bullying and maltreatment across both samples, results indicated that bullying was more harmful than maltreatment, with bullying victims reporting more anxiety, depression, and self-harm than those who were maltreated only. Hase et al. (2015) compared the psychological symptoms of traditional bullying and cyberbullying among middle school and high school students. They found that both forms of bullying were associated with negative psychological symptoms. Furthermore, cyberbullying and traditional bullying were often co-occurring, with participants reporting experiencing both. When traditional bullying was controlled for, however, the negative effects of cyberbullying did not remain significant, though the reverse was not true (Hase et al. 2015).
Craig (1998) examined the relationship between bullying, depression, anxiety and aggression by following a cohort of students from grades five through eight. Craig found that as these children aged there was a decrease in physical aggression and an increase in verbal aggression. Interestingly, Craig found that both being a bully and being the victim of a bully was predictive of reports of anxiety, although victims reported more anxiety than bullies. Victims also reported more depressive symptoms than non-victim comparisons. The decrease in physical aggression and increase in verbal aggression is not surprising given the increase in social comparison and the focus on peer group that characterizes adolescence. Salmon et al. (1998) examined a wide array of variables (e.g., anxiety, esteem, lying, depression) among a sample of students in eighth through eleventh grade. Bullied children tended to be younger (i.e., it was more common in lower grades), tended to be more anxious, more depressed, and more likely to have high lying scores.
Bond et al. (2001), in a 2-year cohort study, assessed anxiety and depression in victims of bullying in secondary school. The authors confirmed a strong relationship between victimization and self-reported symptoms of anxiety and depression. Furthermore, the study found that a history of victimization was predictive of the onset of self-reported anxiety and depression in young girls, but was not found for young boys, indicating that victimization may be more aversive for girls than for boys. Due et al. (2009), utilizing a longitudinal design, examined the effects of bullying on depression and the role that socioeconomic status played in this relationship. In keeping with previous research, the authors once more found a relationship between bullying and depressive symptomology. Additionally, the authors found a relationship between childhood socioeconomic position (CSP) and the effects of bullying. Children from lower CSP reported a greater relationship between bullying and depressive symptomology, while children from higher CSP reported a weaker relationship than children from lower CSP. Kaltiala-Heino et al. (2010) performed a 2-year follow-up study in an attempt to ascertain whether or not involvement in bullying was predictive of depression. The authors found that both being a victim of bullying and being a perpetrator of bullying were both associated with reports of depression.
Although much of the research examining the effects of bullying on psychopathology has examined anxiety and depression, some work has also examined the impact of bullying on other mental health outcomes. Matthiesen and Einarsen (2004), utilizing an adult population, found that bullying (both direct and indirect) at work was associated with reported symptoms of Post-Traumatic Stress Disorder (PTSD). Higher levels of psychiatric distress were reported by those who experienced bullying at work and that the severity of the bullying affected this relationship. In addition to PTSD, the link between psychotic symptoms and bullying has also been examined. Campbell and Morrison (2007) examined psychotic symptoms in victims of bullying among 14–16 year old students. The authors found that students who reported being bullied at secondary school were more likely to report psychotic symptoms. Additionally, negative cognitions about the self and the world following the experience of bullying were further related to psychotic symptoms.
Victimization has been linked to physical concerns as well. For example, in a meta-analysis of studies using older children and adolescent populations linking bullying and a number of psychosomatic problems (e.g., headache, backache, stomach problems), Gini and Pozzoli (2009) found that victimized children and adolescents had higher risk for psychosomatic problems than non-victimized peers. Children and adolescents who were bullies themselves were also found to be at greater risk for psychosomatic problems as were children who reported being both victims of bullying and perpetrators. However, when compared between the three groups, bullies were found to have fewer adjustment problems than those who reported being victimized. Victims of bullying were more likely to report low self-esteem, loneliness, depression and anxiety, whereas bullies were more likely to report externalizing problems, poor school adjustment, and drug and alcohol use. The link between psychosomatic problems, depressive symptomatology, and suicidality has been illustrated in previous work. Roland (2002) showed a positive relationship between psychosomatic problems and depressive symptoms as well as between psychosomatic problems and suicidality. Hashiro and Okumura (1997) found that depressive symptoms and psychosomatic symptoms co-occurred in patients with atopic dermatitis. Fekkes et al. (2006) discussed the relationship between bullying, psychosomatic symptoms and psychological health symptoms. Again they confirmed the relationship between psychosomatic symptoms, negative psychological health symptoms and bullying. Given the relationship between psychosomatic symptoms, aversive mental health, and bullying, it is beneficial for educators and healthcare practitioners to be mindful of these potential connections in evaluation and diagnostic processes.
Limitations
There are a number of limitations that characterize many of the studies examining the linkage between bullying and psychopathology. As is often common in the social sciences, many of the studies were cross-sectional and, therefore, any discussion of causality is not permissible (Hashiro and Okumura 1997; Craig 1998; Salmon et al. 1998; Roland 2002; Matthiesen and Einarsen 2004; Campbell and Morrison 2007; Hase et al. 2015). Several of the studies that did utilize a longitudinal design experienced higher attrition rates than is desirable (Kaltiala-Heino et al. 2010; Moore et al. 2014). Self-report measures were heavily relied upon (Craig 1998; Fekkes et al. 2006; Kaltiala-Heino et al. 2010; Moore et al. 2014; Lereya et al. 2015, Hase et al. 2015). Finally, several studies did not differentiate between cyber-aggression and traditional forms of aggression (Moore et al. 2014; Lereya et al. 2015). Despite these limitations, the existing literature, of which these studies represent just a small sampling, supports a relationship between bullying and psychopathology.
Bullying and Suicide During Adolescence
As noted above, there is an abundance of evidence that bullying is connected to adverse mental health outcomes, both for the perpetrator and the victims of bullying. These mental health concerns, in turn, are linked independently with suicidal ideation and behavior. The purpose of the next section of this article is to focus on studies that have directly linked bullying with suicidal risk, focusing on studies conducted with adolescent participants.
Rigby and Slee (1999), in a sample of secondary schoolchildren in Australia, examined relations among bullying, perceived social support, and suicidal ideation. Those who reported being the victims of bullying and perceiving their social supports to be limited were more likely to experience suicidal ideation than those who were not the victims of bullying and who a lack of perceived social support. Cleary (2000), utilizing the Youth Risk Behavior Survey, showed that victimization leads to an increase in suicidal behavior as well as violent behavior. This increase in violence was particularly salient for males, who were more than two times as likely as females to report an increase in violent behavior following victimization. In a large sample of students, van der Wal et al. (2003) found that bullying was associated with depression and suicidal ideation in both girls and boys. Moreover, they found that the associations were stronger for indirect bullying than for direct bullying. The relationship between suicide risk and bullying was further supported by Kim et al. (2005) in a sample of seventh and eighth grade students. These findings also supported a greater risk among females of the sample.
Heikkila et al. (2013), in a follow-up study of Finnish girls and boys, found that those who were both victims and perpetrators of bullying were 3–4 times more likely to report suicidal ideation in comparing scores taken at age fifteen and those again measured at age seventeen. Additionally, those who were the victims of bullying were at an even greater risk of reporting suicidal ideation than those who were the perpetrators of bullying. Klomek et al. (2007), in a large sample of high school students, found that both being a victim of bullying as well as a perpetrator of bullying were both risk factors for adolescent depression and suicidality. In a Norwegian sample of adolescents measured twice, 1 year apart, Undheim (2013) confirmed the relationship between involvement in bullying, both as a victim and a perpetrator, and suicidal ideation. Girls in the sample experienced greater suicidal ideation than boys when the victims of bullying, though there was no relationship for those who were aggressive toward others. Reports of being the victim of a bully at time one were predictive of suicidal ideation at time two but aggressiveness towards others was not.
Kim et al. (2009), utilizing a cohort study of Korean adolescents, examined the relationship between bullying and suicide risk, while controlling for a number of suicide risk factors (i.e., anxiety/depression, aggressive behavior, and conduct problems). Bullying increased the risk for suicidal ideation independent of anxiety/depression, aggression, and conduct problems as measured by the Korean Youth Self-Report (K-YSR) with the greatest risk felt by victim-perpetrators, followed by victims. The greatest strength of Kim et al.’s (2009) study is the cohort design which allows for more causal interpretations than previous research. Furthermore, this research suggests that the greatest at risk group for adolescents engaged in bullying are those who are victims as well as perpetrators of bullying. Klomek et al. (2010) reviewed cross-sectional and longitudinal findings related to bullying and suicidality. Their review confirmed the elevated level of risk associated with being a victim-perpetrator, as well as confirming the relationship between suicide risk and victimization.
Focusing specifically on cyberbullying, Hinduja and Patchin (2010) found that participants who reported being the victims of or perpetrators of bullying in a classroom or cyber setting were at increased risk of experiencing suicidal ideation as well as making a suicide attempt. Although both experienced an increase in risk compared to those who had not experienced or participated in bullying, those who were victimized were at greater risk than those who had perpetrated bullying. Schneider et al. (2012) surveyed over 20,000 students from ninth- through twelfth-grade on the prevalence and psychological health outcomes of cyberbullying. The majority of students who reported experiencing cyberbullying also reported experiencing in-school bullying and there was an increased risk of victimization for non-heterosexual youth. Students who reported both cyber and in-school bullying were at the greatest risk of reporting depressive symptomology as well as medically serious suicide attempts (requiring medical treatment). In a study examining various forms of victimization, of which cyberbullying was one, Klomek et al. (2008) found that depression and suicidality were positively associated with being victimized because of one’s religion, race, looks or the way they talk; being slapped or hit; having rumors spread about them; having sexual jokes made about them; and being victimized through email or the internet.
Also interested in better understanding the role of cyberbullying in suicidality, Litwiller and Brausch (2013) found that both in-school bullying and cyberbullying were related to suicidality. Furthermore, they found relationships between both forms of bullying, substance use, violent behavior, and unsafe sexual behavior, all of which were found to be associated with suicidal behavior. A recent meta-analysis suggests that cyber bullying is associated with suicidal ideation at even greater rates than more traditional offline bullying (van Geel et al. 2014).
While the studies discussed above found support for the role of bullying in suicidality, there are some examples in the literature that do not support the role or that minimize the role of bullying in suicidal behavior, suggesting that bullying alone, without other risk factors, may not lead to suicidal behavior. Sinyor et al. (2014), utilizing observational data from psychological autopsies of youth who died by suicide in Toronto from 1998 to 2011, found that, while bullying was present in some of the suicides (6.4 %), there were other contributing factors that were more often present: conflict with parents (21.3 %), romantic partner problems (17.0 %), academic problems (10.6 %), and criminal and/or legal problems (10.6 %). The authors concluded that, while bullying plays a role in suicidal behavior, it is often just one of a number of risk factors. The finding that bullying, while related to suicidal behavior, is just one of a complex interplay of risk factors was further supported by Mayes et al. (2014). Mayes and colleagues found that being a bully/victim was significantly related to suicidality, but that all who reported a suicide attempt and the vast majority (all but two) who reported suicidal ideation had comorbid psychiatric disorders.
Limitations
There are a number of limitations that must be considered when evaluating the literature on the relationship between suicide and bullying. Perhaps the greatest limitation is the cross-sectional nature of much of the work that was examined (Rigby and Slee 1999; Cleary 2000; Van der Wal et al. 2003; Kim et al. 2005; Klomek et al. 2007, 2008; Hinduja and Patchin 2010; Schneider et al. 2012; Litwiller and Brausch 2013). Cross-sectional designs, while certainly providing a great deal of important information on the correlates of a behavior, do not allow for inference of causality. Of the studies examined, only three made use of a longitudinal design (Kim et al. 2009; Heikkila et al. 2013; Undheim 2013). These longitudinal designs were not without limitations, however. Heikkila et al. (2013) reported high attrition rates, which may have influenced the results of the study, given that it is likely that attrition could be linked to more severe symptomatology. Additionally, Kim et al. (2009) and Undheim (2013) both had relatively short follow-up periods, 10 months and 1 year, respectively. Thus, although the information derived from these longitudinal studies is extremely valuable, additional longitudinal research is needed to better understand links between bullying and suicide over time, focusing on various types of bullying behaviors and experiences over the course of adolescence.
In addition to these limitations, there were more general limitations that were present in a number of the studies. Self-report was the most common method for collecting data on bullying as well as suicidal symptomatology, with all studies using some form of self-report. Although self-report methodology is arguably the most valid way of assessing one’s internal state, it would be interesting to include multiple perspectives when assessing behavioral symptomology. Several of the studies were also limited in the information they collected on bullying (Cleary 2000; Klomek et al. 2008; Schneider et al. 2012). For example, relational aggression as well as cyber bullying were not differentiated from more traditional forms of aggression in a number of the studies (e.g., Cleary 2000; Klomek et al. 2008; Schneider et al. 2012). Due to this, it is hard to draw any conclusions about what types of bullying influence suicidal behavior (e.g., physical forms vs. relational forms). Finally, while certainly not the case for all the studies examined, the majority had limitations in the generalizability of the findings, typically due to the use of convenience samples or samples drawn from a single geographical region (Rigby and Slee 1999; Cleary 2000; Kim et al. 2005, 2009; Klomek et al. 2007, 2008; Schneider et al. 2012; Litwiller and Brausch 2013; Sinyor et al. 2014). However, despite the limitations of the studies presented, the evidence connecting bullying to suicide among adolescents is quite robust. Cross-sectional designed studies support the existence of a relationship between bullying and suicide. Additionally, longitudinal studies further illustrate this relationship, showing support for the long-term effects of exposure to bullying.
Groups with Heightened Vulnerability
Now that the relationship between bullying, psychopathology, and suicidality during adolescence has been reviewed, the focus of the next section will be to address the question as to whether certain groups of adolescents are at an increased risk for suicidality related to bullying behavior. Although a number of groups considered vulnerable or lacking majority status would have been appropriate to examine, the focus of this section will be on issues surrounding gender and sexual orientation, as these categories are especially relevant for adolescent identity development and for understanding adolescent adjustment in the context of identity-targeted bullying and bullying based on gender-specific socialization. It should be noted that there are many aspects of adolescents’ social experiences that might make them especially vulnerable to being bullied or to being especially impacted by bullying that occurs (e.g., family duress, off-time pubertal development, socioeconomic strain) and these may also interact with mental health challenges to increase the risk of suicidal ideation or behavior.
Gender, Victimization, and Suicide
Gender is critical to consider when examining adolescents’ social experiences and the implications that these social experiences have for developmental outcomes. From a young age, males and females are differentially socialized by parents, teachers, the media, and peers. From essentially every socialization agent, females and males receive gender-specific messages about goals, ideals, appropriate behavior, strengths, and weaknesses (Brown et al. 2015; Lawson et al. 2015). Females are taught (directly and indirectly) to value relationships, collaboration, and emotional expression, whereas males are socialized to focus on physicality, competition, and dominance. From this perspective, gender differences in psychological distress are not surprising. Adolescent females have greater emotional intensity and more strong emotional reactions to social stimuli, as compared to males, and they also have higher levels of depression (Charbonneau et al. 2009; Hyde et al. 2008). Additionally, adolescent females are more likely to report suicidal thoughts and attempts than are adolescent males (Kaess et al. 2011; Wunderlich et al. 2001). According to Kaess et al. (2011), one explanation for this gender difference is that adolescent females reported higher levels of internalizing problems and adolescent males reported higher levels of externalizing problems. In other words, adolescent males are more likely to act with outward displays of aggression while adolescent females are more likely to turn their aggression inward.
With regard to gender, it is important to note that, although females do attempt suicide more than males, males die by suicide at a disproportionately higher rate compared to females. Several explanations have been used to explain this gender gap. Females tend to utilize less lethal methods of suicide when they make an attempt (e.g., drug overdose) while males tend to choose more lethal means such as firearms (Schrijvers et al. 2012; Callanan and Davis 2011; Denning et al. 2000). Joiner (2005) points to the role of the acquired capability for suicide discussed previously. Men display more physical violence than women and live more physically violent lives; due to this, they have acquired the capability to enact lethal self-harm at a greater degree than women and therefore make up a large number of fatal suicides.
Gendered socialization also contributes to youth’s experiences with victimization. Although both males and females engage in, and are victimized by, aggressive behaviors, the specific behaviors used to inflict harm to some extent vary based on gender. Males, as compared to females, are consistently more likely to engage in physical aggression and to be victimized by physical means (Archer 2004). With regard to relational aggression, although the research is mixed in terms of whether males or females are more relationally aggressive (Archer and Coyne 2005; Card et al. 2008), findings consistently show that relational aggression is a special concern for girls, in that girls and boys experience and interpret relationally aggressive behavior differently. For example, girls, as compared to boys, perceive relational aggression to be more hurtful, hostile, and detrimental to their social relationships (e.g., Crick 1995; Goldstein and Tisak 2004, 2010; Paquette and Underwood 1999). In addition, girls are more likely to be victimized by sexual aggression and harassment (Goldstein et al. 2007; Turner et al. 2011), as compared to boys.
As was indicated by a number of the studies discussed, the relationship between adverse outcomes (e.g., depressive symptomatology and suicidality) and bullying was strongest for females (e.g., Bond et al. 2001; Kim et al. 2005; Undheim 2013; Klomek et al. 2010). One explanation for this difference is the fact that adolescent females are more likely to report internalizing problems while adolescent males are more likely to report externalizing problems, turning their aggression outward while females turn theirs inward (Kaess et al. 2011). Undheim (2013) discussed this finding in regard to the maturity of girls at this age, pointing to evidence that adolescent females worry more about life and feel more pressure from society at this age than do adolescent males. Rumination is another mechanism by which adolescent females may be more prone to suicidality than adolescent males. Previous work has supported a relationship between rumination and suicidality (Morrison and O’Connor 2008), and rumination is more common among females (Johnson and Whisman 2013; Nolen and Jackson 2001; Nolen et al. 1999). Type of bullying experienced may also play a role in the gender difference in aversive outcomes. As discussed previously, when girls are victimized by other girls it is most likely to be by relational aggression, and when they are victimized by relational aggression girls experience it more negatively, as compared to their male peers (Crick 1995; Goldstein and Tisak 2004, 2006; Paquette and Underwood 1999). This is especially relevant to discussions of suicide, as social relationships have been proposed as an important element in suicidal behavior. Specifically, damage or perceived damage to social relationships has been theorized to be one of the most important factors in suicide (e.g., Joiner 2005; Van Orden et al. 2010). Additionally, loneliness (which may result as an aftermath of being ostracized by one’s group of friends due to relational aggression) has been established as a risk factor in adolescent suicide (e.g., Page et al. 2006; Roberts and Chen 1995) though the relationship to suicide may be a byproduct of other factors such as depressive symptomatology or its relationship to hopelessness (e.g., Lasgaard et al. 2011; Joiner and Rudd 1996).
In sum, gender differences in experiences with aggression and bullying are due, at least in part, to gender differences in socialization (Crick 1995; Lagerspetz et al. 1988; Underwood 2003). These gender differences in socialization also partially explain the gender differences in aversive psychological outcomes following relational aggression, sexual harassment, and possibly cyberbullying (e.g., Galen and Underwood 1997; Goldstein et al. 2007; Goldstein and Tisak 2004), which may also help to partially explain the increased risk for suicidal thoughts and behavior among adolescent females. Differential socialization also relates to gender differences in physical aggression, and to lethal suicidal behaviors in males.
Sexual Orientation, Victimization, and Suicidality
Another group of adolescents who are at-risk for suicidal cognition and behavior, and one that has gathered a large amount of media attention, are adolescents who identify as members of the Lesbian, Gay, Bisexual, and Transgender (LGBT) community. This has been established in a number of studies focusing on different components of suicidal risk. Russell and Joyner (2001), using the National Longitudinal Study of Adolescent Health (Add Health), found that adolescents who identified themselves as being attracted to members of the same sex were more likely to report suicidal thoughts and suicidal behavior. This relationship was mediated by youth suicide risk factors, depression, hopelessness, alcohol use, suicidal behavior among friends, and experiences of victimization. Friedman et al. (2006) examined the relationship between bullying, social support, and suicidality in gay male adolescents. The authors found that suicidality was greatest in males who reported higher levels of femininity and bullying was found as a mediator of this relationship. As with other studies, bullying was once more found to be related to suicidality.
Almeida et al. (2009) found, in a large sample of 9th–12th grade students from Boston, that LGBT students were more likely to report depressive symptomatology, suicidal ideation, and self-harm than were heterosexual, non-transgendered youth. Furthermore, Almeida and colleagues found that perceived discrimination accounted for the increased symptomatology. Berlan et al. (2010) found that, among females, sexual minorities were more likely to report bullying victimization and perpetration than were heterosexual females. Among males, those classified as “mostly heterosexual” and gay were more likely to experience bullying as perpetrators and victim than were heterosexual males.
LeVasseur et al. (2013), using New York City’s Youth Risk Behavior Survey, found further support for a relationship between sexual minority status and suicidality. Furthermore, they found that sexual minority, gender, and ethnic identities interacted with bullying to predict participants who reported a suicide attempt. In a similar study, Mueller et al. (2015) examined the intersection of race, gender, sexual orientation and suicidality. They found that White and Hispanic gay and bisexual males, White lesbian and bisexual females, and Hispanic bisexual females were more likely to report being bullied than were White heterosexual adolescents. However, the difference between White heterosexual youth and Black lesbian, gay, and bisexual youth was non-significant. Sexual minority youth were more likely to report suicidal ideation, regardless of race, gender, and whether they had experienced bullying.
Why are adolescent members of the LGBT community at an elevated risk for suicide? First, as noted above, sexual minority youth are victimized disproportionately more as compared to their peers (Berlan et al. 2010; Levasseur et al. 2013; Russell and Joyner 2001). Because bullying predicts suicidality across groups, this alone elevates their risk. Relatedly, another explanation that may account for this increase in suicidality among this group is the additional stress of minority status (Meyer 2003). Minority stress is the added stress felt by groups for having minority status and facing the prejudice and discrimination typically associated with being a member of a stigmatized social group. Additionally, LGBT adolescents face a number of complications that hamper the formation of social support (Safren and Pantalone 2006). Many are unable to be open about their sexuality, limiting greatly any likelihood of the development of romantic bonds. In order to fit in, it may be necessary for sexual minorities to hide this vital aspect of their lives. Adolescence is a time for identity exploration and formation; identity development is greatly influenced by family, peers, and perceptions of social norms (Meeus and Dekovic 1995). Thus, conflicts between sexuality and perceptions of social norms may lead LGBT adolescents to feel alienated, and may increase their susceptibility to experiences of victimization.
Protective Factors
One question that must be answered is what differentiates adolescents who attempt suicide following experiences of bullying from those who do not? As noted in the beginning of this article, positive developmental outcomes are most likely among adolescents who are in environments that are a good match for their evolving developmental needs, including social connection, identity exploration, and autonomy support (Eccles et al. 1991, 1993; Goldstein et al. 2005). Although Rigby and Slee (1999) found support for the role of bullying in suicidal behavior, their results also indicated that those who reported higher social support were less likely to report suicidality than were those who reported lower social support. Fleming et al. (2007), in a large sample of adolescents (9570), found that reports of parents caring, other family members caring, teachers being fair and feeling safe at school were all associated with decreased rates of suicide attempts. Bonanno and Hymel (2010) compared adolescents on ratings of victimization, social hopelessness, social support, and suicidality. While hopelessness is a well-established risk factor for suicide, the authors focused on social hopelessness. They found that the relationship between victimization and suicidal ideation was mediated, partially, by social hopelessness, which indicated that social hopelessness was one factor through which victimized adolescents become suicidal. Additionally, the authors found that students who reported higher levels of social support reported lower levels of suicidality.
Familial protective factors have also been shown to decrease suicide risk. Borowsky et al. (2013) found support for the role of parent connectedness, perceived caring by friends and non-parental adults as protective factors against suicide in those who experienced bullying. Elgar et al. (2014) found that participation in family dinners had a positive impact on the mental health of those experiencing cyberbullying. These findings highlight the importance of familial factors in counteracting the harmful effects of exposure to bullying.
Finally, focusing on sexual minorities exposed to bullying, Hatzenbuehler et al. (2014) found that school climates that protected minority students (e.g., had safe spaces or Gay-Straight Alliances) had lower incidences of suicidal thoughts among sexual minority students, while schools that did not have protective environments for sexual minority students had increased reports of suicidal thoughts among sexual minorities. Although these studies have examined different factors associated with lowering adolescents’ suicide risk, taken as a whole, this body of research illustrates the protective role of a supportive, nurturing, developmentally appropriate environment for adolescents.
Discussion
In this review article, research showing clear adverse outcomes faced by adolescents who are the victims and perpetrators of bullying has been reviewed. It has been argued that these bullying experiences, and the associated mental health challenges including suicidality, are best viewed through a lens that considers adolescents’ unique developmental needs. Although the articles reviewed cannot encompass the whole of the scholarly literature on the topic, they are representative of the findings across the field. Regardless of the form that it takes, aggressive behavior and bullying have negative health outcomes. As discussed, bullying behavior is associated with depressive symptomatology as well as PTSD and psychotic symptoms. Furthermore, bullying is related to suicidal ideation as well as suicide attempt behavior. Psychologically vulnerable adolescents, because of their multiple social, physical, and psychological transitions coupled with their neurological immaturity but increased social access, are especially at risk for engaging in behavior that may cause them ultimate harm.
To summarize, there are a number of factors at play that likely increase the risk of psychopathology and suicidality in adolescence. While adolescents are capable of abstract logic and more adult thinking than older children, the prefrontal cortex develops at a slower rate than does the limbic system. Due to this, as well as an increase in hormones associated with puberty, adolescence is characterized by emotional swings and limited emotional regulation. This creates a tendency toward more reckless, impulsive behavior. In turn, this tendency is associated with increased suicidality. Additionally, at a time when the importance of social comparison and peer groups is at an all-time high, the experience of victimization at the hands of a peer could have the devastating effect of increasing suicidality and psychopathology.
It is also important to mention that certain groups of adolescents have experiences that place them at a heightened risk for suicidality linked to bullying. Research was reviewed showing that females were especially sensitive to relationally aggressive infractions and sexual harassment, and that females were also more likely than males to attempt suicide. Adolescent males, however, are more likely than their female counterparts to complete a suicidal attempt. Sexual minority youth are also more likely to report negative outcomes in relation to bullying behavior, and are also more likely to engage in suicidal cognition and behavior.
At the beginning of this article some of the statistics concerning suicide as well as three cases of suicide tied to bullying were discussed. It is important to keep these numbers in mind but also to keep in mind Tyler, Olivia Perryman, and Olivia Penpraze. While the problem of suicide as a national and international problem can be acknowledged by examining the statistics so far discussed, it is often easy to become desensitized to the devastation of suicide when looking solely at the numbers. Tyler was 18, Olivia Perryman was 14, and Olivia Penpraze was 19 years old.
Thus, it is clearly critical to apply the existing evidence on this topic to ways in which suicidality during adolescence can be prevented. This review of the literature has revealed a number of commonalities across studies that point to some clear prevention implications. The first important point is that adolescence is a unique developmental period and any attempts to prevent or intervene upon suicidal ideology or behavior must take this developmental context into consideration. This is also the case for programs designed to target bullying prevention and intervention. The topic of characteristics of developmentally appropriate prevention programming for adolescents has been discussed elsewhere (e.g., Boxer et al. 2008); the consensus is that such programming should have respect for the changing cognitive capacity of teens while acknowledging the need for personal autonomy, peer approval and acceptance, identity development, and family and school involvement where appropriate.
Second, although bullying occurs throughout adolescence, there are specific vulnerabilities that different groups of adolescents face. Specifically discussed are female adolescents for internalizing behavior and suicide attempts, male adolescents for lethal suicidal efforts, and LGBT youth for increased victimization, psychological distress, and suicidality. Given the increased risk of psychopathology and suicidality associated with bullying and for members of these groups, initiatives should focus on targeting the specific needs of these populations.
With a focus on bullying reduction (which ultimately reduces one risk factor for suicide, as discussed throughout this article), the National Crime Prevention Center gives a number of strategies to decrease the incidence of criminal behavior related to bullying. Several of the strategies have clear implications for the prevention of bullying behavior and are included below (Strategies 2016):
-
1.
Introduce diversity tolerance and education in school: Introducing tolerance and diversity education at the elementary-high school level can have an impact on the incidence of bullying and discrimination among adolescent populations.
-
2.
Start peer mediation starting in high school: This strategy has students engaging in peer mediation. This allows for students to develop conflict resolution skills as well as increasing communication and anger management skills in an environment conducive to discussion.
-
3.
Involve parents: Parents can be involved in a number of ways. For example, parents can set a good model for kind, non-bullying behavior within the family context. As another example, parents can regularly discuss peers and social issues with their children.
-
4.
Implement student advisory boards: Implementation of student advisory boards can increase the input of students in procedures and programs that are being used to prevent bullying behavior.
-
5.
Establish hotlines: These can be essential for the prevention of bullying behavior as well as increasing the likelihood of outreach from victims themselves.
The recommendations above are but a few that are offered by the National Crime Prevention Center, but are the ones more salient to bullying behavior. Further recommendations are made by the Center for Disease Control and Prevention (CDC). In an informational pamphlet released by the CDC’s Division of Violence Prevention, they summarized a number of key findings and how these could be applied to preventing suicide in schools. The recommendations were (National Center for Injury Prevention and Control, n.d.):
-
1.
Create a strong sense of connectedness by, for example, encouraging school personnel’s use of first names to greet students and to ask about their days.
-
2.
Teach coping/life skills that encourage resilience and acceptance of differences.
-
3.
Teach school staff about vulnerable populations and the appropriate ways to intervene when bullying situations occur.
-
4.
While bullying behavior should not be encouraged, it is important that the focus not be on blame, shame, or criminalization. Getting youth who engage in bullying professional support for themselves and their families, may aid in making positive change and prevent future bullying behavior.
-
5.
Get peer groups involved. Empowering youth to change the tone of bullying behavior and making it seen as “uncool” will aid in the prevention of the behavior.
In addition to the recommendations provided by the CDC, the Olweus Bullying Prevention Program (OBPP) is an example of a vetted program with demonstrable effects. The OBPP is a school-wide program designed to reduce bullying and to improve peer relations from elementary school through junior high school grades. The OBPP has components that involve schools, classrooms, individuals, and the community in prevention. For example, at the school-wide level, one strategy is to implement a bullying prevention coordinating committee, at the classroom level it is expected that schoolwide rules against bullying will be posted and enforced, at the individual level children’s activities will be supervised, and at the community level members of the community would be used on the coordinating committee to involve the community (Hazelden Foundation 2007). These are just a few examples as to how the OBPP utilizes a wide range of strategies across several levels. The OBPP has garnered support in the literature as a method for preventing bullying behavior in schools. Olweus and Limber (2010) found compelling evidence for the program’s effectiveness in Norwegian schools. Furthermore, they reported that the body of evidence supported the OBPP as having a positive impact on students’ self-reported involvement in bullying and antisocial behavior in the United States. Additionally, programs that are based on the OBPP model have been shown to be the most effective (Farrington and Ttofi 2009). Additionally, Beckman and Svensson (2015) examined whether or not the OBPP was a cost-effective bullying prevention technique. Their analysis revealed that it was, in fact, a cost-effective intervention, which is important given that implementation of this program would require budget allocation.
Given the relationship between bullying and adolescent suicide, prevention of aggression and bullying in schools will aid in the reduction in suicide risk among this population but it is not enough. Interventions are necessary that target suicidality directly. One difficulty in preventing suicide among adolescence is that many of the risk factors for suicide are in common among adolescent populations. The American Association of Suicidology uses the mnemonic IS PATH WARM in order to represent a number of risk factors for suicide (Juhnke et al. 2007). The mnemonic represents: Suicide Ideation, Substance Abuse, Purposelessness, Anger, Trapped, Hopelessness, Withdrawing, Anxiety, Recklessness, and Mood Change.
As can be seen by examining the above list, many of the risk factors for suicide could be mistaken for a “typically” moody, seemingly bored and withdrawn adolescent, especially if parents have expectations for relatively high levels of malcontent among their adolescent children based on their own negative stereotypes of the developmental period. Further, as discussed above, recklessness and risk-taking peak during adolescence, with the developing brain’s emotional centers outpacing the development of the reflective, more adult cognitions. This increased emotionality, coupled with the exposure to increased social pressures that are characteristic of adolescence can lead to mood changes and swings that could be easily misinterpreted if one were to rely solely on this mnemonic to assess suicide risk among adolescents.
So, how can adolescent suicide be prevented? Communication is perhaps the key to preventing adolescent suicide, as well as suicide in general. It is a common misconception that those that are suicidal do not communicate their suicidal intent and that those who communicate suicidal intent are actually not suicidal (Joiner 2010). However, the reality is that the majority of those who die by suicide give signs of their intention to die and many communicate suicidal intent. Due to this, prevention programs focusing on adolescents should focus on communicating the warning signs of suicide as well as helping to de-stigmatize discussions about suicide. Additionally, education about normative adolescent development is crucial, so that teens, parents, and educators alike can more easily disentangle typical changes and challenges from more potentially dangerous ones. This is often done by programs that teach family, friends, and co-workers these signs and bring them into the fold of suicide prevention (e.g., Stop a Suicide Today!). Additionally, as the review of protective factors indicates (Rigby and Slee 1999; Bonanno and Hymel 2010; Borowsky et al. 2013), one of the ways to minimize the relationship between bullying and suicidality is to increase social supports. This can be done both within the family (e.g., family dinners or activities) or outside (e.g., with peer groups or non-parental adults). Increasing the sense of social connectedness or the sense of social support can make the difference between life and death for a bullied adolescent. Adolescents should be provided with a number of ways in which they can establish healthy, supportive peer relationships; out-of-school venues for this (such as community or religious organizations or clubs, community-based classes in an area of special interest) may be especially helpful for youth who feel disconnected or victimized at school.
As hopelessness is a risk factor for suicide, hopefulness is a protective factor against suicide. With the high profile suicides of a number of LGBT adolescents, a focus on intervention and prevention has increased. One program, the It Gets Better Project (http://www.itgetsbetter.org/), utilized videos of members of the LGBT community who communicated their experiences with bullying and victimization and discussing how things have gotten better for them. The website, in addition to offering a number of inspirational videos, also links those who visit the site directly to suicide prevention hotlines for the general public as well as hotlines specific to the LGBT community. Sites such as this promote the protective nature of hopefulness, connect those who visit to services, and de-stigmatize talking about suicide.
Conclusion
In this review, the importance of considering the unique developmental period of adolescence in all facets to better understand the link between bullying and suicide has been highlighted and applied to a discussion of interventions and preventative techniques that address bullying behavior. The scholarly literature as well as the anecdotal evidence described at the beginning of this review points to the importance of preventing bullying behavior and creating interventions to aid in the recognition of those at risk of attempting suicide. What has hopefully been made apparent throughout this review is the importance of taking into account the unique developmental stage of adolescence. Adolescence, with its rapid social and psychological changes coupled with its uneven brain development (hallmarked by increased impulsivity, risk-taking, and emotionality), is a period of substantial risk for suicide. This increased risk, when coupled with exposure to peer victimization, can have deadly consequences. Preventative measures for suicide, while perhaps working for some populations, may not work for all. Adolescence, with its emotional swings and tendency toward impulsivity and reckless behavior, is a time period that must be targeted for suicide prevention and these prevention methods must be geared specifically toward the unique developmental needs of this population. Bullying behavior has a devastating effect on adolescents and by preventing bullying or diminishing its impact, lives will be saved.
References
Almeida, J., Johnson, R. M., Corliss, H. L., Molnar, B. E., & Azrael, D. (2009). Emotional distress among LGBT youth: The influence of perceived discrimination based on sexual orientation. Journal of Youth and Adolescence, 38, 1001–1014. doi:10.1007/s10964-009-9397-9.
Apter, A., Gothelf, D., Orbach, I., Weizman, R., Ratzoni, G., Har-Even, D., et al. (1995). Correlation of suicidal and violent behavior in different diagnostic categories in hospitalized adolescent patients. Journal of the American Academy of Child and Adolescent Psychiatry, 34, 912–918.
Archer, J. (2004). Sex differences in aggression in real-world settings: A meta-analytic review. Review of General Psychology, 8, 291–322. doi:10.1037/1089-2680.8.4.291.
Archer, J., & Coyne, S. M. (2005). An integrated review of indirect, relational, and social aggression. Personality and Social Psychology Review, 9, 212–230.
Arseneault, L., Bowes, L., & Shakoor, S. (2010). Bullying victimization in youths and mental health problems: ‘Much ado about nothing’? Psychological Medicine, 40, 717–729. doi:10.1017/S0033291709991383.
Astor, R. A., Meyer, H. A., & Pitner, R. O. (2001). Elementary and middle school students’ perceptions of violence-prone school subcontexts. The Elementary School Journal, 101, 511–528.
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84, 191–215.
Bandura, A. (1986). Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ: Prentice Hall.
Barlett, C., & Coyne, S. M. (2014). A meta-analysis of sex differences in cyber-bullying behavior: The moderating role of age. Aggressive Behavior, 40, 474–488. doi:10.1002/ab.21555.
Baron, P., & Hanna, J. (1990). Egocentrism and depressive symptomatology in young adults. Social Behavior and Personality: An International Journal, 18(2), 279–285.
Baum, S. (2015). Cyber-bullying and suicide: Is there a link? What are the roles of traditional bullying and the media? In P. Goldblum, D. L. Espelage, J. Chu, & B. Bongar (Eds.), Youth suicide and bullying: Challenges and strategies for prevention and intervention (pp. 77–89). New York, NY: Oxford University Press.
Baum, K. T., Desai, A., Field, J., Miller, L. E., Rausch, J., & Beebe, D. W. (2014). Sleep restriction worsens mood and emotion regulation in adolescents. Journal of Child Psychology and Psychiatry, 55, 180–190. doi:10.1111/jcpp.12125.
Beautrais, A. L., Joyce, P. R., & Mulder, R. T. (1999). Personality traits and cognitive styles as risk factors for serious suicide attempts among young people. Suicide and Life-Threatening Behavior, 29, 37–47.
Beckman, L., & Svensson, M. (2015). The cost-effectiveness of the Olweus Bullying Prevention Program: Results from a modelling study. Journal of Adolescence, 45, 127–137. doi:10.1016/j.adolescence.2015.07.020.
Bender, T. W., Gordon, K. H., Bresin, K., & Joiner, T. E., Jr. (2011). Impulsivity and suicidality: The mediating role of painful and provocative experiences. Journal of Affective Disorders, 129, 301–307. doi:10.1016/j.jad.2010.07.023.
Benner, A. D. (2011). The transition to high school: Current knowledge, future directions. Educational Psychology Review, 23, 299–328. doi:10.1007/s10648-011-9152-0.
Berlan, E. D., Corliss, H. L., Field, A. E., Goodman, E., & Austin, S. B. (2010). Sexual orientation and bullying among adolescents in the growing up today study. Journal of Adolescent Health, 46, 366–371. doi:10.1016/j.jadohealth.2009.10.015.
Berndt, T. J., & Perry, T. B. (1990). Distinctive features and effects of early adolescent friendships. In R. Montemayor, G. R. Adams, & T. P. Gullotta (Eds.), From childhood to adolescence: A transitional period? Advances in adolescent development: An annual book series (Vol. 2, pp. 269–287). Thousand Oaks, CA: Sage.
Birkett, M., Espelage, D. L., & Koenig, B. (2009). LGB and Questioning students in schools: The moderating effects of homophobic bullying and school climate on negative outcomes. Journal of Youth and Adolescence, 38, 989–1000. doi:10.1007/s10964-008-9389-1.
Björkqvist, K. (1994). Sex differences in physical, verbal, and indirect aggression: A review of recent research. Sex Roles, 30, 177–188.
Blakemore, S., Burnett, S., & Dahl, R. (2010). The role of puberty in the developing adolescent brain. Human Brain Mapping, 31, 926–933. doi:10.1002/hbm.21052.
Bonanno, R. A., & Hymel, S. (2010). Beyond hurt feelings: Investigating why some victims of bullying are at greater risk for suicidal ideation. Merrill-Palmer Quarterly, 56(3), 420–440.
Bond, L., Carlin, J. B., Thomas, L., Rubin, K., & Patton, G. (2001). Does bullying cause emotional problems? A perspective study of young teenagers. British Medical Journal, 323, 480–484. doi:10.1136/bmj.323.7311.480.
Borowsky, I. W., Taliaferro, L. A., & McMorris, B. J. (2013). Suicidal thinking and behavior among youth involved in verbal bullying: Risk and protective factors. Journal of Adolescent Health, 53, 54–512. doi:10.1016/j.jadohealth.2012.10.280.
Boxer, P., Terranova, A. M., Savoy, S. C., & Goldstein, S. E. (2008). Developmental issues in the prevention of aggression and violence in school. In T. Miller (Ed.), School violence and primary prevention. New York, NY: Springer.
Bradshaw, C. P., Waasdorp, T. E., & Johnson, S. L. (2015). Overlapping verbal, relational, physical, and electronic forms of bullying in adolescence: Influence of school context. Journal of Clinical Child & Adolescent Psychology, 44, 494–508. doi:10.1080/15374416.2014.893516.
Bridge, J. A., Goldstein, T. R., & Brent, D. A. (2006). Adolescent suicide and suicidal behavior. Journal of Child Psychology and Psychiatry, 47(3), 372–394. doi:10.1111/j.1469-7610.2006.01615.x.
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Cambridge, MA: Harvard University Press.
Bronfenbrenner, U., & Morris, P. A. (1998). The ecology of developmental processes. In W. Damon & R. Lerner (Eds.), Handbook of child psychology, Vol. 1. Theoretical models of human development (6th ed., pp. 793–828). Hoboken, NJ: Wiley.
Brown, B. B., & Braun, M. T. (2013). Peer relations. In C. Proctor & P. A. Linley (Eds.), Research, applications, and interventions for children and adolescents: A positive psychology perspective (pp. 149–164). New York, NY: Springer.
Brown, G. L., Craig, A. B., & Halberstadt, A. G. (2015). Parent gender differences in emotion socialization behaviors vary by ethnicity and child gender. Parenting Science and Practice, 15, 135–157. doi:10.1080/15295192.2015.1053312.
Brown, B. B., & Larson, J. (2009). Peer relationships in adolescence. In R. M. Lerner & L. Steinberg (Eds.), Handbook of adolescent psychology, Vol 2: Contextual influences on adolescent development (3rd ed., pp. 74–103). Hoboken, NJ: Wiley.
Buhrmester, D. (1996). Need fulfillment, interpersonal competence, and the developmental contexts of early adolescent friendship. In W. M. Bukowski, A. F. Newcomb, & W. W. Hartup (Eds.), The company they keep: Friendship in childhood and adolescence (pp. 158–185). New York, NY: Cambridge University Press.
Cairns, R. B., Cairns, B. D., Neckerman, H. J., Gest, S. D., & Gariepy, J. (1988). Social networks and aggressive behavior: Peer support or peer rejection? Developmental Psychology, 24, 815–823.
Callanan, V. J., & Davis, M. S. (2011). Gender differences in suicide methods. Social Psychiatry and Psychiatric Epidemiology, 47(6), 857–869. doi:10.1007/s00127-011-0393-5.
Campbell, M. L. C., & Morrison, A. P. (2007). The relationship between bullying, psychotic-like experiences and appraisals in 14–16-year olds. Behaviour Research and Therapy, 45, 1579–1591. doi:10.1016/j.brat.2006.11.009.
Card, N. A., Stucky, B. D., Sawalani, G. M., & Little, T. D. (2008). Direct and indirect aggression during childhood and adolescence: A meta-analytic review of gender differences, intercorrelations, and relations to maladjustment. Child Development, 79, 1185–1229.
Casey, B. J., Jones, R. M., Levita, L., Libby, V., Pattwell, S., Ruberry, E., et al. (2010). The storm and stress of adolescence: Insights from human imaging and mouse genetics. Developmental Psychobiology, 52, 225–235. doi:10.1003/dev.20447.
Charbonneau, A. M., Mezulis, A. H., & Hyde, J. S. (2009). Stress and emotional reactivity as explanations for gender differences in adolescents’ depressive symptoms. Journal of Youth and Adolescence, 38, 1050–1058.
Cleary, S. D. (2000). Adolescent victimization and associated suicidal and violent behaviors. Adolescence, 35(140), 671–682.
Craig, W. M. (1998). The relationship among bullying, victimization, depression, anxiety, and aggression in elementary school children. Personality and Individual Differences, 24(1), 123–130. doi:10.1016/S0191-8869(97)00145-1.
Crick, N. R. (1995). Relational aggression: The role of intent attributions, feelings of distress, and provocation type. Development and Psychopathology, 7, 313–322. doi:10.1017/S0954579400006520.
Crick, N. R., & Bigbee, M. A. (1998). Relational and overt forms of peer victimization: A multiinformant approach. Journal of Consulting and Clinical Psychology, 66(2), 337–347.
Crick, N. R., & Grotpeter, J. K. (1995). Relational aggression, gender, and social–psychological adjustment. Child Development, 66(3), 710–722.
Crick, N. R., & Grotpeter, J. K. (1996). Children’s treatment by peers: Victims of relational and overt aggression. Development and Psychopathology, 8(2), 367–380. doi:10.1017/S0954579400007148.
Crouter, A. C., & Booth, A. (2006). The slippery nature of romantic relationships: Issues in definition and differentiation. Mahwah, NJ: Lawrence Erlbaum Associates.
Dahl, R. E. (2004). Adolescent brain development: A period of vulnerabilities and opportunities: Keynote address. In R. E. Dahl & L. P. Spear (Eds.), Adolescent brain development: Vulnerabilities and opportunities (Vol. 1021, pp. 1–22). New York, NY: New York Academy of Sciences.
Darling, N., Cumsille, P., & Martinez, M. L. (2008). Individual differences in adolescents’ beliefs about the legitimacy of parental authority and their own obligation to obey: A longitudinal investigation. Child Development, 79, 1103–1118. doi:10.1111/j.1467-8624.2008.01178.x.
Dempsey, A. G., Sulkowski, M. L., Dempsey, J., & Storch, E. A. (2011). Has cyber technology produced a new group of peer aggressors? Cyberpsychology, Behavior, and Social Networking, 14, 297–302. doi:10.1089/cyber.2010.0108.
Denning, D. G., Conwell, Y., King, D., & Cox, C. (2000). Method choice, intent, and gender in completed suicide. Suicide and Life-Threatening Behavior, 30(3), 282–288. doi:10.1111/j.1943-278X.2000.tb00992.x.
Dishion, T. J., Nelson, S. E., & Bullock, B. M. (2004). Premature adolescent autonomy: Parent disengagement and deviant peer process in the amplification of problem behaviour. Journal of Adolescence, 27, 515–530. doi:10.1016/j.adolescence.2004.06.005.
Dishion, T. J., Nelson, S. E., & Kavanagh, K. (2003). The family check-up with high-risk young adolescents: Preventing early-onset substance use by parent monitoring. Behavior Therapy, 34, 553–571. doi:10.1016/S0005-7894(03)80035-7.
Dorn, L. D., & Biro, F. M. (2011). Puberty and its measurement: A decade in review. Journal of Research on Adolescence, 21(1), 180–195. doi:10.1111/j.1532-7795.2010.00722.x.
Drapeau, C. W., & McIntosh, J. L. (for the American association of Suicidology). (2015). U.S.A. suicide 2014: Official final data. Washington, DC: American Association of Suicidology, dated December 22, 2015, downloaded from http://www.suicidology.org.
Due, P., Damsgaard, M. T., Lund, R., & Holstein, B. E. (2009). Is bullying equally harmful for rich and poor children?: A study of bullying and depression from age 15 to 27. European Journal of Public Health, 19(5), 464–469. doi:10.1093/eurpub/ckp099.
Ebbels, K. (2010). Tragic end for a true talent. NorthJersey.com. Retrieved from http://www.northjersey.com/news/tragic-end-for-a-true-talent-1.920406.
Eccles, J. A. (2004). Schools, academic motivation, and stage-environment fit. In R. M. Lerner & L. Steinberg (Eds.), Handbook of adolescent psychology (2nd ed., pp. 125–154). Hoboken, NJ: Wiley.
Eccles, J. S., Lord, S., & Midgley, C. (1991). What are we doing to early adolescents? The impact of educational contexts on early adolescents. American Journal of Education, 99, 521–542.
Eccles, J. S., Lord, S. E., & Roeser, R. W. (1996). Round holes, square pegs, rocky roads, and sore feet: The impact of stage-environment fit on young adolescents’ experiences in schools and families. In D. Cicchetti & S. L. Toth (Eds.), Adolescence: Opportunities and challenges (pp. 47–92). Rochester, NY: University of Rochester Press.
Eccles, J. S., & Midgley, C. (1989). Stage/environment fit: Developmentally appropriate classrooms for early adolescents. In R. E. Ames & C. Ames (Eds.), Research on motivation in education (Vol. 3, pp. 139–186). San Diego, CA: Academic Press.
Eccles, J. S., Templeton, J., Barber, B., & Stone, M. (2003a). Adolescence and emerging adulthood: The critical passage ways to adulthood. In M. H. Bornstein, L. Davidson, C. L. M. Keyes, & K. A. Moore (Eds.), Well-being: Positive development across the life course (pp. 383–406). Mahwah, NJ: Lawrence Erlbaum Associates.
Eccles, J. S., Wigfield, A., & Byrnes, J. (2003b). Cognitive development in adolescence. Handbook of Psychology, Four, 13, 325–350.
Eccles, J. S., Wigfield, A., Midgley, C., Reuman, D., Iver, D. M., & Feldlaufer, H. (1993). Negative effects of traditional middle schools on students’ motivation. The Elementary School Journal, 93, 553–574. doi:10.1086/461740.
Elgar, F. J., Napoletano, A., Saul, G., Dirks, M. A., Craig, W., Poteat, V. P., et al. (2014). Cyberbullying victimization and mental health and the moderating role of family dinners. JAMA Pediatrics, 168(11), 1015–1022. doi:10.1001/jamapediatrics.2014.1223.
Elkind, D. (1967). Egocentrism in adolescence. Child Development, 38(4), 1025–1034.
Evans, E., Hawton, K., & Rodham, K. (2004). Factors associated with suicidal phenomena in adolescents: A systematic review of population-based studies. Clinical Psychology Review, 24, 957–979. doi:10.1016/j.cpr.2004.04.005.
Everall, R. D., Bostik, K. E., & Paulson, B. L. (2005). I’m sick of being me: Developmental themes in suicidal adolescent. Adolescence, 40, 693–708.
Farrington, D. P., & Ttofi, M. M. (2009). School-based programs to reduce bullying and victimization (Campbell Systematic Reviews No. 5). Oslow, Norway: Campbell Corporation. doi:10.4073/csr.2009.6.
Fekkes, M., Pijpers, F. I. M., Fredriks, A. M., Vogels, T., & Verloove-Vanhorick, S. P. (2006). Do bullied children get ill, or do ill children get bullied? A prospective cohort study on the relationship between bullying and health-related symptoms. Pediatrics, 117(5), 1568–1574. doi:10.1542/peds.2005-0187.
Fite, P. J., Stauffacher, K., Ostrov, J. M., & Colder, C. R. (2008). Replication and extension of Little et al’.s (2003) forms and functions of aggression measure. International Journal of Behavioral Development, 32, 238–242. doi:10.1177/0165025408089273.
Fleming, T. M., Merry, S. N., Robinson, E. M., Denny, S. J., & Watson, P. D. (2007). Self-reported suicide attempts and associated risk and protective factors among secondary school students in New Zealand. Australian and New Zealand Journal of Psychiatry, 41, 213–221.
Friedman, M. S., Koeske, G. F., Silvestre, A. J., Korr, W. S., & Sites, E. W. (2006). The impact of gender-role nonconforming behavior, bullying, and social support on suicidality among gay male youth. Journal of Adolescent Health, 38, 621–623. doi:10.1016/j.jadohealth.2005.04.014.
Fuligni, A. J., & Hardway, C. (2006). Daily variation in adolescents’ sleep, activities, and psychological well-being. Journal of Research on Adolescence, 16(3), 353–378.
Furman, W., Brown, B. B., & Feiring, C. (1999). The development of romantic relationships in adolescence. New York, NY: Cambridge University Press.
Galen, B. R., & Underwood, M. K. (1997). A developmental investigation of social aggression among children. Developmental Psychology, 33, 589–600. doi:10.1037/0012-1649.33.4.589.
Gillen-O’Neel, C., & Fuligni, A. (2013). A longitudinal study of school belonging and academic motivation across high school. Child Development, 84, 678–692. doi:10.1111/j.1467-8624.2012.01862.x.
Gini, G., & Pozzoli, T. (2009). Association between bullying and psychosomatic problems: A meta-analysis. Pediatrics: Official Journal of the American Academy of Pediatrics, 123(3), 1059–1065. doi:10.1542/peds.2008-1215.
Goldstein, S. E. (2011). Relational aggression in emerging adults’ friendships and romantic relationships. Personal Relationships, 18, 645–656.
Goldstein, S. E. (2015). Parental regulation of online behavior and cyber aggression: Adolescents’ experiences and perspectives. Cyberpsychology: Journal of Psychosocial Research on Cyberspace. doi:10.5817/CP2015-4-2.
Goldstein, S. E., Davis-Kean, P. E., & Eccles, J. S. (2005). Parents, peers, and problem behavior: A longitudinal investigation of the impact of relationship perceptions and characteristics on the development of adolescent problem behavior. Developmental Psychology, 41, 401–413.
Goldstein, S. E., Malanchuk, O., Davis-Kean, P. E., & Eccles, J. S. (2007). Risk factors for sexual harassment by peers: A longitudinal investigation of African American and European American adolescents. Journal of Research on Adolescence, 17, 285–300.
Goldstein, S. E., & Tisak, M. S. (2004). Adolescents’ outcome expectancies about relational aggression within acquaintanceships, friendships, and dating relationships. Journal of Adolescence, 27, 283–302.
Goldstein, S. E., & Tisak, M. S. (2006). Early adolescents’ conceptions of parental and friend authority over relational aggression. The Journal of Early Adolescence, 26, 344–364. doi:10.1177/0272431606288552.
Goldstein, S. E., & Tisak, M. S. (2010). Early adolescents’ social reasoning about relational aggression. Journal of Child and Family Studies, 19, 471–482.
Goldstein, S. E., Young, A., & Boyd, C. (2008). Relational aggression at school: Associations with school safety and social climate. Journal of Youth and Adolescence, 37, 641–654.
Graber, J. A., & Sontag, L. M. (2009). Internalizing problems during adolescence. Handbook of Adolescent Psychology, 1, 19. doi:10.1002/9780470479193.adlpsy00102.
Grolnick, W. S., & Raftery-Helmer, J. N. (2015). Contexts supporting self-regulated learning at school transitions. In T. Cleary (Ed.), Self-regulated learning interventions with at-risk youth: Enhancing adaptability, performance, and well-being (pp. 251–276). Washington, DC: American Psychological Association.
Gross, J. J., & John, O. P. (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85, 348–362.
Guerra, N. G., & Huesmann, L. R. (2004). A cognitive-ecological model of aggression. Revue Internationale de Psychologie Sociale, 2, 177–204.
Gullone, E., Hughes, E. K., King, N. J., & Tonge, B. (2010). The normative development of emotion regulation strategy use in children and adolescents: A 2-year follow-up study. The Journal of Child Psychology and Psychiatry, 51(5), 567–574. doi:10.1111/j.1469-7610.2009.02183.x.
Gvion, Y., & Apter, A. (2011). Aggression, impulsivity, and suicidal behavior: A review of the literature. Archives of Suicide Research, 15, 93–112. doi:10.1080/13811118.2011.565265.
Hansen, M., Janssen, I., Schiff, A., Zee, P. C., & Dubocovich, M. L. (2005). The impact of school daily schedule on adolescent sleep. Pediatrics: Official Journal of the American Academy of Pediatrics, 115, 1555–1561. doi:10.1542/peds.2004-1649.
Hase, C. N., Goldberg, S. B., Smith, D., Stuck, A., & Campain, J. (2015). Impacts of traditional bullying and cyberbullying on the mental health of middle school and high school students. Psychology in the Schools, 52(6), 607–617. doi:10.1002/pits.21841.
Hashiro, M., & Okumura, M. (1997). Anxiety, depression and psychosomatic symptoms in patients with atopic dermatitis: Comparison with normal controls and among groups of different degrees of severity. Journal of Dermatological Science, 14(1), 63–67. doi:10.1016/S0923-1811(96)00553-1.
Hatzenbuehler, M. L., Birkett, M., Wagenen, A. V., & Meyer, I. H. (2014). Protective school climates and reduced risk for suicide ideation in sexual minority youths. American Journal of Public Health, 104, 279–286. doi:10.2105/AJPH.2013.301508.
Hazelden Foundation. (2007). The Olweus bullying prevention program. Retrieved from http://www.violencepreventionworks.org/public/olweus_scope.page
Heikkila, H., Vaananen, J., Helminen, M., Frojd, S., Marttunen, M., & Kaltiala-Heino, R. (2013). Involvement in bullying and suicidal ideation in middle adolescence: A 2-year follow-up study. European Journal of Child and Adolescent Psychiatry, 22, 95–102. doi:10.1007/s00787-012-0327-0.
Hinduja, S., & Patchin, J. W. (2010). Bullying, cyberbullying, and suicide. Archives of Suicide Research, 14(3), 206–221. doi:10.1080/13811118.2010.494133.
Holt, M. K. (2015). Suicidal risk as a function of bullying and other victimization exposures. In P. Goldblum, D. L. Espelage, J. Chu, & B. Bongar (Eds.), Youth suicide and bullying: Challenges and strategies for prevention and intervention (pp. 31–38). New York, NY: Oxford University Press.
Hyde, J. S., Mesulis, A. H., & Abramson, L. Y. (2008). The ABCs of depression: Integrating affective, biological, and cognitive models to explain the emergence of the gender difference in depression. Psychological Review, 115, 291–313.
Johnson, D. P., & Whisman, M. A. (2013). Gender differences in rumination: A meta-analysis. Personality and Individual Differences, 55, 367–374. doi:10.1016/j.paid.2013.03.019.
Joiner, T. E., Jr. (2005). Why people die by suicide?. Cambridge, MA: Harvard University Press.
Joiner, T. E., Jr. (2010). Myths about suicide. Cambridge, MA: Harvard University Press.
Joiner, T. E., Jr., & Rudd, M. D. (1996). Disentangling the interrelations between hopelessness, loneliness, and suicidal ideation. Suicide and Life-Threatening Behavior, 26(1), 19–26. doi:10.1111/j.1943-278X.1996.tb00253.x.
Juhnke, G. A., Granello, P. F., & Lebrón-Striker, M. A. (2007). IS PATH WARM? A suicide assessment mnemonic for counselors (ACAPCD-03). Alexandria, VA: American Counseling Association.
Kaess, M., Parzer, P., Haffner, J., Steen, R., Roos, J., Klett, M., et al. (2011). Explaining gender differences in non-fatal suicidal behavior among adolescents: A population-based study. BMC Pubic Health, 11, 597–604. doi:10.1186/1471-2458-11-597.
Kaltiala-Heino, R., Fröjd, S., & Marttunen, M. (2010). Involvement in bullying and depression in a 2-year follow-up in middle adolescence. European Child and Adolescent Psychiatry, 19(1), 45–55. doi:10.1007/s00787-009-0039-2.
Kashden, J., Fremouw, W. J., Callahan, T. S., & Franzen, M. D. (1993). Impulsivity in suicidal and nonsuicidal adolescents. Journal of Abnormal Child Psychology, 21, 339–353.
Kim, Y. S., Koh, Y., & Leventhal, B. (2005). School bullying and suicidal risk in Korean middle school students. Pediatrics, 115(2), 357–363.
Kim, Y. S., & Leventhal, B. (2008). Bullying and suicide: A review. International Journal of Adolescent Medicine and Health, 20, 133–154. doi:10.1515/IJAMH.2008.20.2.133.
Kim, Y. S., Leventhal, B., Koh, Y., & Boyce, T. (2009). Bullying increased suicide risk: Prospective study of Korean adolescents. Archives of Suicide Research, 13, 15–30. doi:10.1080/13811110802572098.
Kloep, M., Hendry, L. B., Taylor, R., & Stuart-Hamilton, I. (2016). Development from adolescence to early adulthood: A dynamic systematic approach to transitions and transformations. New York, NY: Psychology Press.
Klomek, A. B., Marrocco, F., Kleinman, M., Schonfeld, I. S., & Gould, M. A. (2007). Bullying, depression, and suicidality in adolescents. Journal of the American Academy of Child and Adolescent Psychiatry, 46(1), 40–49. doi:10.1097/01.chi.0000242237.84925.18.
Klomek, A. B., Marrocco, F., Kleinman, M., Schonfeld, I. S., & Gould, M. A. (2008). Peer victimization, depression, and suicidality in adolescents. Suicide and Life-Threatening Behavior, 38(2), 166–180.
Klomek, A. B., Sourander, A., & Gould, M. (2010). The association of suicide and bullying in childhood to young adulthood: A review of cross-sectional and longitudinal research findings. The Canadian Journal of Psychiatry, 55(5), 282–288.
Lagerspetz, K. M. J., Bjorkqvist, K., & Peltonen, T. (1988). Is indirect aggression typical of females? Gender differences in aggressiveness in 11- to 12-year-old children. Aggressive Behavior, 14, 403–414. doi:10.1002/1098-2337(1988)14:6.
Larson, R., Csikszentmihalyi, M., & Graef, R. (1980). Mood variability in the psychosocial adjustment of adolescents. Journal of Youth and Adolescence, 9, 469–490.
Larson, R., Moneta, G., Richards, M. H., & Wilson, S. (2002). Continuity, stability, and change in daily emotional experience across adolescence. Child Development, 73, 1151–1165. doi:10.1111/1467-8624.00464.
Lasgaard, M., Goossens, L., & Elklit, A. (2011). Loneliness, depressive symptomatology, and suicide ideation in adolescence: Cross-sectional and longitudinal analyses. Journal of Abnormal Child Psychology, 39, 137–150. doi:10.1007/s10802-010-9442-x.
Laursen, B., Coy, K. C., & Collins, W. A. (1998). Reconsidering changes in parent-child conflict across adolescence: A meta-analysis. Child Development, 69, 817–832. doi:10.1111/j.1467-8624.1998.tb06245.x.
Lawson, K. M., Crouter, A. C., & McHale, S. M. (2015). Links between family gender socialization experiences in childhood and gendered occupational attainment in young adulthood. Journal of Vocational Behavior, 90, 26–35. doi:10.1016/j.jvb.2015.07.003.
Lereya, S. T., Copeland, W. E., Costello, E. J., & Wolke, D. (2015). Adult mental health consequences of peer bullying and maltreatment in childhood: Two cohorts in two countries. The Lancet Psychiatry, 2(6), 524–531. doi:10.1016/S2215-0366(15)00165-0.
Lerner, R. M., & Steinberg, L. (2004). Handbook of adolescent pscyhology (2nd ed.). Hoboken, NJ: Wiley.
LeVasseur, M. T., Kelvin, E. A., & Grosskopf, N. A. (2013). Intersecting identities and the association between bullying and suicide attempt among New York City youths: Results from the 2009 New York City Youth Risk Behavior Survey. American Journal of Public Health, 103(6), 1082–1089. doi:10.2105/AJPH.2012.300994.
Levitt, M. J., Guacci-Franco, N., & Levitt, J. L. (1993). Convoys of social support in childhood and early adolescence: Structure and function. Developmental Psychology, 29, 811–818. doi:10.1037/0012-1649.29.5.811.
Lewis, S. A., Johnson, J., Cohen, P., Garcia, M., & Velez, C. N. (1988). Attempted suicide in youth: Its relationship to school achievement, educational goals, and socioeconomic status. Journal of Abnormal Child Psychology, 16(4), 459–471.
Little, T. D., Jones, S. M., Henrich, C. C., & Hawley, P. H. (2003). Disentangling the ‘whys’ from the ‘whats’ of aggressive behavior. International Journal of Behavioral Development, 27(2), 122–133. doi:10.1080/01650250244000128.
Litwiller, B. J., & Brausch, A. M. (2013). Cyber bullying and physical bullying in adolescent suicide: The role of violent behavior and substance use. Journal of Youth and Adolescence, 42, 675–684. doi:10.1007/s10964-013-9925-5.
Loeber, R., & Farrington, D. P. (2000). Young children who commit crime: Epidemiology, developmental origins, risk factors, early interventions, and policy implications. Development and Psychopathology, 12, 737–762.
Lord, S. E., Eccles, J. S., & McCarthy, K. A. (1994). Surviving the junior high school transition: Family processes and self-perceptions as protective and risk factors. The Journal of Early Adolescence, 14, 162–199. doi:10.1177/027243169401400205.
Lundgren, R., & Amin, A. (2015). Addressing intimate partner violence and sexual violence among adolescents: Emerging evidence of effectiveness. Journal of Adolescent Health, 56(1), S42–S50. doi:10.1016/j.jadohealth.2014.08.012.
Mason, A. (2016). Mother hopes teen’s death can spark change. York Daily Record. Retrieved from http://www.ydr.com/story/opinion/columnists/2016/02/05/mother-hopes-teens-death-can-spark-change/79459842/.
Matthiesen, S. B., & Einarsen, S. (2004). Psychiatric distress and symptoms of PTSD among victims of bullying at work. British Journal of Guidance and Counseling, 32(3), 335–356. doi:10.1080/03069880410001723558.
Mayes, S. D., Baweja, R., Calhoun, S. L., Syed, E., Mahr, F., & Siddiqui, F. (2014). Suicide ideation and attempts and bullying in children and adolescents: Psychiatric and general population samples. Crisis: The International Journal of Crisis Intervention and Suicide Prevention, 35(5), 301–309. doi:10.1027/0227-5910/a000264.
McElhaney, K. B., Allen, J. P., Stephenson, J. C., & Hare, A. L. (2009). Attachment and autonomy during adolescence. In R. M. Lerner & L. Steinberg (Eds.), Handbook of adolescent psychology (3rd ed., pp. 358–403). Hoboken, NJ: Wiley.
McRae, K., Gross, J. J., Weber, J., Robertson, E. R., Sokol-Hessner, P., Ray, R., et al. (2012). The development of emotion regulation: An fMRI study of cognitive reappraisal in children, adolescents and young adults. Social Cognitive and Affective Neuroscience, 7(1), 11–22. doi:10.1093/scan/nsr093.
Meeus, W., & Dekovic, M. (1995). Identity development, parental and peer support in adolescence: Results of a national Dutch survey. Adolescence, 30(120), 931–944.
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129(5), 674–697. doi:10.1037/0033-2909.129.5.674.
Moore, S. E., Norman, R. E., Sly, P. D., Whitehouse, A. J. O., Zubrick, S. R., & Scott, J. (2014). Adolescent peer aggression and its association with mental health and substance use in an Australian cohort. Journal of Adolescence, 37, 11–21. doi:10.1016/j.adolescence.2013.10.006.
Morrison, R., & O’Connor, R. C. (2008). A systematic review of the relationship between rumination and suicidality. Suicide and Life-Threatening Behavior, 38, 523–538.
Mueller, A. S., James, W., Abrutyn, S., & Levin, M. L. (2015). Suicide ideation and bullying among US adolescents: Examining the intersections of sexual orientation, gender, and race/ethnicity. American Journal of Public Health, 105(5), 980–985. doi:10.2105/AJPH.2014.302391.
National Center for Injury Prevention and Control. Center for Disease Control and Prevention. (2013). The relationship between bullying and suicide: What we know and what it means for schools. Retrieved from http://www.cdc.gov/violenceprevention/pdf/bullying-suicide-translation-final-a.pdf.
National Center for Injury Prevention and Control. Center for Disease Control and Prevention. (2015). Suicide: Facts at a Glance. Retrieved from http://www.cdc.gov/violenceprevention/pdf/suicide-datasheet-a.PDF.
Nolen, S., & Jackson, B. (2001). Mediators of the gender difference in rumination. Psychology of Women Quarterly, 25, 37–47. doi:10.1111/1471-6402.00005.
Nolen, S., Larson, J., & Grayson, C. (1999). Explaining the gender difference in depressive symptoms. Journal of Personality and Social Psychology, 77, 1061–1072. doi:10.1037/0022-3514.77.5.1061.
Olweus, D. (1978). Aggression in the schools: Bullies and whipping boys. Washington, DC: Hemisphere Publishing Corp.
Olweus, D. (1993). Victimization by peers: Antecedents and long-term outcomes. In K. H. Rubin & J. B. Asendorpf (Eds.), Social withdrawal, inhibition, and shyness in childhood (pp. 315–342). New York, NY: Psychology Press.
Olweus, D., & Limber, S. P. (2010). Bullying in school: Evaluation and dissemination of the Olweus Bullying Prevention Program. American Journal of Orthopsychiatry, 80(1), 124–134. doi:10.1111/j.1939-0025.2010.01015.x.
Ortin, A., Lake, A. M., Kleinman, M., & Gould, M. S. (2012). Sensation seeking as risk factor for suicidal ideation and suicide attempts in adolescence. Journal of Affective Disorders, 143(1–3), 214–222. doi:10.1016/j.jad.2012.05.058.
Österman, K., Björkqvist, K., Lagerspetz, M. J., Charpentier, S., Caprara, G. B., & Pastorelli, C. (1999). Locus of control and three types of aggression. Aggressive Behavior, 25, 61–65. doi:10.1002/(SICI)1098-2337(1999)25:1%3c61::AID-AB6%3e3.0.CO;2-G.
Page, R. M., Yanagishita, J., Suwanteerangkul, J., Zaro, E. P., Mei-Lee, C., & Miao, N. (2006). Hopelessness and loneliness among suicide attempters in school-based samples of Taiwanese, Philippine, and Thai adolescents. School Psychology International, 27(5), 583–598. doi:10.1177/0143034306073415.
Paquette, J. A., & Underwood, M. K. (1999). Gender differences in young adolescents’ experiences of peer victimization: Social and physical aggression. Merrill-Palmer Quarterly, 45, 242–266.
Puhl, R. M., Peterson, J. L., & Luedicke, J. (2013). Weight-based victimization: Bullying experiences of weight loss treatment-seeking youth. Pediatrics, 131, e1–e9. doi:10.1542/peds.2012-1106.
Racz, S. J., & McMahon, R. J. (2011). The relationship between parental knowledge and monitoring and child and adolescent conduct problems: A 10-year update. Clinical Child and Family Psychology Review, 14, 377–398. doi:10.1007/s10567-011-0099-y.
Reed, K. P., Nugent, W., & Cooper, R. L. (2015). Testing a path model of relationships between gender, age, and bullying victimization and violent behavior, substance abuse, depression, suicidal ideation, and suicide attempts in adolescents. Children and Youth Services Review, 55, 128–137. doi:10.1016/j.childyouth.2015.05.016.
Rigby, K., & Slee, P. T. (1999). Suicidal ideation among adolescent school children, involvement in bullying-victim problems, and perceived social support. Suicide and Life-Threatening Behavior, 29(2), 119–130. doi:10.1111/j.1943-278X.1999.tb01050.x.
Roberts, R. E., & Chen, Y. (1995). Depressive symptoms and suicidal ideation among Mexican-Origin and Anglo adolescents. Journal of the American Academy of Child and Adolescent Psychiatry, 34(1), 81–90. doi:10.1097/00004583-199501000-00018.
Roeser, R. W., & Eccles, J. S. (1998). Adolescents’ perceptions of middle school: Relation to longitudinal changes in academic and psychological adjustment. Journal of Research on Adolescence, 88, 123–158. doi:10.1207/s15327795jra0801_6.
Roland, E. (2002). Bullying, depressive symptoms and suicidal thoughts. Educational Research, 44(1), 55–67.
Rubin, K. H., Coplan, R., Chen, X., Buskirk, A. A., & Wojslawowicz, J. C. (2005). Peer relationships in childhood. In T. P. Gullotta & M. Bloom (Eds.), Encyclopedia of primary prevention and health promotion (2nd ed., pp. 808–812). New York, NY: Springer.
Russell, S. T., & Joyner, K. (2001). Adolescent sexual orientation and suicide risk: Evidence from a national study. American Journal of Public Health, 91(8), 1276–1281.
Safren, S. A., & Pantalone, D. W. (2006). Social anxiety and barriers to resilience among lesbian, gay, and bisexual adolescents. In A. M. Omoto & H. S. Kurtzman (Eds.), Sexual orientation and mental health: Examining identity and development in lesbian, gay, and bisexual people (pp. 55–71). Washington, DC: American Psychological Association.
Salmon, G., James, A., & Smith, D. M. (1998). Bullying in schools: Self reported anxiety, depression, and self-esteem in secondary school children. British Medical Journal, 317, 924–925. doi:10.1136/bmj.317.7163.924.
Schneider, S. K., O’Donnell, L., Stueve, A., & Coulter, R. W. S. (2012). Cyberbullying, school bullying, and psychological distress: A regional census of high school students. American Journal of Public Health, 102, 171–177. doi:10.2105/AJPH.2011.300308.
Schrijvers, D. L., Bollen, J., & Sabbe, B. G. C. (2012). The gender paradox in suicidal behavior and its impact on the suicidal process. Journal of Affective Disorders, 138(1–2), 19–26. doi:10.1016/j.jad.2011.03.050.
Shulman, E. P., Smith, A. R., Silva, K., Icenogle, G., Duell, N., Chein, J., et al. (2016). The dual systems model: Review, reappraisal, and reaffirmation. Developmental Cognitive Neuroscience, 17, 103–117. doi:10.1016/j.dcn.2015.12.010.
Simmons, R. G., & Blyth, D. A. (1987). Moving into adolescence: The impact of pubertal change and school context. New York, NY: Aldine De Gruyter.
Sinyor, M., Schaffer, A., & Cheung, A. H. (2014). An observational study of bullying as a contributing factor in youth suicide in Toronto. Canadian Journal of Psychiatry, 59(12), 632–638.
Smetana, J. G. (1995). Parenting styles and conceptions of parental authority during adolescence. Child Development, 66, 299–316.
Smetana, J. G. (2000). Middle-class American adolescents’ and parents’ conceptions of parental authority and parenting practices: A longitudinal investigation. Child Development, 71, 1672–1686. doi:10.1111/1467-8624.00257.
Smetana, J. G., & Asquith, P. (1994). Adolescents’ and parents’ conceptions of parental authority and personal autonomy. Child Development, 65, 1147–1162. doi:10.1111/j.1467-8624.1994.tb00809.x.
Smith, L. (2015). ‘No one knows how much I am suffering inside’: The heartwrenching video diary of a beautiful teen who was driven to suicide by bullying and depression…and her family’s determination her death will not be in vain. The Daily Mail. Retrieved from http://www.dailymail.co.uk/news/article-3216601/No-one-knows-suffering-inside-heartwrenching-video-diary-beautiful-teen-driven-suicide-bullying-depression-family-s-determination-death-not-vain.html.
Smith, A. R., Chein, J., & Steinberg, L. (2013). Impact of socio-emotional context, brain development, and pubertal maturation on adolescent risk-taking. Hormones and Behavior, 64, 323–332. doi:10.1016/j.yhbeh.2013.03.006.
Smith, C. A., Greenman, S. J., Thornberry, T. P., Henry, K. L., & Ireland, T. O. (2015). Adolescent risk for intimate partner violence perpetration. Prevention Science, 16, 862–872. doi:10.1007/s11121-015-0560-0.
Star Ledger Staff. (2011). New details revealed in Rutgers webcam suicide case. NJ.com. Retrieved from http://www.nj.com/news/index.ssf/2011/08/rutgers_suicide_new_details_re.html.
Steinberg, L. (2008). A social neuroscience perspective on adolescent risk-taking. Developmental Review, 28(1), 78–106. doi:10.1016/j.dr.2007.08.002.
Strategies. (2016). In National Crime Prevention Council. Retrieved from http://www.ncpc.org/topics/bullying/strategies.
Suicide Statistics. (2016, March 04). Retrieved from http://www.befrienders.org/suicide-statistics.
Takizawa, R., Maughan, B., & Arseneault, L. (2014). Adult health outcomes of childhood bullying victimization: Evidence from a five-decade longitudinal British birth cohort. The American Journal of Psychiatry, 171, 777–784. doi:10.1176/appi.ajp.2014.13101401.
Tilton-Weaver, L. C., Burk, W. J., Kerr, M., & Stattin, H. (2013). Can parental monitoring and peer management reduce the selection or influence of delinquent peers? Testing the question using a dynamic social network approach. Developmental Psychology, 49, 2057–2070. doi:10.1037/a0031854.
Turner, H. A., Finkelhor, D., Hamby, S. L., Shattuck, A., & Ormrod, R. K. (2011). Specifying type and location of peer victimization in a national sample of children and youth. Journal of Youth and Adolescence, 40, 1052–1067.
Underwood, M. K. (2003). Social aggression among girls. New York, NY: Guilford Press.
Undheim, A. M. (2013). Involvement in bullying as predictor of suicidal ideation among 12- to 15-year-old Norwegian adolescents. European Journal of Child and Adolescent Psychiatry, 22, 357–365. doi:10.1007/s00787-012-0373-7.
Van der Wal, M. F., de Wit, C. A. M., & Hirasing, R. A. (2003). Psychosocial health among young victims and offenders of direct and indirect bullying. Pediatrics, 111(6), 1312–1317.
Van Geel, M., Vedder, P., & Tanilon, J. (2014). Relationship between peer victimization, cyberbullying, and suicide in children and adolescents: A meta-analysis. JAMA Pediatrics, 168, 435–442. doi:10.1001/jamapediatrics.2013.4143.
Van Orden, K. A., Witte, T. K., Cukrowicz, K. C., Braithwaite, S., Selby, E. A., & Joiner, T. E., Jr. (2010). The interpersonal theory of suicide. Psychological Review, 117(2), 575–600. doi:10.1037/a0018697.
Waasdorp, T. E., & Bradshaw, C. P. (2015). The overlap between cyberbullying and traditional bullying. Journal of Adolescent Health, 56, 483–488. doi:10.1016/j.jadohealth.2014.12.002.
Wasserman, D., Cheng, Q., & Jiang, G. (2005). Global suicide rates among young people aged 15–19. World Psychiatry, 4(2), 114–120.
Whitney, I., & Smith, P. K. (1993). A survey of the nature and extent of bullying in junior/middle and secondary schools. Educational Research, 35, 3–25. doi:10.1080/0013188930350101.
Wigfield, A., Byrnes, J. P., & Eccles, J. S. (2006). Development during early and middle adolescence. In P. A. Alexander & P. H. Winne (Eds.), Handbook of educational psychology (2nd ed., pp. 87–114). New York, NY: Routledge.
Wunderlich, U., Bronisch, T., Wittchen, H. U., & Carter, R. (2001). Gender differences in adolescents and young adults with suicidal behaviour. Acta Psychiatrica Scandinavica, 104, 332–339. doi:10.1111/j.1600-0447.2001.00432.x.
Zeman, J., Cassano, M., Perry-Parrish, C., & Stegall, S. (2006). Emotion regulation in children and adolescents. Developmental and Behavioral Pediatrics, 27(2), 155–168. doi:10.1097/00004703-200604000-00014.
Zernike, K. (2012). Jail term ends after 20 days for ex-Rutgers student. The New York Times. Retrieved from http://www.nytimes.com/2012/06/20/nyregion/dharun-ravi-ex-rutgers-student-who-spied-leaves-jail.html.
Zimmer-Gembeck, M. J., Ducat, W. H., & Collins, W. A. (2011). The development of autonomy. In B. B. Brown & M. Pearlstein (Eds.), Encyclopedia of adolescence (Vol. 1, pp. 66–76). Amsterdam, The Netherlands: Elsevier.
Authors’ Contributions
J.G. conceived of the topic, worked on collecting articles, drafted the initial draft of the manuscript, and worked on subsequent drafts, S.G. refined the topic to be reviewed, aided in collecting articles, aided in drafting the manuscript, and suggested revisions to the manuscript throughout development of the manuscript. Both authors have read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflict of interests.
Ethical Approval
This article did not make use of participants or a research design. No ethical approval was required.
Informed Consent
This article made no use of participants or a research design. No informed consent was necessary.
Rights and permissions
About this article

Cite this article
Gunn, J.F., Goldstein, S.E. Bullying and Suicidal Behavior During Adolescence: A Developmental Perspective. Adolescent Res Rev 2, 77–97 (2017). https://doi.org/10.1007/s40894-016-0038-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40894-016-0038-8