
Abstract
This article introduces the Ethics Laboratory as an inter-sectorial and cross-disciplinary dialogical forum which can be viewed as an educational tool for moral learning. The Ethics Laboratory represents a platform for the informal, collaborative investigation, in strict confidentiality, of ethical questions that have social consequences and/or legal concerns and bridges boundaries between research communities, institutions and patients. Its methodological structure proposes an experimental, open-ended way of unpacking implied assumptions, underlying values, comparable notions and observations from different professional fields. In connection with a large social science project on precision medicine, we conducted four Ethics Laboratories followed by eight interviews with a selected number of participants. Through these interviews we learnt how this exploratory dialogical forum heighten moral awareness on issues that are shared among stakeholders who work to implement precision medicine in Denmark. Though the framework was developed specifically to foster ethical reflection within precision medicine, its dialogical structure lends itself to other professional areas and can easily be adopted and carried out.
Similar content being viewed by others


Background
Moral variables permeate professional situations within the emerging field of precision medicine. In the past, the absence of clear pathways in moral assessment and decision-making have led to the creation of various forms of ethics support systems in clinical practice (Rasoal et al. 2017; Förde and Pedersen 2011; Slowther et al. 2012) and institutional review boards with regulatory governance frameworks or research ethics committees (Thomson 2012; Pickworth 2000). Some countries have listed a number of ethical competencies to be adopted by professionals serving on ethics councils through, for example, course training. With the aim of enhancing moral reflection, most courses and training programs have specific learning objectives, such as being acquainted with moral theory and ethical assessment skills (e.g. Beauchamp and Childress 2009; Core Competencies Task Force 2011; Molewijk et al. 2008a, b). These formal mechanisms are put in place to secure an ethical infrastructure and compliance with standards of moral conduct. However, how can moral awareness be cultivated outside of committees, boards and courses such as these? How may professionals address and learn from morally complex situations in an informal setting? How can a confidential space be created where health care stakeholders can engage with each other about the moral concerns weighing on their minds? In other words, how can a moral dialogue that runs across disciplines, sectors and institutions be facilitated?
Researchers within the medical humanities and social sciences explore medical technology and science, while simultaneously harboring an urge to contribute to ethical practices. Impact and output are often measured in written products, such as research articles or reports. Other times, feedback takes the form of a brief presentation at the ethnographic site as a way to infuse obtained data back into the field. It is, however, unknown to what extent the results of the empirical work are read or incorporated by the practitioners and scientists involved. Though most social scientists do not view their research in a formative perspective, we became intrigued in the process by the ethics lab’s potential as a learning tool. In our current research on the introduction of precision medicine in Danish health care we faced the challenge of how to not only investigate the ethical, organizational, and legal challenges, but to make our investigation feed into the very practices we engaged in. In the following we describe how we developed and experimented with a format where the preliminary insights from our qualitative research was the starting point for a collaboration that sought to both strengthen ethical reflection in the field and create new data for the ethnographers. We proposed a dialogical forum entitled the Ethics Laboratory.
New developments in genetics and omics technologies have propelled the field of precision medicineFootnote 1 around the world (Lau 2018; Chen 2013). Precision medicine refers to therapeutic and preventive measures tailored to patients’ needs based on pooling a substantial variety of data, including data on genetic make-up, life style and environment (De Marchiano et al. 2021; Prainsack 2017) with the aim of more targeted interventions. The knowledge production and application of precision medicine is carried out in a combined effort by multiple professionals with diverse backgrounds. Oncologists in phase 1-trials see themselves collaborating with a private pharmaceutical company in the development of pathway-specific drugs or, in laboratories, molecular biologists and pathologists move closer to clinicians, rescinding the traditional gap between bench and bedside, basic science and clinic.
Precision medicine is conditioned by the fact that data from the individual can be compared with data from thousands of others. The tension between “individualistic promises of personalized medicine and the common good” is a recurrent theme in the literature (Van Beers et al. 2018, back cover; Dickenson 2013; Prainsack 2018; Reardon 2017). This fundamental aspect implies that the personal ‘me’ and the collective ‘we’ become mutually shaped in precision medicine. In particular, precision medicine puts emphasis on genomic data and seeks to reach precise diagnoses based on comparing the genome of a single individual with the genomes of others. With the steep decline in cost of genetic sequencing and the improvement of analysis algorithms, more precise therapeutic targeting can enhance patient care, yet ethical issues related to, for example, selection of patients, the interpretation of uncertain knowledge, and the exchange of data in a transnational field abound. While we are not the first to identity these issues (Vollmann et al. 2015; Reardon 2017; Prainsack 2017; Kerr et al. 2021), we wanted to experiment with new ways for stakeholders, our own team included, to understand and address the ethics at stake in the interdisciplinary field of precision medicine.
What is the ethics laboratory?
The architectural blueprint of the Ethics Laboratory is based on a dialogue that takes inspiration from Socratic midwifery (Plato 1992), encouraging collaborative musings on a particular subject and adopting an enquiring mindset. Following the Socratic tradition of helping to birth thoughts in each other, it aims at creating an open-ended and non-judgmental platform; a free and informal space for moral deliberation where participants can share experiences and conceptualize moral questions. The mutualizing act of understanding that runs through the ethics laboratory embodies the Gadamerian concept of fusion of horizons (Gadamer 2004, p. 337) where new perspectives are unearthed through a united exploration (Knox 2021).
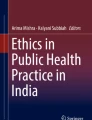
The dialogue follows a specific structure (see Fig. 1) that centers around two exercises. In the first exercise participants are given time to quietly mull over a concrete example from their own professional field that illustrates the theme in the lab. The personal choice of an example has the dual purpose of engaging participants in the lab and enabling the individual experience of a general theme. The example is subsequently converted to a poster size post-it that is hung on the wall. In interdisciplinary pairs of two, participants stand in front of their poster and help each other delve into the ethical content in each other’s example (exercise 2). Eventually, all participants in the ethics lab gather to share thoughts and observations on the experience and the theme. The three-hour long session of each lab gives ample time to educe participants’ concerns and interact with others.

Phases in an ethics laboratory
The Ethics Laboratory is embedded in the Danish research project MeInWe.Footnote 2 The second author is PI on this five-year study of the ethical, regulatory and organizational challenges lodged in the strategies of tailoring diagnosis and treatment to individual genetic variability in Denmark. The first author is responsible for the construction, planning and execution of the ethical dialogues with the empirical fields within the project. MeInWe consists of 15 scholars from a variety of academic fields: anthropology, sociology, political science, biology, public health, law, and philosophy. The project came on the heels of the Danish Government’s National Health Strategy on personalized medicineFootnote 3 and was instituted, independently from the national strategy, to study the implementation of personalized medicine within oncology, cardiology, diabetes care and clinical genetics.
Bringing people together to reflect on questions in precision medicine
Medical and social science, health care practices and health policies are inherently a moral enterprise (Fowers 2020; Molewijk et al. 2008a, b; Brandt and Rozin 1997) as they concern human goods (e.g. early detection to increase the efficacy of a preventive therapy) and right action (e.g. informing or not informing patients with a rare gene variant for which there is currently no treatment). Since the beginning of bioethics, the many fields of human health have caused ethically convoluted and poignant questions. Precision medicine is no exception.
In order to specify the dialogue’s thematic crux, several meetings were held within the MeInWe research group to hone prevalent ethical questions of our ethnographers and the healthcare professionals we were in contact with. In our preparatory meetings we extracted four common moral themes from the multiple sites we visited. Subsequently, we decided on four ethics labs. Each lab would have its own theme. The first ethics lab addressed the theme of selection. The Danish National policy on precision medicine initiated in 2016 a framework for a selection of patient groups that should have the opportunity to be offered a whole genome sequencing. But which ethical criteria are prevalent in patient group selection? And how is selection part of molecular analysis, diagnostics, treatment and prevention in the clinic? Our second ethics lab attended to data sharing and data exchange as data journeys across disciplines, sectors and countries. Medical and health sciences have seen an exponential growth of healthcare data in recent times. Data is the platform on which all precision medicine rests and raises questions such as with whom can data be shared? In what form and under what conditions? What does it mean to ensure anonymity and privacy when data travels across borders?
Precision medicine has caused an explosion of data, yet data does not speak for itself. The theme for the third ethics lab was interpretation. Interpretation challenges familiar categories such as sick and healthy, normal and abnormal. It may be that, for example, a whole genome analysis exposes the presence of a certain gene variant, but is it pathogenic or not? And how should we draw the line between the normal and the abnormal if it cannot be determined with certainty? When is a finding ‘actionable’ (information to be acted on)?
Precision medicine cannot be developed in a padlocked public health system. The field involves collaborations with sequencing companies, informatics businesses, with the pharmaceutical industry, both within and outside of Denmark. For the last ethics lab we chose the theme private-public partnerships. What is public and what is private may no longer be that easy to delineate. Is a BGI (Beijing Genomics Institute) sequencing machine, which was purchased by the University of Copenhagen with public funds, but operated by BGI Europe located in Copenhagen actually public or private? What are the challenges—legally and in terms of public legitimacy—when data moves between actors and can be used for different purposes and stay in different places at the same time? In the era of precision medicine, does it even make sense to distinguish between private and public? The many questions of precision medicine describe its ethical depth and width and the plethora of disciplines involved. Due to the magnitude, not only in quantity but intricacy and in view of societal ramifications, the questions also point to the urgency of addressing them by stakeholders.
In our preparation, we also discussed who to invite among the vast pool of collaborators. As we are collaborating with busy people in high-level positions, the close professional relationships we had created over the years greatly benefitted us in planning the four labs. After we made a list of candidates, we selected who among the MeInWe group would participate to ensure some familiarity among our collaborators as we invited them to visit our work place whereas, previously, it had been our ethnographers visiting them in their work environment. Discussing moral concerns with strangers can be a daunting enterprise and we needed to create an environment of trust for the mutual exchange. In the Ethics Laboratory our collaborators ceased to be solely informants contributing to our study. Together we joined forces as professionals engaged in shaping precision medicine as a technology and as agents in the Danish healthcare system. Email invitations were sent to our collaborators explaining the structure and intent of the ethics laboratory.
As responses to our invitation came in, dates for the ethics labs were arranged. A total of 31 people participated in the labs: 20 participants came from outside the research group, i.e. our pool of collaborators, and 11 from inside the MeInWe group. Interviews were delayed due to the Covid-19 pandemic and thus conducted up to fifteen months after the first lab in December 2019. The second lab took place right before the national lock down in March 2020 and two were carried out in the Fall of 2020. All participants met at the Department of Public Health (University of Copenhagen) for their lab session. In order to better understand how participants perceived the ethics lab, and in that way also assess the lab design, first author conducted interviews with 8 participants. The interviews were conducted between February 23rd and April 27th 2021. We selected participants from all ethics labs to have all four groups and the four topics well represented. Through the interview participants could explain what they had gained from their participation in an ethics lab and how they had processed it. Once all interviews had been conducted and transcribed, we systematically studied the interviewee responses for recurrent themes in perception of the ethics lab to identify overall impression and impact. This article is informed by the interviews on what participants learnt as well as the two authors’ informal conversations about the purpose and possible outcome with numerous participants during the labs.
Generating a moral ecosystem
According to the interviewees, a growing moral awareness evolved in the lab context through the collision of and collaboration on notions and values from cross professional fields. This moral awareness acted like an ecosystem. The diversity of the professionals’ moral gazes was brought into the lab to flow through the system (i.e. the dialogue) where they were broken down and assembled anew. Thus, moral viewpoints went through an organic process that sometimes led to the evaporation of them, either wholly or partially, or the germination of something slightly different from before the lab. This organic process was particularly vibrant in exercise 2 as it aspires to abet the dialogue partner’s moral reasoning through mutual curiosity and continual probing. Analogous to other eco-systems, the moral lab was an open system with porous borders where the world outside the lab brought oxygen (i.e. knowledge, expertise and experience) into the lab while the deliberation process inside the lab was free to migrate to the outside world after the lab.
Being paired with someone from another professional field than one’s own to reflect on a moral concern was particularly interesting to the participants in helping to a greater moral awareness. Participants often remarked on the benefit of standing in front of their poster with their partner in what we could call ‘a dialogical incubator’. Within this micro moral ecosystem, they formed a team that cultivated the specifics in their two examples to assist each other and pave the way for better understanding of both one’s own example and that of one’s partner. In exercise 2, participants are forced to develop and communicate others’ perceptions and suspend the mindset of evaluating them. This dialogue was not limited, of course, to exercise 2 as the exercise is followed by a plenary discussion on findings. Illustrating the underlying Socratic and Gadamerian foundation of the Ethics Laboratory, and in the words of one interviewee, the ethics laboratory became “an eye opener for [the importance of] spending more time on understanding and dialogue rather than just exchanging opinions on something.” The hermeneutical stance that is embedded in the laboratory structure emphasizes the meeting of diverging moral positionings. Grappling with others’ perceptions in a joint effort to decode a theme helped enhance moral discernment and learning. However, it is worth mentioning that several interviewees emphasized the importance of having time alone in the beginning of the lab to contemplate within and find an appropriate and concise example of the lab theme (e.g. interpretation or data) as it, in their minds, added “depth to the conversation that followed” as one interviewee explained.
By being paired with someone from a different profession, our participants were forced to explain something without using a convoluted terminology. In the dialogical process, it was our experience that participants were confirmed in that the moral challenges they face in their home environment are, in fact, general and translatable to other fields despite having different manifestations. As one participant worded it “I find it nice to be confirmed in the challenges that I see in my work with precision medicine - that they are more general.” She continued by pointing out that she found important “insight […] in talking together across disciplines and sectors.” While they found valuable commonalities in regards to their moral concerns, they also gained an informative glimpse of dissimilar logics and approaches of other professional fields. In breaks during the labs and in subsequent interviews, we learnt that participants found the cross-disciplinary and inter-sectorial set-up as instrumental for diminishing silo thinking that, otherwise, tends to obstruct the natural flow in the moral eco-system.
By openly dissecting perspectives, the ethics labs cultivate a moral sensitivity that embraces a willingness to question the limits of one’s own practice and express moral concern. Conceptualized as an awareness of both the rational and affective aspect of the moral deliberative process (Kraaijeveld et al. 2020), one interviewee, a precision oncologist, expressed moral sensitivity when being inquisitive about cancer patient selection for clinical trials, questioning both the timing in offering precision treatment (“at the moment of diagnosis or after standardized treatment,” she conjectured), the difficulty in selecting suitable candidates and the challenge of delivering bad news when a patient is deemed ‘not suited’ for a clinical trial. Though these thoughts did originate from her participation in the ethics Lab, she did share in her interview with first author that it had, nevertheless, made her particularly conscious of how a morally attuned awareness “arises in the dialogue with the others;” a sentiment that was shared by the other interviewees.
“Precision medicine is still for the very few,” this precision oncologist professed, which calls for being acutely aware of “the ethical challenges in what we do and the effects on patients of not being selected,” she explained. This moral attunement can sensitize professionals to recognize ethical issues more quickly as they arise. Activating this form of sensitivity through dialogue helps participants better verbalize and understand personal moral stance vis-à-vis important and troubling aspects of their profession. It generates moral consciousness that may have been dormant in their work while, now, come to the forefront of their practice. As we saw earlier, this sensitivity is also at work when investigating diverging ethical perspectives between professionals and professions. In this view, the Ethics Laboratory maps out the interrelatedness of perspectives more than offering prescriptive criteria for determining boundaries. They lead not to moral conclusions or recommendations. Rather, they hold space for the moral variables within a theme to be explored phenomenologically, allowing participants to become more well-versed in the skill of honing a moral subject matter. Holding space for these multi-sided considerations allow for a firmer foundation for normative judgments than when made instinctively or subconsciously.
The moral sensitivity that the dialogues revealed seemed at times to be integrally linked to what the American philosopher Mark Johnson calls moral imagination (Johnson 1993). Moral imagination is the “ability to imaginatively discern various possibilities for acting in a given situation and to envision the potential help and harm that are likely to result from a given situation” (Johnson 1993, p. 202). Thus, sensitivity opens the door to envisioning different viewpoints and probable courses of actions with the possibility of expanding cognitive and affective horizons. “I left with new perspectives that I hadn’t considered before because I hadn’t carefully looked at our topic [interpretation] from other professional angles,” as a health lawyer summed up in her interview. She is referring to how, in her ethics lab, a biostatistician, two clinical geneticists, a precision oncologist and a governmental chief administrator offered differing interpretations of ‘anonymity’ and the protection of personal data. The clinicians were equally worried about overstepping some legal boundary by retrieving genetic data that is protected and frustrated seeing that they were often unable to get clear juridical advice in how to interpret the law. The governmental chief administrator in the group added a different perspective that pointed to how a comprehensive written consent form signed by patients who are getting a whole genome sequencing analysis secures the protection of patient data. The biostatistician explained in her interview how she found herself in between the clinical geneticists on the one hand, and the governmental chief administrator and the lawyer on the other hand. The stakes for her are not as high as the clinicians because her work involves registers and, thus, she is not responsible for a patient’s treatment or even in direct contact with patients. Yet, in her work she can potentially identify patients if she receives a strata or a subgroup with less than 5 individuals.
When interdisciplinarity becomes a premise for collaboration, as in the case of precision medicine, research traditions and professional worldviews are bought into close contact. This contact can cause confusion and discomfort as concepts clash despite being, on the outset, self-explanatory as, for example, in the case of ‘anonymity.’ The multi-dimentional aspect of ‘anonymity’ that surfaced in the dialogue made the biostatistician and others, in the end, more cognizant of its conceptual fluidity as a result of the range of professional uses. Emancipating ‘anonymity’ from their own particular use to imagine other interpretations serves as an educational illustration that they can draw on when working in future interdisciplinary collaborations.
A social scientist who participated in another lab alluded to a similar experience when she shared, in her interview, the observation of how perceptions were tested by investigating each others’ practices, explaining how “participants discovered something in each other, something that they wondered about and then got a chance to discuss.” Through the dialogical feedback, particularly in the case of exercise 2 and the collective deliberation that follows, imagined alternatives and new notions were explored, giving the participants an opportunity to critically self-reflect on their typical mental scripts.
Thus, the four ethics labs implanted seeds of thought in our participating biomedical clinicians and scientists, biostatisticians, policy-makers and lawyers. In this way, these seeds can become part of a moral deliberation practice after the lab. Moreover, the moral ecosystem became part and parcel of our own ongoing social science study on the ethical ramifications of implementing precision medicine in Denmark. Both the ethics labs and the interviews revealed that the lab could function as a free space for social scientists to discuss and experiment with insights in conversation with healthcare professionals. Several of the MeInWe researchers reported how this conversation continued in discussions with their informants outside the lab. In some way, the interviews revealed this need to continue the moral discourse. While the dominant strength of the labs, according to the participants, was the moral awareness they fostered, the prevailing limitation they cited was the seemingly abrupt ending without a summation of what was discussed or proposing an aftermath. Leaving the ethics lab after 3 h of deliberation, the participants were curious about how group members processed the conversation and how they intended to use it in their work place. Some were curious about the other labs’ discoveries. Several of the interviewees expressed that they would have liked a follow-up session and suggested a second meeting be incorporated into the design to be held a couple of months later with the same people.
However, not only did participants express a wish for a follow-up session with their group. Some also proposed the idea to have an Ethics Laboratory set up in their workplace, either by having one of our team members return to their ethnographic site or be visited by a facilitator that could guide them through the moral deliberation. Several stressed the need for a structured format. One feared that the conversation would otherwise end in digressions, opinionated outbursts and “chitchat” that would derail the moral deliberation. Many reported that arranged moral conversations rarely occurred in their workplace. Some suggested other uses of the ethics lab idea by including the Ethics Laboratory in the design of an interdisciplinary research project as a way for the project partners to learn from their ethical observations as a project progresses.
Beyond precision medicine
Precision medicine involves ever more translational movements between basic science and the clinic. It covers movements between basic scientific discovery, disease modelling, drug development, clinical indexes and patient care (Seyhan and Carini 2019). Similar to these translational phases in precision medicine where scientists and physicians interact to translate basic biomedical discoveries into routine medical practice, our vision for the Ethics Laboratory was to design a dialogical platform and create “a communicative climate” (Abma et al. 2009, p. 218) that could bring a varied group of professionals into conversation on joint moral concerns, and in this way promote a moral ecosystem of interconnected professional fields. Such a moral ecosystem may reach far beyond the field of precision medicine. Reflection is an integral process of learning that can provide guidance in professional contexts (e.g. Moon 1999; Schön 1984). In this light, the Ethics Laboratory can be viewed as a vehicle for moral development and ethics education as it invites participants to critically engage with complex moral issues whether it be addressing the challenges of precision medicine, globalization processes, climate change or human migration.
Much has been written on the bioethics curriculum of medical and nursing students (Martins et al. 2021; Ngan and Sim 2021; Gordijn and ten Have 2018). The training is intended to prepare the students for the moral dilemmas in a clinical setting. Seeing that some studies show how medical students’ moral receptivity stagnate during their medical education (Serodio et al. 2016; Hegazi and Wilson 2013) and, additionally, in view of the fact that moral issues permeate medicine, science and society, it is worthwhile contemplating fora post formal training where experienced professionals can come into conversation and explore the morality of, for example, a technology or an intervention. The Ethics Laboratory does not teach ethics in the traditional manner within an educational system nor does it take place within a framework with identified learning objectives that encompass familiarity with moral theories, acquiring knowledge of bioethics or adopting a series of ethical competencies (e.g. Core Competencies Task Force 2011; Larcher et al. 2010). However, the didactic value of the lab is found in the intersubjective, guided deliberation, in strict confidentiality, on a broad range of ethical questions across professions. As such, it lends itself as a model to be incorporated in teaching programs, research projects and public information settings.
Research projects, either national or international, consist of a Consortium of collaborators when they reach a certain size. Building on the suggestion of several of the interviewees, the Ethics Laboratory can promote interactivity in the beginning, midway and end of a research project, and thereby enable internal sharing of moral topics involved in the respective work packages. By engaging in these topics throughout the project, greater synchronization can be framed and sustained. In this way, the ethics lab model can help improve mutual understanding and close interdisciplinary partnerships as well as predicting and preventing unwanted pitfalls, paths and outcome. Bringing the Ethics Laboratory to the public square, like engaging in public debates in the Ancient market place of Athens, could address many current societal and global issues. For example, educating publics on the ethical questions and ramifications of a new policy that will limit citizen autonomy (e.g. regulations to promote environmental sustainability that will impact people’s lifestyles). Transparency is a foundational principle that has long been heralded by democracies (Fung 2013). Moral deliberation in an ethics lab pledges alliance to this principle and, as such, can be said to correspond to public hearings or newspaper debates.
Although the model structure is novel, the Ethics Laboratory is not entirely an unorthodox idea. It aligns with a growing trend that advocates for a specifically participatory approach to moral learning. For decades, the American physican, Edmund Pellegrino, a harbinger of a virtuous approach to medical ethics, has stressed the development of dispositions and values, such as compassion, courage and prudence, in medical training (Pellegrino 2001). His advocacy underscores how moral learning reaches far beyond cognitive capabilities to encompass actual character building and emotional awareness of the health care provider when faced with humanly challenging situations. Another prominent medical ethicist Jan Helge Solbakk, who is also a physician, substantiates Pellegrino’s position by demonstrating how tragic stories of illness in an educational environment serve as prominent teachers of ethical wisdom (Solbakk 2015). Without reducing moral learning to theoretical positions, he emphasizes “the only true doctor of morality: dialogue” (Solbakk 2015, p. 208). Understanding ethics as a dialogical practice is supported by the Dutch approach to moral deliberation (Metselaar et al. 2015; Molewijk et al. 2008a, b) taking experiences, conflicts and emotions “as starting points for an inquiry into the underlying moral positions of the stakeholders” (Metselaar et al. 2015, p. 51). These scholars join forces in explaining the limits of a strictly theoretical stance to moral learning. According to this perspective, ethical theories provide theoretically consistent and coherent arguments without offering much guidance in the moral conundrums and often messy reality of physician and patient life.
Unlike the view of the subject acquiring moral knowledge through theories and competencies, as if filling up an empty container, we came to understand moral learning differently. More than relying on a transmission of information through pre-established rational theories to guide people’s moral conduct, the Ethics Laboratory builds on exploring real-life experiences with a morally ambiguous content (Knox 2021). Moral learning occurs when work experiences are activated and reflected on in tandem without focusing on outcomes. Thus perceived, the Ethics Laboratory becomes an experiment that scrutinizes ethical commitments and decisions while, in chorus, contemplating moral possibilities and limits. Literacy in education refers to the acquisition of basic skills, for example the ability to read and write. Without literacy skills, reading a book, a newspaper or a road sign will be impossible, making many goods inaccessible, for example a scholarly education. Equally, moral literacy depends on specific qualities that are necessary for expanding awareness on ethical issues within a professional context or field.
The ethics lab’s communitarian nature calls for an integrative approach to ethical topics that are important both for healthcare and society at large. Moral literacy involves recognizing moral ambiguities and using imagination as well as reflective skills to identify conflicts and concerns, virtues and values underlying a situation in addition to considering consequences of actions and the intention of actors. Discussing what is valuable and at stake in a given professional or societal context can enhance moral literacy in areas that run across disciplines, sectors and institutions, across interests, customs and preferences. To mention one example, moral distress is an increasing concern in health care practice (Houston et al. 2013; Allen et al. 2013). If not addressed, moral distress can eventually cause health professionals to leave their jobs and even their profession (Austin 2016). As a result of arduous ethical issues in patient care (Kälvemark et al. 2004) and medical research, the Ethics Laboratory model can serve as one safeguard against the experience of distress by making lived predicaments visible and shared through dialogue.
The presence of reasoning (explaining moral perspectives to each other), sensitivity (exposing oneself to the embedded ethical challenges in one’s work) and imagination (envisioning other perspectives than one’s own) shaped the moral awareness that transpired in our ethics labs. Considering our findings, the Ethics Laboratory represents a collaborative learning activity in public health, medical science and practice. With that in mind, it can support professionals’ navigation through complex situations and, thereby, sustain the moral ecosystem.
Notes
Where Europe generally use the term ‘personalized medicine,’ the US tends to use the term ‘precision medicine’. Though not entirely identical, we use them interchangeably in this article.
“Personalized Medicine in the Welfare State” (MeInWe) is made possible by the Carlsberg Foundation’s Semper Arden grant in 2017 awarded to Professor Mette N. Svendsen from the University of Copenhagen. See www.meinwe.ku.dk.
The Ministry of Health and Danish Regions initiated in December 2016 the health strategy “Personalized Medicine – to the benefit of the patient”.
References
Abma, T.A., B. Molewijk, and G.A.M. Widdershoven. 2009. Good care in ongoing dialogue. Improving the quality of care through moral deliberation and responsive evaluation. Health Care Analysis 17: 217–235.
Allen, R., et al. 2013. Moral distress among healthcare professionals at a health system. Healthcare Law, Ethics, and Regulation 15 (3): 111–118.
Austin, W. 2016. Contemporary healthcare practice and the risk of moral distress. Healthcare Management Forum 29 (3): 131–133.
Beauchamp, T.L., and J.F. Childress. 2009. Principles of biomedical ethics, 7th ed. Oxford: Oxford University Press.
Brandt, A.M., and P. Rozin, eds. 1997. Morality and health. New York: Routledge.
Chen, R., and M. Snyder. 2013. Promise of personalized omics to precision medicine. Wiley Interdisciplinary Reviews: Systems Biology and Medicine 5 (1): 73–82.
Core Competencies Task Force. 2011. Core competencies for healthcare ethics consultation, 2nd ed. Chicago: American Society of Bioethics and Humanities.
De Marchiano, Maria, et al. 2021. Translational research in the era of personalized medicine: Where we are and where wil will go. Journal of Personalized Medicine 11: 216.
Dickenson, D. 2013. Me medicine vs. we medicine: Reclaiming technology for the common good. New York: Columbia University Press.
Förde, R., and R. Pedersen. 2011. Clinical ethics committees in Norway: What do they do and does it make a difference? Special section – Bioethics beyond borders. Cambridge Quarterly Health Care Ethics 20: 389–395.
Fowers, B. J. 2020. Social science as an inherently moral endeavor. Journal of Moral Education 1–12. https://doi.org/10.1080/03057240.2020.1781069.
Fung, A. 2013. Infotopia: Unleashing the democratic power of transparency. Politics and Society 42 (2): 183–212.
Gadamer, H.-G. 2004. Truth and method. London: Continuum.
Gordijn, B., and H. ten Have. 2018. The trilemma of designing international bioethics curricula. Medicine, Health Care and Philosophy 21: 1–2.
Hegazi, I., and I. Wilson. 2013. Medical education and moral segmentation in medical students. Medical Education 47 (10): 1022–1028.
Houston, S., et al. 2013. The intensity and frequency of moral distress among different healthcare disciplines. The Journal of Clinical Ethics 24 (2): 98–112.
Johnson, M. 1993. Moral imagination: Implications of cognitive science for ethics. Chicago: The University of Chicago Press.
Kälvemark, et al. 2004. Living with conflicts-ethical dilemmas and moral distress in the health care system. Social Science and Medicine 58 (6): 1075–1084.
Kerr, A., C.K. Chekar, E. Ross, J. Swallow, and S. Cunningham-Burley, eds. 2021. Personalised cancer medicine: Future crafting in the genomic era. Manchester: Manchester University Press.
Knox, J.B.L. 2021. The ethics laboratory: A dialogical practice for moral deliberations in professional cross-fields. HEC Forum. https://doi.org/10.1007/s10730-021-09460-w online September 24th.
Kraaijeveld, M.I., J.B.A.M. Schilderman, and E. van Leeuwen. 2020. Moral sensitivity revisited. Nursing Ethics 28 (2): 179–189.
Larcher, V. et al. (2010). Core competencies for clinical ethics committees. Medical Ethics 10 (1): 30–33.
Lau, E., and J. Wu. 2018. Omics, big data, and precision medicine in cardiovascular sciences. Circulation Research 122 (9): 1165–1168.
Martins, V.S.M., C.M.N.C. Santos, P.U.R. Bataglia, et al. 2021. The teaching of ethics and the moral competence of medical and nursing students. Health Care Analysis 29: 113–126.
Metselaar, S., et al. 2015. Beyond recommendation and mediation: Moral case deliberation as moral learning in dialogue. The American Journal of Bioethics 15 (1): 50–51.
Molewijk, A.C., T. Abma, M. Stolper, and G. Widdershoven. 2008. Teaching ethics in the clinic. The theory and practice of moral case deliberation. Journal of Medical Ethics 34 (2): 120–124.
Molewijk, B., E. van Zadelhoff, B. Lendemeijer, and G. Widdershoven. 2008. Implementing moral case deliberation in Dutch health care; improving moral competency of professionals and the quality of care. Bioethica Forum 1 (1): 57–65.
Moon, J.A. 1999. Reflection in learning and professional development: Theory and practice. London and New York: Routledge.
Ngan, O.M.Y., and J.H. Sim. 2021. Evolution of bioethics education in the medical programme: A tale of two medical schools. International Journal of Ethics Education 6: 37–50.
Pellegrino, E. 2001. Physician and philosopher. The philosophical foundation of medicine: Essays by Dr. Edmund Pellegrino. Charlottesville: Carden Jennings Publishing.
Pickworth, E. 2000. Should local research ethics committees monitor research they have approved? Journal of Medical Ethics 26: 330–333.
Plato. 1992. Theatetus. Indianapolis/Cambridge: Hackett Publishing Company.
Prainsack, B. 2017. Personalized medicine: Empowered patients in the 21st century? New York, NY: New York University Press.
Prainsack, B. 2018. The ‘we’ in the ‘me’: Solidarity and health care in the era of personalized medicine. Science, Technology, and Human Values 43 (1): 21–44.
Rasoal, Dara, K. Skovdahl, M. Gifford, and A. Kihlgren. 2017. Clinical ethics support for healthcare personnel: An integrative literature review. HEC Forum 29: 313–346.
Reardon, J. 2017. The postgenomic condition. Ethics, justice and knowledge after the genome. Chicago: Chicago University Press.
Schön, D. A. 1984. The reflective practitioner: How professionals think in action. Basic Books.
Serodio, A., B.I. Kopelman, and P.U.R. Bataglia. 2016. The promotion of medical students’ moral development: A comparison between a traditional course on bioethics and a course complemented with the Konstanz method of dilemma discussion. International Journal of Ethics Education 1: 89–89.
Seyhan, A.A., and C. Carini. 2019. Are innovation and new technologies in precision medicine paving a new era in patients centric care? Journal of Translational Medicine 17: 114.
Slowther, A.M., L. McClimans, and C. Price. 2012. Development of clinical ethics services in the UK: A national survey. Journal of Medical Ethics 38: 210–214.
Solbakk, J.H. 2015. Movements and movies in bioethics: The use of theatre and cinema in teaching bioethics. In bioethics education in a global perspective, ed. Henk ten Have, 203–221. Dordrecht: Springer.
Thomson, C. 2012. Research ethics committees. In Encyclopedia of applied ethics, vol. 3, ed. Ruth Chadwick, 786–796. San Diego: Academic Press.
Van Beers, B., S. Sterckx, and D. Dickenson, eds. 2018. Personalised medicine, individual choice and the common good. Cambridge: Cambridge University Press.
Vollmann, J., V. Sandow, S. Wäscher, and J. Schildmann, eds. 2015. The ethics of personalised medicine: Critical perspectives. Surrey/UK: Ashgate.
Acknowledgements
This work was supported by a Semper Ardens Grant from the Carlsberg Foundation [grant number CF17-0016 (PI Mette N. Svendsen)].
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None to declare.
Ethical approval
Participants gave their informed consent to participate in the ethics laboratory and were informed of future publications. According to Danish law this study did not need ethical approval from the research ethics review board as no biological sample were taken.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Knox, J.B.L., Svendsen, M.N. The ethics laboratory: an educational tool for moral learning. International Journal of Ethics Education 7, 257–270 (2022). https://doi.org/10.1007/s40889-022-00142-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40889-022-00142-w