
Abstract
Background
High levels of FGF23 associate with adverse events in CKD. The urinary fractional excretion of phosphate (FePi) might modify this association, although data are limited in moderate and advanced CKD. We investigated the association of combined FePi and serum FGF23 with incident heart failure, cardiovascular events and mortality in patients with CKD stages 2–4.
Methods
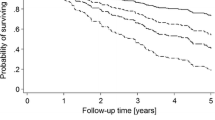
Patients from the Chronic Renal Insufficiency Cohort were divided into four groups according to the median of FePi and FGF23: low-FePi/low-FGF23, reference group; high-FePi/low-FGF23; low-FePi/high-FGF23; high-FePi/high-FGF23. Primary outcomes were: the composite of cardiovascular death or hospitalization for heart failure; cardiovascular death; hospitalization for heart failure; and death from any cause. Survival analysis and adjusted regression analyses were performed.
Results
We analyzed 3684 patients with a mean age of 58 ± 11 years of whom 45% were male. Mean eGFR was 44 ± 15 ml/min/1.73 m2. The median time of follow-up was 12 (IQR 7–13) years. The risk of the composite of cardiovascular death or hospitalization for heart failure was increased in the low-FePi/high-FGF23 group (HR 1.35; 95%CI 1.09–1.67) and in the high-FePi/high-FGF23 group (HR 1.50; 95%CI 1.20–1.86), compared to the low-FePi/low-FGF23 group. Cardiovascular death and hospitalization for heart failure were also increased in both groups with high FGF23. Death from any cause was increased in the low-FePi/high-FGF23 group (HR 1.56 (95%CI 1.30–1.89) and in the high-FePi/high-FGF23 (HR 1.57 (95%CI 1.29–1.90)).
Conclusions
High FGF23 was associated with heart failure and cardiovascular death in patients with low FePi and high FePi with moderate to advanced CKD. This contrasts with reports in mild CKD.
Graphical abstract


Similar content being viewed by others


Code and data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Balani S, Perwad F (2019) Fibroblast growth factor 23 and phosphate homeostasis. Curr Opin Nephrol Hypertens 28(5):465–473
Isakova T et al (2011) Fibroblast growth factor 23 is elevated before parathyroid hormone and phosphate in chronic kidney disease. Kidney Int 79(12):1370–1378
Marthi A et al (2018) Fibroblast growth factor-23 and risks of cardiovascular and noncardiovascular diseases: a meta-analysis. J Am Soc Nephrol 29(7):2015–2027
Fliser D et al (2007) Fibroblast growth factor 23 (FGF23) predicts progression of chronic kidney disease: the Mild to Moderate Kidney Disease (MMKD) Study. J Am Soc Nephrol 18(9):2600–2608
Almahmoud MF et al (2018) Fibroblast growth factor-23 and heart failure with reduced versus preserved ejection fraction: MESA. J Am Heart Assoc 7(18):e008334
Duran A, Joury A, Ventura HO (2021) FGF23 predicts outcomes in heart failure but questions remain unanswered. Int J Cardiol. https://doi.org/10.1016/j.ijcard.2021.06.036
Kuro-o M (2011) Phosphate and klotho. Kidney Int 79:S20–S23
Dominguez JR et al (2013) Fractional excretion of phosphorus modifies the association between fibroblast growth factor-23 and outcomes. J Am Soc Nephrol 24(4):647–654
Bellasi A et al (2019) Fractional excretion of phosphate (FeP) is associated with end-stage renal disease patients with CKD 3b and 5. J Clin Med 8(7):1026
Villodres MJ et al (2019) Fractional excretion of phosphorus and vascular calcification in stage 3 chronic kidney disease. J Investig Med 67(3):674–680
Bech AP et al (2015) Impact of fractional phosphate excretion on the relation of FGF23 with outcome in CKD patients. J Nephrol 28(4):477–484
Lash JP et al (2009) Chronic Renal Insufficiency Cohort (CRIC) study: baseline characteristics and associations with kidney function. Clin J Am Soc Nephrol 4(8):1302–1311
Phelps KR, Mason DL (2015) Parameters of phosphorus homeostasis at normal and reduced GFR: theoretical considerations. Clin Nephrol 83(3):167–176
Lang RM et al (2015) Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J-Cardiovasc Imaging 16(3):233–271
House AA et al (2019) Heart failure in chronic kidney disease: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int 95(6):1304–1317
Stöhr R et al (2018) FGF23 in cardiovascular disease: innocent bystander or active mediator? Front Endocrinol 9:351
Ix JH et al (2012) Fibroblast growth factor-23 and death, heart failure, and cardiovascular events in community-living individuals: CHS (Cardiovascular Health Study). J Am Coll Cardiol 60(3):200–207
Pavik I et al (2013) Secreted Klotho and FGF23 in chronic kidney disease Stage 1 to 5: a sequence suggested from a cross-sectional study. Nephrol Dial Transpl 28(2):352–359
Isakova T et al (2011) Fibroblast growth factor 23 and risks of mortality and end-stage renal disease in patients with chronic kidney disease. JAMA 305(23):2432–2439
Panwar B et al (2015) Fibroblast growth factor 23 and risk of incident stroke in community-living adults. Stroke 46(2):322–328
Garimella PS et al (2014) Fibroblast growth factor 23, the ankle-brachial index, and incident peripheral artery disease in the Cardiovascular Health Study. Atherosclerosis 233(1):91–96
Lim K et al (2012) Vascular Klotho deficiency potentiates the development of human artery calcification and mediates resistance to fibroblast growth factor 23. Circulation 125(18):2243–2255
Jimbo R et al (2014) Fibroblast growth factor 23 accelerates phosphate-induced vascular calcification in the absence of Klotho deficiency. Kidney Int 85(5):1103–1111
Smith ER, Holt SG, Hewitson TD (2017) FGF23 activates injury-primed renal fibroblasts via FGFR4-dependent signalling and enhancement of TGF-β autoinduction. Int J Biochem Cell Biol 92:63–78
Sanchez-Niño MD, Fernandez-Fernandez B, Ortiz A (2020) Klotho, the elusive kidney-derived anti-ageing factor. Oxford University Press, Oxford
Funding
This study was supported by the projects: (i) “New targets in diastolic heart failure: from comorbidities to personalized medicine – NETDIAMOND” co-financed by the European Structural and Investment Funds (ESIF), through the Programa Operacional Regional Lisboa 2020 (POCI-01-0145-FEDER-016385) and national funds by FCT Fundação para a Ciência e Tecnologia, I.P. (SAICT-PAC/0047/2015); and (ii) Cardiovascular R&D Center–UnIC (UIDB/00051/2020 and UIDP/00051/2020), financed by national funds through FCT–Portuguese Foundation for Science and Technology.
Author information
Authors and Affiliations
Contributions
Research idea: LM. Literature search, study design, data analysis and first manuscript draft preparation: LM, MBV, JSN. Interpretation of the results and critical revision of the manuscript: LM, MBV, JSN. Each author contributed important intellectual content during manuscript drafting or revision, accepts personal accountability for the author’s own contributions, read and approved the final manuscript and agrees to ensure that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved. LM, MBV, JSN: Responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
Corresponding author
Ethics declarations
Conflict of interest
The authors report no relationships that could be construed as a conflict of interest.
Ethical approval
The CRIC Study protocol was approved by the institutional review boards of all participating centers: the University of Pennsylvania Institutional Review Board (Federalwide Assurance # 00004028), Johns Hopkins Institutional Review Board (Study # NA_00044034/CIR00004697), The University of Maryland, Baltimore Institutional Review Board, University Hospitals Cleveland Medical Center Institutional Review Board, MetroHealth Institutional Review Board, Cleveland Clinic Foundation Institutional Review Board (IRB #5969), University of Michigan Medical School Institutional Review Board (IRBMED), Wayne State University Institutional Review Board, University of Illinois at Chicago Institutional Review Board, Tulane Human Research Protection Office, Institutional Review Boards, Biomedical Social Behavioral (reference#: 140987), and Kaiser Permanente Northern California Institutional Review Board.
Informed consent
The study is in accordance with the Declaration of Helsinki. All CRIC participants provided written informed consent.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Mendonça, L., Bigotte Vieira, M. & Neves, J.S. Association of combined fractional excretion of phosphate and FGF23 with heart failure and cardiovascular events in moderate and advanced renal disease. J Nephrol 36, 55–67 (2023). https://doi.org/10.1007/s40620-022-01358-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40620-022-01358-1