
Abstract
Objective
Few studies have examined the impact of coronavirus disease 2019 (COVID-19) on the primarily Latinx community along the U.S.-Mexico border. This study explores the socioeconomic impacts which contribute to strong predictors of severe COVID-19 complications such as intensive care unit (ICU) hospitalization in a primarily Latinx/Hispanic U.S.-Mexico border hospital.
Methods
A retrospective, observational study of 156 patients (≥ 18 years) Latinx/Hispanic patients who were admitted for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection at a U.S.-Mexico border hospital from April 10, 2020, to May 30, 2020. Descriptive statistics of sex, age, body mass index (BMI), and comorbidities (coronary artery disease, hypertension, diabetes, cancer/lymphoma, current use of immunosuppressive drug therapy, chronic kidney disease/dialysis, or chronic respiratory disease). Multivariate regression models were produced from the most significant variables and factors for ICU admission.
Results
Of the 156 hospitalized Latinx patients, 63.5% were male, 84.6% had respiratory failure, and 45% were admitted to the ICU. The average age was 67.2 (± 12.2). Those with body mass index (BMI) ≥ 25 had a higher frequency of ICU admission. Males had a 4.4 (95% CI 1.58, 12.308) odds of ICU admission (p = 0.0047). Those who developed acute kidney injury (AKI) and BMI 25–29.9 were strong predictors of ICU admission (p < 0.001 and p = 0.0020, respectively). Those with at least one reported comorbidity had 1.98 increased odds (95% CI 1.313, 2.99) of an ICU admission.
Conclusion
Findings show that age, AKI, and male sex were the strongest predictors of COVID-19 ICU admissions in the primarily Latinx population at the U.S.-Mexico border. These predictors are also likely driven by socioeconomic inequalities which are most apparent in border hospitals.
Similar content being viewed by others

Introduction
The coronavirus disease 2019 (COVID-19) pandemic has revealed sweeping health care inequalities across the United States (U.S.). Latinx, the largest ethnic minority population in the country, has been particularly affected by severe COVID-19 complications and high mortality rates [1, 2]. Latinx patients accounted for almost 1.9 times the case rate, 2.8 times the hospitalization rate, and 2.3 times the death rate compared with their White, non-Latinx counterparts in the U.S. [1]. California is also home to the largest proportion of the U.S. Latinx population [3, 4]. In June 2020, during the second surge of COVID-19, the Latinx population accounted for 45% of the total number of deaths due to COVID-19 in California [3].
The Latinx population across the U.S.-Mexico border experiences significant health disparities relative to the rest of the U.S. due to higher poverty rates, higher rates of chronic comorbidities, decreased health insurance coverage, lack of health care infrastructure, and inadequate health care access [4,5,6]. Additionally, Latinx patients are overrepresented in essential service industries, such as food services, health care, waste management, agriculture, and construction which increases their exposure risk to severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), the causative agent of COVID-19 [7, 8]. Studies of Latinx patients who were hospitalized for COVID-19 found that 25% worked in essential occupations [6, 7]. These industries, in particular, lack the infrastructure for employees to work from home and are often set in crowded areas with poor hygiene, which thus increases the risk of transmission, disease, and subsequent complications [7,8,9].
Our objective is to describe the significant risk factors that may have contributed to the disparate COVID-19 outcomes of the Latinx patients at a U.S.-Mexico border hospital. Our study was set at El Centro Regional Medical Center (ECRMC) which is the largest hospital in Imperial County and is located 12 miles north of the U.S.-Mexico border. During the time of the study, the Latinx community had the highest overall COVID-19 cases per 100,000 across all age groups when compared to their White, non-Hispanic, Black, non-Hispanic, Asian, and Native Hawaiian/Pacific Islander counterparts in California [10].
In 2020, Imperial County had the second-highest rate of COVID-19 cases and the highest COVID-19 death rate per population (304 people per 100,000) in the entire state of California [10]. At the peak of the 2020 COVID-19 pandemic, ECRMC’s patient census rose to nearly two times the normal total patient census and ten times the normal ICU census (El Centro Regional Medical Center Internal Hospital Data, 2020). At ECRMC, preliminary data demonstrated that in 2020 from March through July during the first COVID-19 surge in Imperial County, 18.7% of the 497 COVID-19 patients who were admitted died (El Centro Regional Medical Center, Internal Hospital Data, 2020).
Previous studies have demonstrated that Latinx patients are disproportionately affected by COVID-19, but there is still a paucity of research on the outcomes of Latinx patients with COVID-19 who reside along the U.S.-Mexico border [7, 8]. Our study describes the unique characteristics of the Latinx population at a border hospital which have contributed to the complications during hospitalization such as ICU admission and death among Latinx COVID-19 patients in a U.S.-Mexico border hospital.
Methods
Study Design
This was a retrospective, observational study of 156 adults who were hospitalized for severe COVID-19 and their associated outcomes at a U.S.-Mexico border hospital while operating at surge capacity serving a primarily Latinx community from April 10, 2020, to May 30, 2020. The primary outcome of interest was admission to the ICU, while the secondary outcome of interest was mortality. This retrospective study was considered exempt by our institutional review board (IRB #200,558).
Inclusion Criteria
Included within this study were patients who identified as primarily as Latinx adult patients (≥ 18 years of age) with COVID-19 diagnosed by the SARS-CoV-2 nasal pharyngeal swab polymerase chain reaction test by Abbot© who were admitted to the hospital. The patients were admitted due to their requirement for treatment and a high risk of clinical deterioration as judged by the emergency medicine clinician at the time of assessment. Admission criteria included hypoxia (O2 saturation levels < 90% on room air), tachypnea (respiratory rate > 30), visible increased work of breathing, any complication due to a coagulopathy (stroke, cardiac ischemia, pulmonary embolism), and other indicators of end-organ damage (e.g., acute renal failure).
Exclusion Criteria
Excluded from the study were those who primarily identified as not-Latinx/Hispanic, pediatric patients (< 18 years of age), pregnant women, patients who did not consent for further treatment or admission, and patients who were dead on arrival to the ED.
Materials
Study participants were identified by searching the electronic health record (EHR) (MedHost©) for chief complaints and emergency department (ED) International Classification of Disease, 9th Revision (ICD-9) and 10th revision (ICD-10), associated with COVID-19. Admitted patients were then followed throughout their hospital course through another EHR (Cerner©) while matching the patients’ unique medical record numbers to obtain treatment, laboratory, death, discharge, and length-of-stay data (in unit days). Each admitted patient’s chart was scanned for information on vital signs and the ventilation strategies including the following: nasal cannula, high-flow nasal cannula, bi-level non-invasive positive pressure (BiPAP), and endotracheal intubation.
Data Collection
A team of trained data abstractors performed a retrospective chart review of patients diagnosed with SARS-CoV-2 infection who presented to ECRMC ED from April 1, 2020, to May 30, 2020. The data abstractors were unblinded to study hypothesis and uniformly received on-site training in data extraction, identifying cases through selection criteria, and identifying specific study variables. Documentation by the treating emergency department physician and the pharmacy infusion records were reviewed by study investigators.
Variables collected included receipt of intervention, patient demographics (age, sex, body mass index (BMI), and ethnicity), and comorbidities including cardiovascular disease/hyperlipidemia, hypertension, chronic obstructive pulmonary disease, or other chronic respiratory diseases such as asthma, chronic kidney disease, diabetes mellitus, and immunosuppression (current disease state of immunosuppression or currently taking immunosuppressive medication such as immunotherapy, and anticancer drugs). These data were recorded in a password-protected, patient deidentified Microsoft Excel© sheet. Delivering oxygenation through nasal cannula, non-rebreathing masks, bi-level positive pressure ventilation, intubation, and high-flow nasal cannula were recorded as were the associated outcomes of ICU admission and mortality. Additional outcomes data were recorded including repeat ED visits, hospitalization, and transfer to outside hospitals. Follow-up on discharged/transferred patients using a regional tracking website was performed to assess whether patients were seen or admitted at a different hospital. The data were reviewed for quality and consistency throughout the abstraction process.
Statistical Analysis
Descriptive statistics were employed to describe categorical data such as sex, age groups of 18–49 and 50–64, BMI ≥ 35, and presence of at least one comorbidity (coronary artery disease, hypertension, diabetes, cancer/lymphoma, current use of immunosuppressive drug therapy, chronic kidney disease/dialysis, or chronic respiratory disease). Means and standard deviations were used to express continuous data such as age, BMI, and time since the onset of COVID-19 symptoms. T-tests were used to examine if there was a statistically significant difference between continuous variables in ICU patients versus non-ICU patients. Associations between categorical variables and the following outcomes: ICU admission and mortality were examined using chi-square tests.
Bivariate analyses were used to assess potential associations between patients’ characteristics/demographics and the outcome variables: ICU admission and mortality. Due to missing mortality data, multivariate regression models were produced for only the ICU admission outcome. Using the bivariate analyses, the most significant variables and factors for ICU admission were used to produce both the full and the final regression models. For the full multivariate regression models, an α level of 0.10 was used initially to test for significance. For the final, reduced regression model, a p-value < 0.05 was considered statistically significant and confidence intervals were reported at a level of 95%. All analyses were performed using SAS© Studio Version 3.1.0 (Cary, North Carolina, USA).
Results
A total of 169 patient records were examined and 13 patient records were excluded from the study (Fig. 1). There were 5 patient encounters that were duplicate records of visits to the ED, 2 patients with unknown outcome data, 1 pregnant patient requiring transfer to a tertiary center, 2 patients who were hospitalized for another medical diagnosis but had asymptomatic COVID-19, and 3 non-Latinx patients.

Admissions with confirmed SARS-CoV-2 at El Centro Regional Medical Center (ECRMC). Note: *5 patients with duplicate visits to the ED, 2 unknown ICU status, 1 pregnant patient requiring transfer to a tertiary center, 2 patients who were hospitalized for another medical diagnosis but had asymptomatic COVID-19, 3 non-Latinx patients
Descriptive Statistics
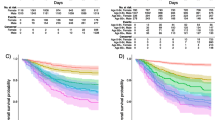
Of the 156 hospitalized patients, 71 (45.5%) required intensive care unit (ICU) level of care. Most patients were male (63.5%) with a mean body mass index (BMI) of 29.9 (± 6.7) and 50.6% were ≥ 65 years old. Tabulated frequencies of patient comorbidities are found in Table 1. A majority of the hospitalized patients were overweight (body mass index (BMI) 25–30) or obese (BMI > 30). The average age of ECRMC hospitalized COVID-19 patients overall was 64.3 years (± 14.1). There was a significant difference in the mean age of ICU admitted patients compared with non-ICU patients ages which was 67.2 (± 12.2) versus 62.3 (± 14.9), respectively (p = 0.0359). As patients were categorized into 18–49 years old, 50–64 years old, and ≥ 65 years old, there was an observed increased frequency of ICU admissions with advancing age. Seventy-one percent (44) of the 62 ICU admissions were inpatients who were ≥ 65 years old.
Patient comorbidities in association with ICU admission were analyzed. Overall, the most common comorbidities in the hospitalized patients were hypertension (66.7%), diabetes mellitus (51.9%), coronary artery disease, or hyperlipidemia (CAD/HLD) (45.5%) (Table 1). There was no significant difference in the number of comorbidities in the non-ICU admitted patients versus the ICU admitted patients (p = 0.574).
The admission complications of COVID-19 patients are shown in Table 2. Of the 156 patients who initially presented to the ED, 132 (84.6%) required respiratory support for respiratory failure in the ED. Those who were admitted to the ICU required more intensive oxygenation and ventilation. Those admitted to the ICU frequently required BiPAP, high-flow nasal cannula, or were intubated immediately in the ED (Table 2).
The development of acute kidney injury (AKI) during any time during a patient’s hospitalization appeared to be significantly associated with ICU admission (p < 0.0001). If dialysis was also utilized at any time during hospitalization, this was also associated with ICU admission (p = 0.0572). In addition, cardiovascular and coagulopathic complications, including thromboembolic disorders (deep venous thrombosis, arterial thrombosis, pulmonary embolism), ischemic stroke (CVA), and troponin elevation were found to be associated with ICU admission (p = 0.0004) (Table 2).
Mortality Outcome
The unstratified mortality outcome data were available from 148 of the 156 COVID-19 patients. Of those who were admitted to the ECRMC ICU, a total of 22 patients died, 16 patients were admitted in the ICU, and 6 were not admitted to the ICU. There were 8 patients who initially received care at ECRMC and were subsequently transferred out to a tertiary facility and mortality data were not obtained from these patients (Appendix B). There were 19 (86.4%) deaths in the ≥ 65-year-old age group. Of all the characteristics between the survivors and those who died, older age was found to be statistically significant (p < 0.0001). Additionally, patients who required dialysis (p < 0.0001) or developed AKI (p = 0.0002) during their hospitalization were less likely to survive. Among other complications, those who had developed a coagulopathic complication were associated with non-survival (p = 0.0230). As far as interventions, there was no difference in mortality for those patients who required ventilatory support in the ED versus those who did not require ventilatory support (p = 0.3655). Due to the small sample size, a chi-square analysis and subsequently a regression model could not be performed.
Multivariate Logistic Regression Models
There were 151 observations due to 5 missing data that could not be included in the models. There were 58 ICU admissions and 93 non-ICU admissions. From the bivariate analysis in the previous tables, variables used for the full multivariate logistic regression model included sex (male versus female), age categories (18–49, 50–64, and ≥ 65 years old), BMI categories (underweight, or normal, overweight, and obese), history of CAD/HLD, history of CKD, and AKI complications, cardiovascular and coagulopathic complications, and history of dialysis (Table 1 and Table 2). These variables were found to be significant at an α level of 0.10.
The full multivariate logistic regression model included sex (male versus female), age categories (18–49 years old, 50–64 years old, and ≥ 65 years old), BMI categories (underweight, or normal, overweight, and obese), CAD/HLD alone, history of chronic kidney disease, history of dialysis, complications of coagulopathy during admission, and complications of AKI (Table 3). Of these, sex, overweight BMI, age ≥ 65 years old, comorbidities, history of CAD/HLD, cardiovascular and coagulopathic complications, and AKI were found to be the most significant. The clinically relevant variables such as coronary artery disease and/or hyperlipidemia were clinically significant risk factors for both ICU admission and mortality in previous observational literature. However, cardiovascular and coagulopathic complications were not included in the final model because they were not found to be statistically significant when entered in the final model at an α level of 0.05. Therefore, in creating the final multivariate logistic regression model, age was included, along with the variables of sex, BMI, history of coronary artery disease and/or hyperlipidemia, and AKI which were significant with an α level of 0.05 (Table 3).
In the final regression model, risk factors such as male sex, age, comorbidities, and complication of AKI during hospitalization were found to be significant predictors of ICU admission. Male patients have 3.76 odds (95% CI 1.36, 10.4) of being admitted to the ICU when compared with female patients (p = 0.0053). Those in the ≥ 65-year-old age group had 5.84 (95% CI 2.03, 16.8) odds of ICU admission compared with the 50–64-year-old age category (p = 0.0011). Of the ICU admitted patients, there was a higher proportion of overweight patients than obese patients (46.8% versus 32.3%, respectively) (Table 1). Obese patients were found to have 2.61(95% CI 0.79, 8.71) odds of admission to the ICU, but limited sample size may have contributed to the insignificant p-value (p = 0.117). Out of the chronic comorbidities in our hospitalized patients, those with a documented history of coronary artery disease/hyperlipidemia had 0.19 (95% CI 0.067, 0.518) odds of ICU admission compared with those without a history of coronary artery disease/hyperlipidemia (p = 0.0013). Additionally, those who developed AKI during their hospitalization had 19.7 (95% CI 6.36, 61.1) odds of ICU admission compared with those who do not develop AKI (p < 0001). Our multivariate logistic regression analysis found that the best predictors of ICU admission at ECRMC were male sex, those ≥ 65 years of age, those who developed acute kidney injury during their hospitalization, and those who had a BMI higher than 25. Additionally, patients with a history of coronary artery disease and/or hyperlipidemia were found to have a “protective factor” against ICU admission.
Discussion
Our study has a unique focus on the COVID-19 outcomes of a Latinx population specifically at a California border hospital. As with areas with predominantly Latinx populations, Imperial County has experienced some of the worst COVID-19 outcomes compared to the rest of the state. In our study of the initial COVID-19 surge, 45% of all the Latinx ECRMC hospitalized COVID-19 patients required intensive care compared with larger observational studies that had 14.2 to 36.1% of their patients requiring ICU level of care [12, 13]. These poor outcomes are indicators of overall health inequalities that have longed plagued Latinx border population prior to COVID-19.
Multiple factors likely contribute to the disparate COVID-19 hospitalizations at the U.S.-Mexico border. First, there is an increased risk of communicable respiratory disease spread due to transborder movement of essential workers [6, 7]. Second, poor health care infrastructure increases the risk of complications and death due to delayed medical care [7,8,9]. Third, there is a high prevalence multiple medical comorbid conditions such as diabetes, hypertension, and coronary artery disease [4,5,6]. Additionally, there is an influx of the aging population with multiple medical comorbidities that are known to substantially increase the risk of hospitalization, invasive ventilation or intubation, and death associated with COVID-19 [12,13,14,15,16].
The Imperial County Border Population
An estimated total of 15 million inhabitants resides at U.S.-Mexico Border with a large proportion who are of Mexican in origin [17]. Eight-five percent of Imperial County residents identify themselves as Hispanic/Latinx with a substantial percentage of Mexican heritage [17]. There is increased U.S.-Mexico transborder movement because of U.S. economic dependency of essential workers and because of the proximity to the border (12 miles). The U.S.-Mexico border is the busiest border crossing in the world with well over 275 million border crossings and comprise of essential workers, agricultural transit in trade and commerce, and U.S. citizens visiting family or seeking health care [17, 18]. Because of the essential nature of the border crossings, these crossings were not prevented by Department of Homeland Security (DHS) COVID-19 restrictions [19]. Studies from the most recent influenza pandemic demonstrated that cross-border travel can pose an increased risk of infectious disease transmission across both sides of the U.S.-Mexico border [20].
Like other areas with large Latinx population, Imperial County also has a large proportion of their population who are overrepresented in essential service industries, such as food services, health care, waste management, agriculture, and construction which increases their exposure risk to SARS-CoV-2 [7, 8]. Studies of Latinx patients who were hospitalized for COVID-19 found that 25% worked in essential occupations [6, 7]. These industries lack the infrastructure for employees to work from home and are often set in crowded areas with poor hygiene, which thus increases the risk of transmission, disease, and subsequent complications [7,8,9].
Socioeconomic Healthcare Disparities
Imperial County has high poverty rates with approximately 20% inhabitants of living below the poverty line [21]. Poverty is associated with decreased access to health insurance coverage and health care literacy [4,5,6]. Low insurance coverage leads to diagnostics delays of preventable diseases like diabetes and hypertension because of the limited access to preventative health screenings [22]. Decreased health literacy can contribute associated with obesity and other preventable diseases. Lack of health literacy is associated with for poorer health outcomes due to increased barriers to obtain disease prevention information. This, in turn, decreases success in disease management [22].
Imperial County has an overall shortage of health care providers and hospitals. The population is being served by two hospitals: ECRMC and Pioneers Memorial Hospital and Healthcare District in Brawley, California. In 2016, Imperial County has had one of the highest ratios of population to physician in California (4890 residents to one doctor), compared to 1090:1 in California overall [23]. This uneven distribution of physicians creates a health care delivery gap across all specialties. For example, emergency physicians practice overwhelmingly in urban areas (92%), whereas 2730 (6%) were in large rural areas and 1197 (2%) in small rural areas [24]. The disparate health care distribution has created a hole through the safety net of timely treatment of preventable disease overall which then became a significant contributor to the poor COVID-19 outcomes observed in Imperial County hospitals.
Emergency Department and Healthcare Disparities
The primary and preventative health care resource vacuum is absorbed by increased utilization of the emergency departments in already under-resourced hospitals. A large international survey study has shown that patients who see a regular physician had a decreased likelihood of going to the emergency department for care [25]. In the U.S., there is an increasing number of patients who utilize the ED because of significant delays in obtaining primary care appointments in a timely manner and are often waiting up to 2 months [25,26,27,28]. A California survey examined ED utilization found that patients with chronic illnesses compared to those without chronic illnesses were as follows: (1) likely to utilize the ED over an entire lifetime, (2) have had three of more visits to the ED per year, (3) likely to have “avoidable” ED visits [28]. Because of the 24/7/365 days a year availability of an ED, patients have more immediate access to laboratory results and specialists [28]. One report demonstrated that Imperial County has a low ratio of primary care physicians to population with 21.1 primary care physicians (PCPs) per 100,000 population compared to the adjacent border county of San Diego with 51.4 PCPs per 100,000 [29]. The delay and lack of primary care coverage then increases the demand for both chronic and acute health care needs which often overwhelms the resources at local emergency departments.
Prior to COVID-19 pandemic, reportedly 90% of U.S. emergency departments suffer from overcrowding where the need for emergency services often exceeds the resources for patient care [30]. The growth in ED visits over the last few decades has exceedingly outpaced the population demand. Additionally, there is a substantial increase of complex, comorbid patients with increased acuity who require medical attention in the EDs [31, 32]. The two lone EDs in Imperial County act a safety net for basic, primary medical care in a community where there is a high prevalence of chronic medical conditions. This dependency on the EDs for primary care can contribute to the constant overcrowding [30]. Emergency departments are often under resourced and understaffed which also contributes to the overcrowding and push rural and critical access hospitals like the hospitals in Imperial County to their breaking point even prior to the COVID-19 pandemic [30,31,32]. The COVID-19 pandemic in hospitals like ECRMC are often overwhelmed with shear volumes of patients where it is often ineffective in treating patients in a timely manner [30, 31]. Resources for a crisis or a continuous mass casualty event are non-existent because of the lack of resources at baseline [30]. The overcrowding that is already in most EDs make these departments most vulnerable to poor outcomes in highly contagious respiratory infectious disease like COVID-19.
Aging Population
Older hospitalized COVID-19 patients tend to have more comorbidities which are associated with an increased risk of severe COVID-19 complications and death [12,13,14, 33, 34]. Our study observations at ECRMC support these large studies where age was a significant risk factor for ICU admission and mortality, especially in the ≥ 65-year-old age category. Because there is a strong association of morbidity and mortality secondary to COVID-19 in older individuals, there has been a concerted effort to prioritize of both treatments and vaccines for 65-year-old and older age population [12,13,14, 33,34,35]. The aging population has increased precipitously over the last few decades in the U.S. with over a third (13,787,044) of the U.S. population which is now 65 years old and over, and this has been increasingly more evident in California overall [21]. Imperial County, like much of the rest of California, has had a 198% population increase over the last decade of those aged 65 years and older [21, 36]. Thus, the elderly population in Imperial County were the most vulnerable to severe COVID-19 complications in the often-overwhelmed emergency departments.
Male Sex
Males hospitalized for COVID-19 are at increased risk of becoming admitted to the ICU and dying when compared with females [12, 13, 23,24,25]. Our study supported this observation of male sex increased risk of COVID-19 ICU admission. Additionally, male patients had a higher prevalence of chronic conditions such as hypertension, diabetes, coronary heart disease, obstructive pulmonary disease, nicotine dependence, and heart failure compared with females which directly contribute to increased risk of COVID-19 ICU hospitalization and mortality [37, 39].
Social and behavioral factors can increase the risk for COVID-19 exposure and subsequent complications. Additionally, Latinx population is more likely to be disproportionately represented in essential industries that often increase exposure to SARS-CoV-2 infection. Males, in general, are often employed in food processing, transportation, construction, and manufacturing jobs—all of which are considered essential work during the pandemic [8, 38]. Many of those who reside in Imperial County work in the agricultural industry which accounts for approximately half of all employment [40, 41].
BMI
Obesity has become increasingly prevalent over the past few decades in the US. Compared to their non-Hispanic/White counterparts, Latinx populations also have higher rates elevated BMI (BMI > 25) [42]. Obesity is known to increase chronic comorbidities such as diabetes, hypertension, and hyperlipidemia, which in turn increases the risk for severe COVID-19 complications [1, 42,43,44]. According to California Health Interview Survey in 2009, 62% of Imperial County adults reported being overweight or obese, compared to 51% statewide. In Imperial County, 31% of the adult residents were obese (BMI > 30), compared to the rest of California overall (23%) [45]. It is with urbanization and increased exposure to Western style diets and lifestyle which has largely affected the health [46]. Often it is the children of subsequent generations of immigrants where increased exposure to Western diet and lifestyle will increase the risk of higher BMI and body fat percentage at baseline. In Imperial County, most of the residents are largely native residents of the US [45, 46].
Several prior observational studies have demonstrated that elevated BMI in patients increases the risk of respiratory failure and thus ICU admission and endotracheal intubation in COVID-19 patients [12,13,14, 42,43,44]. In our study, of the 62 patients who had an ICU admission, 79% (49) were classified as overweight or obese (Table 1). Although ICU admission was more frequently observed in the ≥ 65-year-old age group, the younger population of hospitalized 18–49-year-old patients was also likely to be obese or overweight (Appendix B, Table 3). Mechanical ventilation was frequently required due to respiratory failure in ICU patients with COVID-19 (Appendix B). Our regression model shows that even a BMI 24.5–29.9 was significantly associated with ICU admissions compared to those with normal BMI. Obesity also had an increased odds of ICU admission, but this was not statistically significant (p = 0.249). This discrepancy could be partially explained by the small sample size and may highlight the non-linear relationship between increasing BMI with the odds of ICU admission.
Acute Kidney Injury
While hospitalized, comorbidities have been shown to increase the risk of acute kidney injury (AKI) in patients. Diabetes, hypertension, and cardiovascular disease are very prevalent in the Imperial Valley [23]. These comorbidities increase the risk of AKI development [47, 48]. Multiple studies have demonstrated that AKI is a common complication for hospitalized COVID-19 patients and is associated with both ICU admission and mortality [49,50,51,52,53]. Our ECRMC patients who developed AKI at any time during hospitalization had increased odds of ICU level of care compared with those who did not have AKI. Patients who have been diagnosed with diabetes and hypertension may already have an upregulation of ACE2 receptors, which may contribute to an increased risk of severe COVID-19 secondary to direct renal damage due to SARS-CoV-2 [53, 54].
Limitations
This was a single-center, retrospective analysis of hospitalized COVID-19 patients at one hospital near the U.S.-Mexico border. While not representative of the general population, the emergent response at an under-resourced hospital may be reflective of many U.S-Mexico border hospitals that serve a large proportion of Latinx patients. Although few studies primarily investigated the impacts of Latinx populations, there have not been many studies on the Latinx patients at the U.S.-Mexico border.
Our number of observations is small. Comorbidities and obesity are both known to increase COVID-19 complications and disease severity such as ICU admission and death [11,12,13,14, 43]. But some well-established correlations could not be completely reflected because of the likely bias of a small sample size. Additionally, the overrepresentation of the 50–64-year-old age group also had more comorbidities which may have led to an increased risk of ICU admission. The reported history of coronary artery disease and/or hyperlipidemia was found to be protective against ICU admissions which could be partially explained by the chronic use of statin medications in this group of hospitalized COVID-19 patients [55]. Some observational studies on patients who have been admitted for COVID-19 have also demonstrated that taking lipid-lowering medications such as statins could potentially decrease the risk of developing severe COVID-19 and decrease the recovery time among patients with severe disease [55,56,57]. Perhaps a larger sample size may demonstrate that there is little association between the use of statins and protection against severe COVID-19. Statins have shown some theoretical anti-inflammatory, anti-thrombotic, and immunomodulatory functions which could be potentially decrease the risk of severe COVID-19 development [56].
Additionally, the data from this study was performed during a surge and therefore some data was incomplete and was inevitably excluded. This led to sample sizes that were insufficient in eliminating sampling bias. Despite the lack of complete data for some common complications due to COVID-19, our study supports prior findings and highlights the poor outcomes in this Latinx border population.
Future Studies
At the time of writing this study, there have been several variants of concern (VOCs) including delta, gamma, lambda, and omicron [26, 58, 59]. These VOCs have been contributing to an increased number of cases across the U.S. Most recently, Imperial County has one of the highest vaccination rates per population with 94% completely vaccinated and 44% with boosters against SARS-CoV-2 [45].
We hope that this observational study will call attention to the need to study the true impacts of infectious diseases like COVID-19 on the Latinx border population. Future research efforts can be potentially focused on addressing the underlying the health care disparities that make the health care system and the population at U.S.-Mexico border more vulnerable to poor outcomes from catastrophic events. Other research should also focus on the lessons learned from the COVID-19 pandemic that can be used to prepare for future catastrophic events that will overwhelm the emergency departments in under-resourced border hospitals.
Conclusion
More research is starting to develop on the impacts COVID-19 on the Latinx community; however, there is still little known in regard to the Latinx U.S. border population and COVID-19. Our study highlights the underlying socioeconomic and health care disparities which likely contribute to the significant disparity of COVID-19 outcomes in the Latinx/Hispanic U.S.-Mexico border population.
Data Availability
The data obtained for this study can be found under restricted access at https://doi.org/10.5281/zenodo.6430637.
Code Availability
The SAS © Code used to analyze the data obtained for this study can be found under restricted access at https://doi.org/10.5281/zenodo.6430637.
References
Centers for Disease Control and Prevention. Risk for COVID-19 infection, hospitalization, and death by race/ethnicity. 2021; https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html. Accessed July 25, 2021.
Rodriguez-Diaz CE, Guilamo-Ramos V, Mena L, Hall E, Honermann B, Crowley JS, Baral S, Prado GJ, Marzan-Rodriguez M, Beyrer C, Sullivan PS, Millett GA. Risk for COVID-19 infection and death among Latinos in the United States: examining heterogeneity in transmission dynamics. Ann Epidemiol. 2020;52:46-53.e2. https://doi.org/10.1016/j.annepidem.2020.07.007.
United States-Mexico Border Health Commission. Border lives health status in the United States- Mexico border region order lives health status in the United States-Mexico border region. 2010; https://www.ruralhealthinfo.org/assets/940-3105/health-status-in-the-united-states-mexico-border-region.pdf. Accessed 20 July 2021.
Substance Abuse and Mental Health Services Administration. Double Jeopardy: COVID-19 and behavioral health disparities for Black and Latino communities in the U.S. 2020; https://www.samhsa.gov/sites/default/files/covid19-behavioral-health-disparities-black-latino-communities.pdf. Accessed 25 July 2021.
Lady B, Henning-Smith C, Kunz S. NRHA border health policy brief. National Rural Health Association (NRHA) Border Health Initiative. 2018; https://www.ruralhealth.us/NRHA/media/Emerge_NRHA/Advocacy/Policy%20documents/05-11-18-NRHA-Policy-Border-Health.pdf. Accessed 21 July 2021.
Institute for Health Metrics and Evaluation. US county profile: Imperial County, California. IHME. 2016; http://www.healthdata.org/sites/default/files/files/county_profiles/US/2015/County_Report_Imperial_County_California.pdf. Accessed 20 May 2021.
Macias Gil R, Marcelin JR, Zuniga-Blanco B, Marquez C, Mathew T, Piggott DA. COVID-19 pandemic: disparate health impact on the Hispanic/Latinx population in the United States. J Infect Dis. 2020;222(10):1592–5. https://doi.org/10.1093/infdis/jiaa474.
Podewils LJ, Burket TL, Mettenbrink C, Steiner A, Seidel A, Scott K, Cervantes L, Hasnain-Wynia R. Disproportionate incidence of COVID-19 infection, hospitalizations, and deaths among persons identifying as Hispanic or Latino - Denver, Colorado March-October 2020. MMWR Morb Mortal Wkly Rep. 2020;69(48):1812–6. https://doi.org/10.15585/mmwr.mm6948a3.
Honein MA, Christie A, Rose DA, Brooks JT, Meaney-Delman D, Cohn A, Sauber-Schatz EK, Walker A, McDonald LC, Liburd LC, Hall JE, Fry AM, Hall AJ, Gupta N, Kuhnert WL, Yoon PW, Gundlapalli AV, Beach MJ, Walke HT. Summary of guidance for public health strategies to address high levels of community transmission of SARS-CoV-2 and related deaths. MMWR Morb Mortal Wkly Rep. 2020;69(49):1860–7. https://doi.org/10.15585/mmwr.mm6949e2.
Hsu P, Hayes-Bautista DE. The epidemiology of diversity: COVID-19 case rate patterns in California. J Immigr Minor Health. 2021;23(4):857–62. https://doi.org/10.1007/s10903-021-01159-x.
Imperial County Public Health Department. Imperial county public health status report; 2017. p. 2015–2016; https://www.icphd.org/media/managed/medicalproviderresources/HEALTH_STATUS_2015_2016_final.pdf. Accessed 20 April 2021.
Kim L, Garg S, O’Halloran A, Whitaker M, Pham H, Anderson EJ, Armistead I, Bennett NM, Billing L, Como-Sabetti K, Hill M, Kim S, Monroe ML, Muse A, Reingold AL, Schaffner W, Sutton M, Talbot HK, Torres SM, Yousey-Hindes K, et al. Risk factors for intensive care unit admission and in-hospital mortality among hospitalized adults identified through the US coronavirus disease 2019 (COVID-19)-associated hospitalization surveillance network (COVID-NET). Clin Infect Dis. 2021;72(9):e206–14. https://doi.org/10.1093/cid/ciaa1012.
Petrilli CM, Jones SA, Yang J, Rajagopalan H, O’Donnell L, Chernyak Y, Tobin KA, Cerfolio RJ, Francois F, Horwitz LI. Factors associated with hospital admission and critical illness among 5279 people with Coronavirus Disease 2019 in New York City: Prospective cohort study. BMJ. 2020;369:m1966. https://doi.org/10.1136/bmj.m1966.
Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW, Barnaby DP, Becker LB, Chelico JD, Cohen SL, Cookingham J, Coppa K, Diefenbach MA, Dominello AJ, Duer-Hefele J, Falzon L, Gitlin J, Hajizadeh N, Harvin TG, Hirschwerk DA. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA. 2020;323(20):2052. https://doi.org/10.1001/jama.2020.6775.
United States Census Bureau. 65 and older population grows rapidly as baby boomers age (Release No. CB20–99). 2020; https://www.census.gov/newsroom/press-releases/2020/65-older-population-grows.html. Accessed 20 July 2021.
California Department of Aging. (n.d.). Facts about California's elderly. https://aging.ca.gov/Data_and_Reports/Facts_About_California's_Elderly/. Accessed 3 October 2021.
Lady B, Henning-Smith C, Kunz S (2018) NRHA border health policy brief. National Rural Health Association (NRHA) Border Health Initiative. https://www.ruralhealth.us/NRHA/media/Emerge_NRHA/Advocacy/Policy%20documents/05-11-18-NRHA-Policy-Border-Health.pdf. Accessed 21 Jul 2021
Bureau of Transportation Statistics (2019) https://www.bts.gov/browse-statistical-products-and-data/border-crossing-data/border-crossingentry-data. Accessed 1 June 2021
DHS measures on the border to limit the further spread of coronavirus. Department of Homeland Security. https://www.dhs.gov/news/2020/05/20/fact-sheet-dhs-measures-border-limit-further-spread-coronavirus. Accessed 27 May 2020
MacPherson DW, Gushulak BD, Baine WB, et al. Population mobility, globalization, and antimicrobial drug resistance. Emerg Infect Dis. 2009;15(11):1727–32. https://doi.org/10.3201/eid1511.090419.
United States Census Bureau (2020) https://www.census.gov/library/publications/2007/acs/acs-03.html. Accessed 24 Jul 2021
Prentice JC, Pizer SD. Delayed access to health care and mortality. Health Serv Res. 2007;42(2):644–62. https://doi.org/10.1111/j.1475-6773.2006.00626.x).
Imperial County Department of Public Health (2019) https://www.icphd.org/media/managed/medicalproviderupdates/HEALTH_STATUS_REPORT_2018_2019_final_.pdf. Accessed 3 Nov 2022
Bennett CL, Sullivan AF, Ginde AA, Rogers J, Espinola JA, Clay CE, Camargo CA Jr. National Study of the Emergency Physician Workforce, 2020. Ann Emerg Med. 2020;76(6):695–708.
van den Berg MJ, van Loenen T, Westert GP. Accessible and continuous primary care may help reduce rates of emergency department use. An international survey in 34 countries. Family Pract. 2016;33(1):42–50. https://doi.org/10.1093/fampra/cmv082.
Office of the Inspector General. Access to care: provider availability in Medicaid managed care [Internet]. Washington D.C.: Department of Health and Human Services. 2014; Nov. Report No.: OEI-02–13–00670. http://oig.hhs.gov/oei/reports/oei-02-13-00670.pdf.
Rust G, Ye J, Baltrus P, Daniels E, Adesunloye B, Fryer GE. Practical barriers to timely primary care access: impact on adult use of emergency department services. Arch Intern Med. 2008;168(15):1705–10. https://doi.org/10.1001/archinte.168.15.1705.
Harris Interactive Survey Collected for the California Healthcare Foundation. Emergency Department Utilization in California- Survey of Consumer Data and Physician Data (2005). https://www.chcf.org/wp-content/uploads/2017/12/PDF-EDOveruseSurveyFindings.pdf. Accessed 3 Nov 2022
Gaines, Robbin. California Health Care Foundation. California maps: how many primary care and specialist physicians are in your county? 2017. https://www.chcf.org/publication/california-maps-primary-care-specialist-physicians-county/#related-links-and-downloads. Accessed 3 Nov 2022
Kelen GD, Wolfe R, D’Onofrio G, Mills AM, Diercks D, Stern SA, Wadman MC, Sokolove PE. Emergency department crowding: the Canary in the Health Care System. NEJM Catalyst Commentary (2021). https://doi.org/10.1056/CAT.21.0217
Weiss SJ, Derlet R, Arndahl J, Ernst AA, Richards J, Fernández-Frankelton M, Schwab R, Stair TO, Vicellio P, Levy D, Brautigan M, Johnson A, Nick TG. Estimating the degree of emergency department overcrowding in academic medical centers results of the National ED Overcrowding Study (NEDOCS). Acad Emerg Med. 2004;11:38–50. https://doi.org/10.1197/j.aem.2003.07.017.
American College of Emergency Physicians (ACEP). Policy statement crowding 2019. https://www.acep.org/globalassets/new-pdfs/policy-statements/crowding.pdf. Accessed 2 Nov 2022
Rosenthal N, Cao Z, Gundrum J, Sianis J, Safo S. Risk factors associated with in-hospital mortality in a US national sample of patients with COVID-19. JAMA Netw Open. 2020;3(12):e2029058. https://doi.org/10.1001/jamanetworkopen.2020.29058.
Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S, Huang H, Zhang L, Zhou X, Du C, Zhang Y, Song J, Wang S, Chao Y, Yang Z, Xu J, Zhou X, Chen D, Xiong W, Xu L, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with Coronavirus Disease 2019 pneumonia in Wuhan. China JAMA Internal Medicine. 2020;180(7):934–43. https://doi.org/10.1001/jamainternmed.2020.0994.
Centers for Disease Control and Prevention. Vaccine recommendations for older adults. 2021; https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/older-adults.html. Accessed 3 Oct 2021
California Department of Aging .2021; https://aging.ca.gov/Data_and_Reports/Facts_About_California's_Elderly/. Accessed 3 Oct 2021
Griffith DM, Sharma G, Holliday CS, Enyia OK, Valliere M, Semlow AR, Stewart EC, Blumenthal RS. Men and COVID-19: a biopsychosocial approach to understanding sex differences in mortality and recommendations for practice and policy interventions. Prev Chronic Dis. 2020;17:E63. https://doi.org/10.5888/pcd17.200247.
Jain V, Yuan JM. Predictive symptoms and comorbidities for severe COVID-19 and intensive care unit admission: a systematic review and meta-analysis. Int J Public Health. 2020;65(5):533–46. https://doi.org/10.1007/s00038-020-01390-7.
Pijls BG, Jolani S, Atherley A, Derckx RT, Dijkstra J, Franssen G, Hendriks S, Richters A, Venemans-Jellema A, Zalpuri S, Zeegers MP. Demographic risk factors for COVID-19 infection, severity, ICU admission and death: a meta-analysis of 59 studies. BMJ Open. 2021;11(1):e044640. https://doi.org/10.1136/bmjopen-2020-044640.
Waltenburg MA, Rose CE, Victoroff T, Butterfield M, Dillaha JA, Heinzerling A, Chuey M, Fierro M, Jervis RH, Fedak KM, Leapley A, Gabel JA, Feldpausch A, Dunne EM, Austin C, Pedati CS, Ahmed FS, Tubach S, Rhea C, Tonzel J. Coronavirus disease among workers in food processing, food manufacturing, and agriculture workplaces. Emerg Infect Dis. 2021;27(1):243–9. https://doi.org/10.3201/eid2701.203821.
El Centro Chamber of Commerce. 2010; Community. https://web.archive.org/web/20101103174411/http:/elcentrochamber.org/the-city-of-el-centro/community/. Accessed 1 Aug 2021
Centers for Disease Control. 2019; Health United States, 2018. Table 26. Accessed 1 August 2022. https://www.cdc.gov/nchs/data/hus/hus18.pdf.
Stefan N, Birkenfeld AL, Schulze MB, Ludwig DS. Obesity and impaired metabolic health in patients with COVID-19. Nat Rev Endocrinol. 2020;16(7):341–2. https://doi.org/10.1038/s41574-020-0364-6.
Fang L, Karakiulakis G, Roth M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir Med. 2020;8(4):e21. https://doi.org/10.1016/S2213-2600(20)30116-8.
Imperial County Department of Public Health. Obesity. 2022 . https://www.icphd.org/health-information-and-resources/data-&-statistics/other-reports/obesity/#:~:text=Thirty%2Done%20percent%20of%20Imperial,for%20California%20overall%20(23%25. Accessed 1 Nov 2022
Lopez DI, Chacon L, Vasquez D, Brown LD. Body composition outcomes of Healthy Fit and the role of acculturation among low-income Hispanics on the US-Mexico border. BMC Public Health. 2021;21:976. https://doi.org/10.1186/s12889-021-11015-0.
Farooqi S, Dickhout JG. Major comorbid disease processes associated with increased incidence of acute kidney injury. World journal of nephrology. 2016;5(2):139–46. https://doi.org/10.5527/wjn.v5.i2.139.
Loutradis C, Pickup L, Law JP, Dasgupta I, Townend JN, Cockwell P, Sharif A, Sarafidis P, Ferro CJ. Acute kidney injury is more common in men than women after accounting for socioeconomic status, ethnicity, alcohol intake and smoking history. Biol Sex Differ. 2021;12(1):30. https://doi.org/10.1186/s13293-021-00373-4.
Ali H, Daoud A, Mohamed MM, Salim SA, Yessayan L, Baharani J, Murtaza A, Rao V, Soliman KM. Survival rate in acute kidney injury superimposed COVID-19 patients: a systematic review and meta-analysis. Renal Failure. 2020;42(1):393–7. https://doi.org/10.1080/0886022X.2020.1756323.
Chan L, Chaudhary K, Saha A, Chauhan K, Vaid A, Zhao S, Paranjpe I, Somani S, Richter F, Miotto R, Lala A, Kia A, Timsina P, Li L, Freeman R, Chen R, Narula J, Just AC, Horowitz C, Fayad Z, et al. Mount Sinai COVID Informatics. Center AKI in Hospitalized Patients with COVID-19. J American Soc Nephrol. 2021;32(1):151–60.
Hardenberg JB, Luft FC. Covid-19, ACE2 and the kidney. Acta Physiolog. 2020;230(1):e13539. https://doi.org/10.1111/apha.13539.
Hirsch JS, Ng JH, Ross DW, Sharma P, Shah HH, Barnett RL, Hazzan AD, Fishbane S, Jhaveri KD, Northwell, COVID-19 Research Consortium, & Northwell Nephrology COVID-19 Research Consortium. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 2020;98(1):209–18. https://doi.org/10.1016/j.kint.2020.05.006.
Ng JH, Bijol V, Sparks MA, Sise ME, Izzedine H, JhaveriKD,. Pathophysiology and pathology of cute kidney injury in patients with COVID-19. Adv Chron Kidney Dis. 2020;27(5):365–76. https://doi.org/10.1053/j.ackd.2020.09.003.
Sharma P, Uppal NN, Wanchoo R, Shah HH, Yang Y, Parikh R, Khanin Y, Madireddy V, Larsen CP, Jhaveri KD, Bijol V, Northwell Nephrology COVID-19 Research Consortium. COVID-19-associated kidney injury. A case series of kidney biopsy findings. Journal of the American Society of Nephrology. 2020;31(9):1948–58. https://doi.org/10.1681/ASN.2020050699.
Daniels LB, Ren J, Kumar K, Bui QM, Zhang J, Zhang X, Sawan MA, Eisen H, Longhurst CA, Messer K. Relation of prior statin and anti-hypertensive use to severity of disease among patients hospitalized with COVID-19: findings from the American Heart Association’s COVID-19 Cardiovascular Disease Registry. PLoS ONE. 2021;16(7):e0254635. https://doi.org/10.1371/journal.pone.0254635.
Reiner Ž, Hatamipour M, Banach M, Pirro M, Al-Rasadi K, Jamialahmadi T, Radenkovic D, Montecucco F, Sahebkar A. Statins and the COVID-19 main protease: in silico evidence on direct interaction. Arch Med Sci. 2020;16(3):490–6. https://doi.org/10.5114/aoms.2020.94655.
Castiglione V, Chiriacò M, Emdin M, Taddei S, Vergaro G. Statin therapy in COVID-19 infection. Eur Heart J Cardiovas Pharmacoth. 2020;6(4):258–9. https://doi.org/10.1093/ehjcvp/pvaa042.
Centers for Disease Control and Prevention. COVID-19 laboratory-confirmed hospitalizations. CDC COVID-NET. https://gis.cdc.gov/grasxp/COVIDNet/COVID19_5.html. Accessed 26 Jul 2021
World Health Organization. Tracking SARS-CoV-2 variants. 2021. https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/. Accessed 14 Sept 2021
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Faith C. Quenzer, Ashley Williams, Andrew T. Lafree, Sten Kajitani, George Mathen, Vanessa Villegas, Kari M. Kajitani, and Christian Tomaszewski. The first draft of the manuscript was written by Faith C. Quenzer, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval
This is a retrospective, observational study which was conducted on already available data, for which formal consent was not needed. The UC San Diego Research Ethics Committee has confirmed that our study is IRB exempt and not requiring approval per their board.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Quenzer, F.C., Coyne, C.J., Ferran, K. et al. ICU Admission Risk Factors for Latinx COVID-19 Patients at a U.S.-Mexico Border Hospital. J. Racial and Ethnic Health Disparities 10, 3039–3050 (2023). https://doi.org/10.1007/s40615-022-01478-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40615-022-01478-1