
Abstract
Background
There is a significant number of neuropsychological measures for use among children aged 6–12 years. However, most of these tests have been developed in high-income contexts (HICs). To avoid or to at least to minimize bias in assessment, most researchers carry out cultural adaptations of these tools. In selecting sub-tests to adapt before using the entire test battery, researchers would benefit from having a reference source summarizing available tools and how easily they can be used in different context. This is where the paper makes a contribution. This narrative review has a twofold aim: first, to identify tools commonly used among 6–12-year-olds; second, to summarize the psychometric properties of these tools especially emphasizing their usage across different cultural contexts.
Methods
We searched the literature from 1 January 1987 to 31 December 2017 for tools used among children aged 6 to 12 years. An extensive search of PubMed, Psych Info and Web of Science using the keywords (i) neuropsychological or neurocognitive with (ii) assessment or test was done.
Results
A hundred and forty-five papers out of 306 reported on psychometric properties of different tools including Behavior Rating Inventory of Executive Functioning—BRIEF (count = 6), Visual-Motor Integration—VMI (count = 6), the Test of Memory Malingering—TOMM (count = 6), MSVT (count = 6) and Continuous Performance Tests—CPT (count = 6). Forty-six percent of the papers reported studies conducted in the USA. Most of these studies were based in high-income countries, which further highlights the need to validate these measures for use in lower- and middle-income countries. Psychometric check was adequate in most tests for measuring executive functioning such as BRIEF, although tests such as CPT that measure complex attention had mixed findings. Moreover, we found that these studies addressed certain aspects of validity and or reliability while leaving out others; thus, a comprehensive picture is lacking.
Conclusion
We propose further studies to thoroughly investigate and report the psychometric properties of these measures, especially in lower- and middle-income countries.
Similar content being viewed by others


Introduction
The ages 6–12 are known as the ‘ages of reason’ by the likes of Piaget’s cognitive theorists. Children ages 6–7 years are likely to start developing reasoning abilities related to the concrete operational level of cognitive development where they can form complex representations and be able to solve complex problems. For example, a child at this age can understand that a parent can be a disciplinarian and at the same time be a provider while a teacher can also be a parent at their own home hence be a disciplinarian and provider to his/her own children. As these cognitive abilities develop, formal operations level of cognitive development quips in starting at ages 10–12 years. This is where the children can form generalizations across different instances and also have hypothetical reasoning ability. They can combine several shapes to form an overall pattern.
Performance on these cognitive abilities is founded on the physiological growth of the brain in terms of neurons whose plasticity or formation is a function of environmental factors/triggers. Performance is measured adequately by valid and reliable neuropsychological tools and the psychometric adequacy inquiry forms the objectives of this narrative review. This is particularly for children aged 6–12 years whose literature on psychometric properties of cognitive tools is marred by mixed findings (Llorente et al. 2009; Spironello et al. 2010). The mixed findings embedded in different literatures make it hard to find one tool for a certain cognitive function whose validity and reliability indicators are good for forming a hypothesis on the functionality of a child (Hubley and Zumbo 1996). Children aged 6–12 years are just starting school, and their ability to learn is embedded on cognitive functions such as those related to memory formation, problem solving, flexibility and judgement (Chen at al. 2009; Stad et al. 2019). Functions such as cognitive flexibility among these children have been found to be related to school performance (Stad et al. 2019). Culture-sensitive tools can be used to identify learning problems as well as inform an instruction plan that improves performance or a treatment plan that rehabilitates cognitive deficits. Tools for children aged 6–12 years are diverse and with mixed findings on their validity and reliability indicators (Ahonniska et al. 2000; Holding et al. 2004; Llorente et al. 2009; Spironello et al. 2010). Cultural diversity calls for development of tools that are sensitive and specific to the cultural constructs hence the diversity in tools formed and reported psychometric properties. This narrative review aims to summarize findings on psychometric properties of cognitive tools used among children aged 6–12 years.
Neuropsychological Tools
Neuropsychological tools are measures used to assess the brain-behaviour relationship (Casaletto and Heaton 2017). Executive function, memory, visuomotor coordination, processing speed, language and attention are basic cognitive domains measured using these tools (Fasfous et al. 2015). Intrusive tests such as spinal tap were used before the advent of neuropsychological tools which have over the years evolved from paper-based tools to computerized ones. Neuropsychological tools have not only made it less intrusive to assess cognitive functions, they have over the years become more comprehensive and easier to administer with some of the tools needing no training to administer and score. This has made it possible to diagnose neurocognitive disorders as well as monitor dysfunction progression and recovery thereby better informing interventions.
Good neuropsychological tools have to be standardized, reliable and valid. When a test measures what it is purported to measure, then the test is said to be valid and it is reliable when it accurately measures what it is supposed to measure (Hubley and Zumbo 1996; Kelley 1927). A test is said to have sensitivity when it is able to identify those with disease and have specificity when it is able to identify those without disease (Parikh et al. 2008). Testing of validity and reliability of a test is construed in different forms. Construct validity is assumed whenever there is good correlation between constructs and responses from the measures (Teglasi et al. 2012). A tool is said to have construct validity whenever it is able to show response variations in relation to real life and the measured phenomenon. Discriminant and convergent validity are used to establish construct validity. Discriminant validity is established when two tools that are supposed to measure different phenomena demonstrate this difference. Convergent validity is established whenever two tests that are supposed to measure the same phenomenon show this similarity. Factor analysis also establishes construct validity by showing whether a cluster of items that are supposed to be caused by the target constructs. As a note, in this review, when the form of construct validity is not specified as none of the three discussed above, it will be identified as just construct validity.
Studies that have previously reviewed neurocognitive tests have either reviewed tests relevant to specific diseases or other age groups with partial relevance to early schoolers (Bradley-Johnson 2001; Ezeamama et al. 2018; Stadskleiv 2020; Williams et al. 2014). The test specific reviews have published findings on psychometric properties and cultural relevance of different neurocognitive tests(Bradley-Johnson 2001). The current study furthers these findings and gives prominence to the early schoolers.
Study Objective
This narrative review looks at neurocognitive tools developed and standardized from 1987 to 2017 specifically for children ages 6–12 years. A narrative review is recommended for a critical discussion of knowledge on a topic of interest with the aim of collating and summarizing study findings on the topic as well as identifying research gaps (Ferrari 2015). The aims of this review are to identify and summarize commonly used neuropsychological tools among 6–12 years globally and their psychometric properties across different contexts. Specifically, the review aims at answering the following research questions:
-
1.
Which standardized neurocognitive tools are commonly used among 6–12-year-olds?
-
2.
Which cultural adaptations have been made to these tools?
-
3.
What is the reliability, validity, sensitivity, and specificity of these tools?
Methods
We identified studies conducted between 1987 and 2017 through a thorough search of PubMed, Psych Info, and Web of Science using the keywords (i) neuropsychological or neurocognitive with (ii) assessment or test.
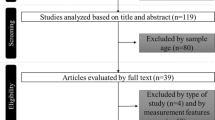
Following this search, we included original studies that examined any form of psychometric properties using neuropsychological tests among children aged 6–12 years globally. RM examined each study against the exclusion and inclusion criteria and determined whether it should be included in the review. Inclusion criteria: written in English language, use of Neuropsychological measures, children 6–12 years, all peer-reviewed published journal articles, publications between 1997 and 2017 and human subjects’ research. Studies that partially covered the age criteria were also included in the review. Exclusion criteria: not in English language, neurophysiological measure, grey literature, full text missing and animals. Information concerning the type of neuropsychological assessment, cognitive domain measured (executive functions, perceptual motor, complex attention, language, learning and memory), study setting and type of standardization conducted was extracted. She developed a template of key findings on a spreadsheet and shared with other mentors. She received feedback from FV, AA, MPG and KM. There were 12 papers that lacked clarity in their psychometric findings where all the other authors reviewed these papers one by one. Out of these papers, three were selected on the basis that they did have results showing the tools’ validity. Figure 1 shows the data extraction flow chart. Information from the papers was coded in terms of authors, country where the study was done, population of interest, tool examined and domains it covers, as well as the reliability and validity outcomes. This information was entered into an online Excel sheet that was accessible by all the authors. Cognitive domains and sub-domains were classified according to the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5) (Sachdev et al. 2014) as shown in Fig. 2.

Data extraction flow chart

Classification of cognitive domains and sub-domains
Results
The narrative review identified 306 papers, in which 145 papers met the inclusion criteria as indicated in Fig. 1. Figure 1 provides a data extraction flow chart (also see Appendix 1 in Supplementary Information). Most of the papers used multiple tools, with the total frequency of different tools used amounting to 142. Twenty-three of the tools had a total frequency of ≥2. The majority of the studies were conducted in the clinical population (N = 102). The cognitive domain distribution of studies included 77 on executive function tests, 75 on complex attention tests, 49 on perceptual motor and motor tests, 21 on learning tests, 28 on language tests and 62 on memory tests, as well as 14 on tests distributed across arithmetic, social cognition, cognitive reserve, intelligence, representational competence and academic achievement domains. The validity and reliability terms as well as the statistical and adaptation criteria described are those referenced by the original study authors. Almost half of the studies were conducted in the USA as shown in Table 1.
Adaptation Processes in the Reviewed Studies
There were eleven papers that reported on formation of completely new tools compared to a hundred and thirty-four that adapted and/or tested the psychometric properties of already-existing tools.
Assembly
There are eleven studies that chose to develop new tools. (van Nieuwenhuijzen et al. 2011) developed a social information processing measure because there wasn’t a tool that measured this cognitive domain. This measure involved using vignettes in combination with cartoons, picture and video which depicted different social situations, and the child was required to respond to different questions like what was happening and how they would respond in a similar situation. Scores were developed that evaluated the responses information processing trajectory within a linear scale. Shorter versions of tools were also created for screening purposes.
Adoption
Adoption involved translation and making iterations to the items. Tools whose adaptation included translation had to be keen in ensuring the new versions did not lose the characteristics of the original tool. This is because the respondent’s language background tends to exert some effect on the tools. It is for this reason that most cultural adaptations took language into account (Rohitrattana et al. 2014; Siqueira et al. 2016). Some of the tools did not rely heavily on language; hence, the new versions had to translate the instructions only (Bangirana et al. 2015). Bilingual translators were preferred in five studies and a back-translation design adapted for the translation (Bangirana et al. 2015; Fasfous et al. 2015; Hwang et al. 2006; Siqueira et al. 2016). Where two translators would not agree on instruction or stimuli translation, a third one would be integrated as a tie breaker.
Translation was only done after permission was sought from the original authors. This, at times, faced challenges where authors were not willing to give permission for development of a different version, or in situations where they did, permission was partial in that the developers gave access to for example the tool’s stimuli (Siqueira et al. 2016).
Once translation was done, substitution was pursued for certain items that were unfamiliar to the respondents with items that were familiar (Kitsao-Wekulo et al. 2013b). In adapting a neurobehavioural test battery among Thai children, the authors substituted envelopes with paper as well as hair brush with hair clip (Rohitrattana et al. 2014). The later substitution was interestingly because of similar pronunciations to a toothbrush. An adaptation of the Child Hayling Test (CHT) among Brazilian children included the exclusive use of nouns instead of a mixture of nouns, adverbs and adjectives that were used in the adult version of the test (Siqueira et al. 2016). This was done to meet the linguistic preference of the Brazilian children population. These forms of changes are integrated in the stimuli and instructions. Usually, mental health practitioners, such as psychologists at postgraduate level, judged whether each item is representative of the cognitive domains for which the tool is supposed to measure, and whether they would be easily comprehended.
Practice effects were determined in one study by doing a paired T-test analysis (Kitsao-Wekulo et al. 2013a), while in another, percentage change and reliability change indexes were calculated (Llorente et al. 2009). Reliability change indexes take into account performance that is likely to be because of measurement unreliability. To reduce practice effects in test–retest reliability measurements, adaptation also involved creating alternative forms of the same tests. Creating alternate forms may not always be the best practice as a study among Thai children showed low test–retest reliability in tests with alternate forms (Rohitrattana et al. 2014). Comparability of alternate forms may need to be improved to reduce such effects. Sub-measures, as opposed to a full neuropsychological battery, have been targets for adaptation based on the objectives of the study (Reitan and Wolfson 2004; Thomas et al. 2016). Sadeh, Burns and Sullivan (2012) investigated the predictive power of the EF screener within Behavior Assessment System for Children-Teacher Report (BASC). An EF screener with strong predictive power would be useful in screening for behavioural problems early enough for preventive and intervention purposes.
Pilot
Ten pilot studies evaluated the linguistic, semantic and syntax complexities of the tools. P. K. Kitsao-Wekulo et al. (2013a) did a pilot study for the Kilifi Toolkit to check translation comprehension, familiarity of the items and ceiling and floor effects of the modifications, as well as ease of administration and scoring. Pilot studies exuded vital information such as the impact of examples in helping children understand the guidelines (Hwang et al. 2006).
Standardization
Validity and reliability estimates were evaluated for the tests in one hundred and forty-one papers depending on the objectives of the study in relation to the tool. Four papers sought to extract age-related test norms. Test–retest reliability was assessed using intraclass correlation (ICC) while internal consistency (extent to which items hang together) was evaluated using Cronbach alpha. Confirmatory factor analysis has been used in the studies to assess the tests’ construct validity or assess how well the factor structure fits the test items. A good fit is one with a non-significant p value, a root mean square error of approximation (RMSEA) of less than .01 and a comparative fit index (CFI) of more than .90 (Rose et al 2011). Construct validity has also been assessed by identifying group difference between diseased and healthy samples based on their cognitive outcomes in the tests (Spironello et al. 2010). Discriminant (a tool’s ability to differentiate those with cognitive impairment from those without) and convergent validity (two tools’ ability to identify those with cognitive impairment) is part of construct validity. Another way used to look at the internal structure of a test is through factor analysis with eigenvalues among other calculations being done to evaluate the number of factors (Stinnett et al 2002). Concurrent validity, where the level of agreement between two tools is evaluated, was measured using Pearson’s correlation coefficient (Spironello et al. 2010). Receiver operating characteristics (ROC) have been used to assess the sensitivity and specificity of tests i.e. the tests’ scoring ability in differentiating those with cognitive impairment from those without (Thaler et al. 2010). Area under the curves (AUCs) have also been used with ROC to assess for group differences. An AUC of .80 and above indicates good classification which is synonymous with support for predictive discrimination. Sensitivity has also been assessed using univariate analyses of variance (ANOVAs). ANOVA has also been used in studies creating norms for tests where the effects of age and gender are evaluated (Reynolds et al. 2016). Multiple regression analysis (MANOVA) gives a clearer picture of associations by removing confounding effects and measurement errors among other factors that influence outcomes. (Konstantopoulos et al 2015). chose to use MANOVA when creating normative data for CCTT where the relationship between completion time and age and gender was investigated. Structural equations do the same as they have been used to give an overall accurate estimation of associations (Budtz-Jorgensen et al. 2002). Higher sensitivity and specificity are predictive of the best cut-off points/scores when assessing for impairment in children. Test of Memory and Learning (TOMAL) evaluation indicated that a cut-off point of .80 indicated the best sensitivity and specificity combination (sensitivity .70, specificity .62) (Thaler et al. 2010). Criterion validity has been used to evaluate further the internal structure of a tool by elucidating the test’s ability to denote the severity of the cognitive impairment (Woodward and Donders 1998).
The population chosen to test the tools’ psychometric properties is based on the objectives of the study and the population most likely to exhibit cognitive impairment. Thirty-seven papers chose an entirely healthy population to study, while thirty-six chose a population with a healthy control and seventy-two chose an entirely diseased population depending on the cognitive deficit of interest to the study. Thirty-seven papers had populations with attention deficit hyperactive disorder representing the most (26%) preferred population in the studies.
There are studies which chose to adapt the test among males only (n = 2) and another on female only (n = 1) instead of both genders (Carone 2014; Termine et al. 2016). As much as gender is highlighted as a confounder in research, in neurocognitive adaptation studies, gender effect on cognitive measurements has been found to be insignificant. (Roy et al. 2015). found that gender was insignificant in executive function measurements.
Cognitive Domains Psychometric Checks
The psychometric results of different measures are outlined, and they are organized into the neurocognitive domains the tools measure. The description of the results as either poor/weak, moderate and good/high is according to the original study authors’ classification of findings. In the main text, a summary is provided, and detailed information on the countries where the studies were conducted as well as the specific psychometric outcomes with actual numbers (including the presence and absence of specific psychometric checks and the reported statistics) are in Appendix 1 of the supplementary materials.
Executive Function Tests Standardization Outcomes
The Behaviour Rating Inventory of Executive Functioning (BRIEF) had the highest number of standardization studies (N = 7). It passed validation indicators though reliability studies were yet to be done. The WISC III and IV reported good validity though reliability indicators varied with regard to subsets under study. The Digit Span subtest of the WISC III had low test–retest reliability (Table 2).
Memory Tests Standardization Outcomes
The Medical Symptom Validity Test (MSVT) was the most heavily researched on (N = 6) closely followed by the Test of Memory Malingering (TOMM and TOMM 2) and Word Memory Test (WMT) each having five studies looking at their psychometric properties. TOMM had varying studies indicating different findings with regard to validity, specificity and sensitivity. The other two tests showed high validity (Table 3).
Complex Attention Standardization Outcomes
The Continuous Performance Test (CPT) and its revisions had the highest number of studies (N = 6) looking into its psychometric properties. Different studies found differing standardization outcomes as indicated in Table 3. CANTAB came in second and its general validity was established though its subtests, spatial working memory (SWM), had low construct validity. CANTAB’s test–retest reliability was also found to be low (Tables 4).
Motor and Perceptual Motor Standardization Outcomes
Six studies looked at the Developmental Test of Visuo-Motor Integration psychometric indicators. The studies had differing findings when it came to discriminant validity and test–retest reliability. General validity was established, but two studies could not agree on the discriminant validity of the tool as one reported the validity to be poor (Table 5).
Learning Standardization Outcomes
Cogstate Battery, WISC IV, Differential Ability Scales (DAS) and NEPSY were the most frequently studied tests (count ≥2). Cogstate validity was not questionable, but two studies found its test–retest reliability to range from weak/low to strong. NEPSY had similar reliability outcomes (Table 6).
Language Standardization Outcomes
The language tests had equal variance on frequency of studies done. The WSC IV vocabulary test was found to have no validity, and the Seashore Rhythm Test had low internal consistency. Most of the language tools had no validity indicators (Table 7).
Other Tests’ Standardization Outcomes
There was no validity for the cognitive reserve subtest within WIAT-II. Tests used for social cognition were found to be valid including interesting tools such as cartoons, pictures and video vignettes (Table 8).
Tools Tested in LMIC Including Sub-Saharan Africa (SSA)
Six studies from SSA four in Kenya and two in Uganda were included. In Uganda, the authors tested construct, concurrent and convergent validity, as well as test–retest reliability for the computerized, self-administered CogState battery and construct validity for the KABC-II (Bangirana et al. 2009; Bangirana et al. 2015). Moderate test–retest coefficient correlations were found while concurrent and convergent validity correlations were found with tools such as KABC-II and TOVA. In Kenya, on the other hand, internal consistency was tested for Tower Test (planning), Self-Ordered Pointing Test (SOPT; verbal/visual selective reminding), Verbal List Learning (VLL; working memory), Colored Progressive Matrices (CPM; reasoning), Dots (nonverbal memory), Contingency Naming Test (CNT; attention and attention shift, Score (auditory sustained and selective attention), as well as People Search (visual sustained and selective attention) (Kitsao-Wekulo et al. 2013a). Test–retest reliability for immediate memory span and CNT was found to be below acceptable levels while the other subtests had marginally to acceptable reliability. Internal consistent results ranged from .70 to .84. The sensitivity, specificity and test–retest reliability of the Ten Questions Questionnaire, which measures perceptual motor and memory domains, was also tested among 6–9-year-old Kenyan children (Mung’ala-Odera et al 2004). Test–retest reliability was found to be excellent for motor, vision, speech and four cognition questions while specificity and sensitivity rates were greater than 70% and 96% respectively.
Discussion
This narrative review covered studies on adaption and standardization of neurocognitive tools that were done in between 1987 and 2017 among children aged 6–12 years old. The narrative review investigated the standardized tools that are commonly used and the cultural adaptations made to these tools, as well as the reliability, validity, sensitivity and specificity of these tools.
Commonly Used Tools and Psychometric Outcomes
The cognitive domains covered were exhaustive of the DSM-5 classification though tools that covered executive functions, complex attention and memory domains were the most researched on tools. The child neuropsychological test findings reviewed in this paper reported on mostly executive functioning standardization outcomes where BRIEF was the most researched on tool (N = 6) followed by KABC-II (N = 3). Validity indicators for the BRIEF showed partial-to-low correlation outcomes with only discriminant validity being wholly significant when it came to its three composite scores or scale scores, as well as comparison of its teacher-rated to parent-rated versions. BRIEF may have been a common tool due to the ease of administration through the parents (Vriezen and Pigott 2002). KABC-II construct validity was supported in all the studies though its predictive validity and reliability findings were rated as low to moderate. KABC-II was among the few executive function tools to be standardized in LMIC despite its complexity in administration (Bangirana et al. 2009).
Complex attention standardization outcomes were mainly reported for the CPT (N = 6) and Attention Network Test (ANT) (N = 5). The later had low reliability outcomes with only one study reporting moderate to high test–retest reliability findings. The validity outcomes were, however, high proving that the tool has good internal validity. CPT was also popularly studied, and this could have led to the very many developed versions of it which continue to be updated. Moreover, it has good discriminant validity indicators with moderate test–retest reliability. However, the specificity and sensitivity indicators range from moderate to high and the general validity was found to be partially significant.
Medical Symptom Validity Test (MSVT) (N = 6), The Test of Memory Malingering (TOMM) (N = 6) and Word Memory Test (WMT) (N-4) were commonly studied under the memory domain. WMT showed mixed results when it came to validity outcomes, but specificity was endorsed as high in two studies. This trend was not seen in MSVT which showed good validity and specificity outcomes while TOMM had mixed findings where validity was indicated as partially significant in some studies, specificity high and sensitivity as low. In some cases, insufficient effort could have affected the variability in validity and sensitivity outcomes.
Visuo-Motor Integration was the only perceptual motor prevalently studied test (N = 6) with mixed discriminant, validity findings but good convergent, construct, concurrent and criterion validity. Test–retest reliability ranged from low to high in varied studies while inter-rater reliability was ranked as high in one study. The popularity of this tool could be attributed to ease of administration (Ahonniska et al. 2001) especially due to the age of our population of interest or it could also be due to being among the very few tests that are available for the perceptual motor domain.
Neuropsychological batteries, tests that have several subtests within them, may not have been attributed as common as they were broken down into their respective subtests cognisant to the cognitive domain covered. They were, however, also widely studied. The tests include the Wechsler Intelligence Scale for Children (WISC), Halstead-Reitan Neuropsychological Test Battery for Children (HRNB-C) and Cambridge Neuropsychological Test Automated Battery (CANTAB). HRNB-C was found to have good discriminant and construct validity while reliability and sensitivity were found to be high. CANTAB as well was found to have good construct validity though internal consistency ranged from poor to high in between the subtests (Syvaoja et al. 2015). WISC III and IV subsets were commonly studied with reliability findings ranging from poor to high depending on the subtest while validity outcomes showed the same partial trend.
CogState battery along with other few tests have been validated in Africa (Bangirana et al. 2015; Holding et al. 2004; Mung’ala-Odera et al. 2004). In as much as only six studies have been conducted across Kenya and Uganda, the number of tests covered is nearly exhaustive of the cognitive domains identified as vital in DSM-5. Executive functions covered include planning, working memory and reasoning; complex attention subdomains covered include attention and attention shift/ selective attention; memory subdomains include non-verbal memory; while perceptual motor sub-domains include visuomotor coordination and visuospatial perception. In addition, CogState’s reported construct, concurrent and convergent validity means that measurement of neurocognitive deficits is at par with other states especially considering that the CogState battery is computerized; hence, its administration and scoring is easy.
The form of standardization conducted in these tests is diverse, and though not comprehensive in some tests like Tower Test, the tools other psychometric properties have been tested in other settings like in London and Central Finland as is the case with the Tower Test (Ahonniska et al. 2000; Bishop et al. 2001). The validity and reliability findings of the tests in this review were also not widely spread across settings especially in the case of discriminant validity which despite most studies in this narrative review reporting on it, none of the studies conducted in sub-Saharan Africa reported on this form of validity. This is despite some studies having healthy and diseased populations that could be used to calculate discriminant validity of the cognitive tools. This selective testing of validity has been found to be because of authors’ preference for what is relevant to them and what is easily obtained (Hubley and Zumbo 1996). Authors tend to choose the type of validity to be tested based on the purposes for which they would like the test to be used. If they want to see whether the tool can measure attention in the same way as another validated attention test, they will choose to do convergent validity testing. When they want to show that a tool can discriminate between children with cognitive insults from the ones that are healthy, they will choose to test for discriminant validity. However distinct the types of validity are, a tool cannot be assumed to work well unless it shows evidence of reliability, correlation with variables that it is expected to correlate with and lack of correlation with variables that it is not expected to correlate as well as evidence that the tool items reflect the cultural construct (Chiang et al. 2015 (October, 13)). In most of the studies reported in this review, reliability and validity were assumed to be different entities; hence, a study could test for validity without testing for reliability. Moreover, most tests had one study reporting on their psychometric properties which should not be the practice with cognitive tools because they are sensitive to cultural experiences in development. Among the tests reviewed, The Developmental Test of Visuo-Motor Integration was the only test that reported on reliability as well as discriminant, convergent and construct validity and in addition had more than one study reporting its psychometric properties. This should be the practice among researchers before assuming that a tool works well. Educators and clinicians should check on these properties before integrating the tools into practice. Interpretation, use and relevance across different cultural settings should be the norm.
Cultural Adaptations
Adaptation processes took different dimensions each dependent on the objectives of the studies. Recommendations for cognitive tests adaptation consist of translation, piloting and test modification (Malda et al. 2008). The adaptation processes captured in this review involved changes to the tools in terms of language and items while the objectives of the study at times necessitated just the testing of different psychometric properties of full batteries or their subsets. The reviewed studies partially tapped into the recommended adaptation procedures. It is beyond the objectives of this review to make recommendations on appropriate adaptation of cognitive tests in different cultural contexts. However, some of the adapted tests resulted in cognitive tests with high validity and reliability indicators while others had low indicators. Tests such as the Behavioral Assessment and Research System (BARS) had test–retest validity ranging from low to high depending on the sub-test. The Brazilian Child Hayling Test had high content validity but low specificity; Behavior Assessment System for Children-Teacher Report was found to have high reliability, good construct validity but its predictive validity was found to be weak and partially significant; while the Kilifi toolkit was found to have moderate internal consistency, low to moderate test retest reliability and partially significant predictive validity (Kitsao-Wekulo et al. 2013b; Rohitrattana et al. 2014; Sadeh et al. 2012; Siqueira et al. 2016). The variability in psychometric indicators could be as a result of many factors including differences in test population, differences in individual task scores that may affect reliability or also the adapted test items do not reflect the cultural construct (Cooper et al. 2017).
Implications for Domains Well Covered
A total of seventy-seven and seventy-five of the studies tested the psychometric properties of tools that measure executive function and complex attention respectively.
Executive function domain has been extensively covered among preschoolers and children in early school years despite development of this domain starting at around 3–5 years and its maturity being in adolescence (Best and Miller 2010). This trend presupposes that these studies are inclined to find out the developmental trend rather than whether or not the function has reached maturity. In addition to this, the tests such as BaterÃa de EvaluaciÃn NeuropsicolÃgica Infantil (BENCI), Developmental Neuropsychological Assessment (NEPSY) and subtests of Behavioral Assessment of Dysexecutive Syndrome for Children (BADS-C) monitor executive dysfunction progression and recovery. This interest in executive function development means many tools are likely to be developed and standardized for measurement of these domains compared to other domains. In addition, the interest leads to development of different versions of the same tools in different settings.
Key Gaps and Areas for Intervention
Most of the tools have been standardized to be used in the USA, yet each setting has different cultural practices that give a different orientation to cognitive functioning. One’s environment determines cognitive development trajectory. In the USA, processing speed of information is valued in education, which may underpin quality of information which is inadvertently valued among Hispanics (Casaletto and Heaton 2017).
Only seven studies reported on the development of normative data with other studies reporting on the decision to changing the tools to make them valid. Though there is still a debate on which option to pick before integration of a tool in a certain setting, it is interesting to note that the researchers are hesitant to develop normative data. It is important for test results to be interpreted with regard to the general population as clinical data may not cover the full range of possible scores. Normative data is able to tell whether a child’s functioning score is well within that of the general population in reference to age or not (Ellingsen 2016). Normative data studies are difficult to conduct as several methods of data collection need to be integrated to obtain an ethnically diverse sample that is truly representative of the general population (Nolte et al. 2015).
Conclusion
The narrative review indicates that more needs to be done in cultural adaptation and standardization of neuropsychological tools. There is a need to extensively standardize other DSM-5 cognitive domains; adapt and standardize tools in diverse settings; and integrate diverse validity and reliability measures, as well as courageously do normative data studies.
Strengths and Limitations
A narrative review was conceptualized to be the best form of interrogating the research questions due to its nature of critically looking at and discussing the knowledge of interest. That said, there are other forms of studies that would have complemented the findings of this review such as systematic reviews. The review concentrated on studies done between 1987 and 2017 hence studies falling off this timeline were not integrated. Further, the search sites were limited to PubMed, Web of Science and Psych Infor yet there are other databases that would have generated more information. However, even though we concentrated on these three search sites, we had duplication of data a situation that would have inadvertently been described as having reached saturation level. The terms used for the search were limited to “neuropsychological” or “neurocognitive” and “assessment” or “test”. Using other terms with these ones could have increased the comprehensiveness and impact of the work. However, during screening other search terms were tried out but they resulted in the same and, in some cases, fewer results meaning this study search terms resulted in optimal and unique studies. Moreover, this search criteria resulted in many studies being screened in comparison to other cognitive review studies that have found fewer search results. In addition, narrative reviews are said to be subjective and their search criteria may not have explicit specifications (Ferrari 2015). The search did not include studies with non-English-reported findings due to lack of resources for hiring translators. However, reviews that have not included non-English publications have been found to not have systematic bias (Morrison et al. 2012; Nussbaumer-Streit et al. 2020). The search did not include data published in test manuals that was not published in research journals.
Data Availability
The data from which the results of this review were extracted can be accessed by contacting the corresponding author.
Abbreviations
- BRIEF:
-
Behaviour Rating Inventory of Executive Functioning
- WISC:
-
Wechsler Intelligence Scales
- MSVT:
-
Medical Symptom Validity Test
- TOMM:
-
Test of Memory Malingering
- WMT:
-
Word Memory Test
- CPT:
-
Continuous Performance Tests
- SWM:
-
Spatial Working Memory
- CANTAB:
-
Cambridge Neuropsychological Test Battery
- TOVA:
-
Test of Variables of Attention
- KABC:
-
Kaufman Assessment Battery for Children
- DAS:
-
Differential Ability Scales
- NEPSY:
-
Developmental Neuropsychological Assessment
- WIAT:
-
Wechsler Individual Achievement Test
- SSA:
-
Sub-Saharan Africa
- SOPT:
-
Self-Ordered Pointing Test
- VLL:
-
Verbal List Learning
- CPM:
-
Colored Progressive Matrices
- CNT:
-
Contingency Naming Test
- DSM V:
-
Diagnostic and Statistical Manual of Mental Disorders, 5th Edition
- LMIC:
-
Lower- and middle-income countries
- ANT:
-
Attention Network Test
- HRNB-C:
-
Halstead-Reitan Neuropsychological Test Battery for Children
- CANTAB:
-
Cambridge Neuropsychological Test Automated Battery
- BENCI:
-
BaterÃa de EvaluaciÃn NeuropsicolÃgica Infantil
- BADS-C:
-
Behavioral Assessment of Dysexecutive Syndrome for Children.
References
Ahonniska, J., Ahonen, T., Aro, T., Tolvanen, A., & Lyytinen, H. (2000). Repeated assessment of the Tower of Hanoi test: reliability and age effects. Assessment, 7(3), 297–310.
Ahonniska, J., Ahonen, T., Aro, T., Tolvanen, A., & Lyytinen, H. (2001). Practice effects on visuomotor and problem-solving tests by children. Perceptual and Motor Skills, 92(2), 479–494.
Bangirana, P., Seggane-Musisi., Allebeck, P., Giordani, B., John, C., Opoka, O.,. .. MJ., B. (2009). A preliminary examination of the construct validity of the KABC-II in Ugandan children with a history of cerebral malaria. African Health Sciences, 9(3).
Bangirana, P., Sikorskii, A., Giordani, B., Nakasujja, N., & Boivin, M. J. (2015). Validation of the CogState battery for rapid neurocognitive assessment in Ugandan school age children. Child and Adolescent Psychiatry and Mental Health, 9.
Best, J. R., & Miller, P. H. (2010). A developmental perspective on executive function. Child Development, 81(6). https://doi.org/10.1111/j.1467-8624.2010.01499.x.
Bishop, D. V. M., Aamodt-Leeper, G., Creswell, C., McGurk, R., & Skuse, D. H. (2001). Individual differences in cognitive planning on the Tower of Hanoi task: Neuropsychological maturity or measurement error? Journal of Child Psychology and Psychiatry, and Allied Disciplines, 42(4), 551–556.
Bradley-Johnson, S. (2001). Cognitive assessment for the youngest children: a critical review of tests. Journal of Psychoeducational Assessment, 19(1), 19–44. https://doi.org/10.1177/073428290101900102.
Budtz-Jorgensen, E., Keiding, N., Grandjean, P., & Weihe, P. (2002). Estimation of health effects of prenatal methylmercury exposure using structural equation models. Environmental Health, 1(1), 2.
Carone, D. A. (2014). Young child with severe brain volume loss easily passes the word memory test and medical symptom validity test: Implications for mild TBI. The Clinical Neuropsychologist, 28(1), 146–162. https://doi.org/10.1080/13854046.2013.861019.
Casaletto, K. B., & Heaton, R. K. (2017). Neuropsychological assessment: past and future. Journal of the International Neuropsychological Society, 23(9–10), 778–790. https://doi.org/10.1017/S1355617717001060.
Chen, X., Chen, H., Li, D., & Wang, L. (2009). Early childhood behavioral inhibition and social and school adjustment in Chinese children: a 5-year longitudinal study. Child Development, 80(6), 1692–1704. https://doi.org/10.1111/j.1467-8624.2009.01362.x.
Chiang, I. A., Jhangiani, R. S., & Price, P. C. (2015 (October, 13)). Research methods in psychology: reliability and validity of measurement (2 ed.). Canada: BC Campus.
Cooper, S. R., Gonthier, C., Barch, D. M., & Braver, T. S. (2017). The role of psychometrics in individual differences research in cognition: a case study of the AX-CPT. Frontiers in Psychology, 8, 1482–1482. https://doi.org/10.3389/fpsyg.2017.01482.
Ellingsen, K. M. (2016). Standardized assessment of cognitive development: Instruments and issues. In Early Childhood Assessment in School and Clinical Child Psychology (pp. 25-49).
Ezeamama, A. E., Bustinduy, A. L., Nkwata, A. K., Martinez, L., Pabalan, N., Boivin, M. J., & King, C. H. (2018). Cognitive deficits and educational loss in children with schistosome infection—a systematic review and meta-analysis. PLoS Neglected Tropical Diseases, 12(1), e0005524. https://doi.org/10.1371/journal.pntd.0005524.
Fasfous, Peralta-Ramirez, M. I., Perez-Marfil, M. N., Cruz-Quintana, F., Catena-Martinez, A., & Perez-Garcia, M. (2015a). Reliability and validity of the Arabic version of the computerized Battery for Neuropsychological Evaluation of Children (BENCI). Child Neuropsychology, 21(2), 210–224. https://doi.org/10.1080/09297049.2014.896330.
Ferrari, R. (2015). Writing narrative style literature reviews. Medical Writing, 24(4), 230–235. https://doi.org/10.1179/2047480615z.000000000329.
Holding, P. A., Taylor, H. G., Kazungu, S. D., Mkala, T., Gona, J., Mwamuye, B., et al. (2004). Assessing cognitive outcomes in a rural African population: development of a neuropsychological battery in Kilifi District, Kenya. Journal of the International Neuropsychological Society : JINS, 10(2), 246–260. https://doi.org/10.1017/S1355617704102166.
Hubley, A. M., & Zumbo, B. D. (1996). A dialectic on validity: where we have been and where we are going. The Journal of General Psychology, 123(3), 207–215. https://doi.org/10.1080/00221309.1996.9921273.
Hwang, Y., Hosokawa, T., Swanson, H. L., Ishizaka, I., Kifune, N., Ohira, D., & Ota, T. (2006). A Japanese short form of the Swanson cognitive processing test to measure working memory: reliability, validity, and differences in scores between primary school children of the United States and Japan. Psychological Reports, 99(1), 27–38. https://doi.org/10.2466/pr0.99.1.27-38.
Kelley, T. L. (1927). Interpretation of educational measurements. Oxford: World Book Co.
Kitsao-Wekulo, P. K., Holding, P. A., Taylor, H. G., Abubakar, A., & Connolly, K. (2013a). Neuropsychological testing in a rural African school-age population: evaluating contributions to variability in test performance. Assessment, 20(6), 776–784. https://doi.org/10.1177/1073191112457408.
Kitsao-Wekulo, P. K., Holding, P. A., Taylor, H. G., Kvalsvig, J. D., & Connolly, K. J. (2013b). Determinants of variability in motor performance in middle childhood: a cross-sectional study of balance and motor co-ordination skills. BMC Psychology, 1(1), 29–29. https://doi.org/10.1186/2050-7283-1-29.
Konstantopoulos, K., Vogazianos, P., Thodi, C., & Nikopoulou-Smyrni, P. (2015). A normative study of the Children's Color Trails Test (CCTT) in the Cypriot population. Child Neuropsychology, 21(6), 751–758.
Llorente, A. M., Voigt, R. G., Williams, J., Frailey, J. K., Satz, P., & D'Elia, L. F. (2009). Children's color trails test 1 2: -retest reliability and factorial validity. The Clinical Neuropsychologist, 23(4), 645–660.
Malda, M., Vijver, F. J. R. V. D., Transler, C., Sukumar, P., Srinivasan, K., & Rao, K. (2008). Adapting a cognitive test for a different culture: an illustration of qualitative procedures. Psychology Science Quarterly, 50(4), 451–468.
Morrison, A., Polisena, J., Husereau, D., Moulton, K., Clark, M., Fiander, M., et al. (2012). The effect of English-language restriction on systematic review-based meta-analyses: a systematic review of empirical studies. International Journal of Technology Assessment in Health Care, 28, 138–144. https://doi.org/10.1017/S0266462312000086.
Mung'ala-Odera, V., Meehan, R., Njuguna, P., Mturi, N., Alcock, K., Carter, J. A., & Newton, C. R. (2004). Validity and reliability of the 'Ten Questions' questionnaire for detecting moderate to severe neurological impairment in children aged 6-9 years in rural Kenya. Neuroepidemiology, 23(1–2), 67–72. https://doi.org/10.1159/000073977.
Nolte, M. T., Shauver, M. J., & Chung, K. C. (2015). Analysis of four recruitment methods for obtaining normative data through a Web-based questionnaire: a pilot study. Hand (N Y), 10(3), 529–534. https://doi.org/10.1007/s11552-014-9730-y.
Nussbaumer-Streit, B., Klerings, I., Dobrescu, A. I., Persad, E., Stevens, A., Garritty, C., et al. (2020). Excluding non-English publications from evidence-syntheses did not change conclusions: a meta-epidemiological study. Journal of Clinical Epidemiology, 118, 42–54. https://doi.org/10.1016/j.jclinepi.2019.10.011.
Parikh, R., Mathai, A., Parikh, S., Chandra Sekhar, G., & Thomas, R. (2008). Understanding and using sensitivity, specificity and predictive values. Indian Journal of Ophthalmology, 56(1), 45–50.
Reitan, R. M., & Wolfson, D. (2004). The Trail Making Test as an initial screening procedure for neuropsychological impairment in older children. Archives of Clinical Neuropsychology, 19(2), 281–288.
Reynolds, E., Fazio, V. C., Sandel, N., Schatz, P., & Henry, L. C. (2016). Cognitive development and the immediate postconcussion assessment and cognitive testing: a case for separate norms in preadolescents. Applied Neuropsychology: Child, 5(4), 283–293. https://doi.org/10.1080/21622965.2015.1057637.
Rohitrattana, J., Siriwong, W., Suittiwan, P., Robson, M. G., Strickland, P. O., Rohlman, D. S., & Fiedler, N. (2014). Adaptation of a neurobehavioral test battery for Thai children. Roczniki Państwowego Zakładu Higieny, 65(3), 205–212.
Rose, S. A., Feldman, J. F., Jankowski, J. J., & Van Rossem, R. (2011). Basic information processing abilities at 11 years account for deficits in IQ associated with preterm birth. Intelligence, 39(4), 198–209.
Roy, A., Allain, P., Roulin, J.-L., Fournet, N., & Le Gall, D. (2015). Ecological approach of executive functions using the Behavioural Assessment of the Dysexecutive Syndrome for Children (BADS-C): developmental and validity study. Journal of Clinical and Experimental Neuropsychology, 37(9), 956–971. https://doi.org/10.1080/13803395.2015.1072138.
Sachdev, P. S., Blacker, D., Blazer, D. G., Ganguli, M., Jeste, D. V., Paulsen, J. S., & Petersen, R. C. (2014). Classifying neurocognitive disorders: the DSM-5 approach. Nature Reviews. Neurology, 10(11), 634–642. https://doi.org/10.1038/nrneurol.2014.181.
Sadeh, S. S., Burns, M. K., & Sullivan, A. L. (2012). Examining an executive function rating scale as a predictor of achievement in children at risk for behavior problems. School Psychology Quarterly, 27(4), 236–246. https://doi.org/10.1037/spq0000012.
Siqueira, L. S., Goncalves, H. A., Hubner, L. C., & Fonseca, R. P. (2016). Development of the Brazilian version of the Child Hayling Test. Trends Psychiatry Psychother, 38(3), 164–174. https://doi.org/10.1590/2237-6089-2016-0019.
Spironello, C., Hay, J., Missiuna, C., Faught, B. E., & Cairney, J. (2010). Concurrent and construct validation of the short form of the Bruininks-Oseretsky test of motor proficiency and the movement-ABC when administered under field conditions: Implications for screening. Child: Care, Health and Development, 36(4), 499–507. https://doi.org/10.1111/j.1365-2214.2009.01066.x.
Stad, F. E., Wiedl, K. H., Vogelaar, B., Bakker, M., & Resing, W. C. M. (2019). The role of cognitive flexibility in young children’s potential for learning under dynamic testing conditions. European Journal of Psychology of Education, 34(1), 123–146. https://doi.org/10.1007/s10212-018-0379-8.
Stadskleiv, K. (2020). Cognitive functioning in children with cerebral palsy. Developmental Medicine and Child Neurology, 62(3), 283–289. https://doi.org/10.1111/dmcn.14463.
Stinnett, T. A., Oehler-Stinnett, J., Fuqua, D. R., & Palmer, L. S. (2002). Examination of the underlying structure of the NEPSY: a developmental neuropsychological assessment. Journal of Psychoeducational Assessment, 20(1), 66–82.
Syvaoja, H. J., Tammelin, T. H., Ahonen, T., Rasanen, P., Tolvanen, A., Kankaanpaa, A., & Kantomaa, M. T. (2015). Internal consistency and stability of the CANTAB neuropsychological test battery in children. Psychol Assess, 27(2), 698–709. https://doi.org/10.1037/a0038485.
Teglasi, H., Nebbergall, A. J., & Newman, D. (2012). Construct validity and case validity in assessment. Psychological Assessment, 24(2), 464–475. https://doi.org/10.1037/a0026012.
Termine, C., Luoni, C., Fontolan, S., Selvini, C., Perego, L., Pavone, F., et al. (2016). Impact of co-morbid attention-deficit and hyperactivity disorder on cognitive function in male children with Tourette syndrome: a controlled study. Psychiatry Research, 243, 263–267.
Thaler, N. S., Allen, D. N., McMurray, J. C., & Mayfield, J. (2010). Sensitivity of the test of memory and learning to attention and memory deficits in children with ADHD. Clinical Neuropsychology, 24(2), 246–264. https://doi.org/10.1080/13854040903277305.
Thomas, E., Maruff, P., Paul, J., & Reeve, R. (2016). Spatial sequence memory and spatial error monitoring in the Groton Maze Learning Task (GMLT): a validation study of GMLT sub-measures in healthy children. Child Neuropsychology, 22(7), 837–852. https://doi.org/10.1080/09297049.2015.1038989.
van Nieuwenhuijzen, M., Vriens, A., Scheepmaker, M., Smit, M., & Porton, E. (2011). The development of a diagnostic instrument to measure social information processing in children with mild to borderline intellectual disabilities. Research in Developmental Disabilities, 32(1), 358–370. https://doi.org/10.1016/j.ridd.2010.10.012.
Vriezen, E. R., & Pigott, S. E. (2002). The relationship between parental report on the BRIEF and performance-based measures of executive function in children with moderate to severe traumatic brain injury. Child Neuropsychology, 8(4), 296–303. https://doi.org/10.1076/chin.8.4.296.13505.
Williams, M. E., Sando, L., & Soles, T. G. (2014). Cognitive tests in early childhood: psychometric and cultural considerations. Journal of Psychoeducational Assessment, 32(5), 455–476. https://doi.org/10.1177/0734282913517526.
Woodward, H., & Donders, J. (1998). The performance of children with traumatic head injury on the wide range assessment of memory and learning-screening. Applied Neuropsychology, 5(3), 113–119. https://doi.org/10.1207/s15324826an0503_1.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
This study was part of a larger study whose ethical approval was sort from Tilburg University’s Research Ethics Committee (REC#2017/25) and University of Nairobi, Kenyatta National Hospital Ethics and Research Committee (P556/07/2016).
Consent for Publication
We give consent for publication of this paper.
Financial Disclosure
This study was funded through a seed grant for early career researchers organized by Partnerships for Mental Health Development in Sub-Saharan Africa (PaM-D) (NIMH award number U19MH98718) and the Kenyatta National Hospital’s Research & Programs Department.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 175 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rachel, M., Fons, V.D.V.J.R., Amina, A. et al. Assessing Neuropsychological Functions in Middle Childhood: a Narrative Review of Measures and Their Psychometric Properties Across Context. J Pediatr Neuropsychol 7, 113–138 (2021). https://doi.org/10.1007/s40817-021-00096-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40817-021-00096-9