
Abstract
Background
We sought to quantify socioeconomic disparities in patients with severe aortic stenosis (AS) undergoing transcatheter aortic valve replacement (TAVR) at an urban, tertiary referral center.
Methods
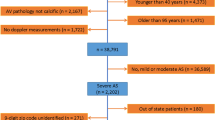
This retrospective case-control study identified 67 patients with severe AS (aortic valve [AV] area ≤1 cm2 or AV area index ≤0.60 cm2/m2 or AV velocity ≥40 mmHg) who underwent TAVR from November 5, 2013 to June 10, 2014. Study subjects were matched to controls with severe AS without TAVR in a 4:1 age-frequency match. Demographic data were collected using electronic medical records. Area-based median household income was obtained by geocoding patients’ addresses and linking with census data. Charlson comorbidity index for all subjects was calculated.
Results
Income disparity was significant in that with every $10,000 increase in income, the odds of receiving TAVR increased by 10% (p = 0.05). Non-blacks were significantly more likely to receive TAVR than blacks (odds ratio [OR] 2.812, confidence interval [CI] 1.007–7.853; p = 0.048). No differences in comorbidities were found between the two groups. Post hoc analysis to identify etiologies of the found disparities examined differences of AV area and AV area index, indication for two-dimensional echocardiography (echo), symptoms prior to echo, and action after echo within the control group. Black race significantly impacted the TAVR status despite the same AV area (OR 0.33, CI 0.09–0.97, p = 0.043). After echo, blacks were more likely to decline AVR, be lost to follow-up, and not be referred to cardiology (OR 4.41, CI 1.43–13.64; p = 0.010).
Conclusion
Socioeconomic and racial disparities were associated with patients with severe AS receiving TAVR at a major referral center. This study emphasizes the importance of improving access to standard of care for these subgroups of cardiac patients.

Similar content being viewed by others

References
Pilote L, Joseph L, Belisle P, Penrod J. Universal health insurance coverage does not eliminate inequities in access to cardiac procedures after acute myocardial infarction. Am Heart J. 2003;146:1030–7.
Rose KM, Foraker RE, Heiss G, Rosamond WD, Suchindran CM, Whitsel EA. Neighborhood socioeconomic and racial disparities in angiography and coronary revascularization: the ARIC surveillance study. Ann Epidemiol. 2012;22:623–9.
Yeung M, Kerrigan J, Sodhi S, et al. Racial differences in rates of aortic valve replacement in patients with severe aortic stenosis. Am J Cardiol. 2013;112:991–5.
Philbin EF, McCullough PA, DiSalvo TG, Dec GW, Jenkins PL, Weaver WD. Socioeconomic status is an important determinant of the use of invasive procedures after acute myocardial infarction in New York State. Circulation. 2000;102:III107–15.
Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:521–643.
Osnabrugge RL, Mylotte D, Head SJ, et al. Aortic stenosis in the elderly: disease prevalence and number of candidates for transcatheter aortic valve replacement: a meta-analysis and modeling study. J Am Coll Cardiol. 2013;62:1002–12.
Deutsch MA, Krane M, Bleiziffer S, Lange R. Health-related quality of life after transcatheter aortic valve replacement. J Am Coll Cardiol. 2013;61:108.
Svensson LG, Blackstone EH, Rajeswaran J, et al. Comprehensive analysis of mortality among patients undergoing TAVR: results of the PARTNER trial. J Am Coll Cardiol. 2014;64:158–68.
Vavalle JP, Phillips HR, Holleran SA, et al. Analysis of geographic variations in the diagnosis and treatment of patients with aortic stenosis in North Carolina. Am J Cardiol. 2014;113:1874–8.
Cook NL, Ayanian JZ, Orav EJ, Hicks LS. Differences in specialist consultations for cardiovascular disease by race, ethnicity, gender, insurance status, and site of primary care. Circulation. 2009;119:2463–70.
Callier JG, Brown SC, Parsons S, Ardoin PJ, Cruise P. The effect of race and gender on invasive treatment for cardiovascular disease. J Cult Divers. 2004;11:80–7.
Capers IV Q, Sharalaya Z. Racial disparities in cardiovascular care: a review of culprits and potential solutions. J Racial Ethn Health Dispar. 2014;1:171–89.
Barber S, Hickson DA, Kawachi I, et al. Neighborhood disadvantage and cumulative biological risk among a socioeconomically diverse sample of African American adults: an examination in the Jackson Heart Study. J Racial Ethn Health Dispar. 2016;3:444–56.
Minha S, Barbash IM, Magalhaes MA, et al. Outcome comparison of African-American and Caucasian patients with severe aortic stenosis subjected to transcatheter aortic valve replacement: a single-center experience. Catheter Cardiovasc Interv. 2015;85:640–7.
Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63:2438–88.
Amato MC, Moffa PJ, Werner KE, Ramires JA. Treatment decision in asymptomatic aortic valve stenosis: role of exercise testing. Heart. 2001;86:381–6.
Alter DA, Naylor CD, Austin P, Tu JV. Effects of socioeconomic status on access to invasive cardiac procedures and on mortality after acute myocardial infarction. N Engl J Med. 1999;341:1359–67.
Patel DK, Green KD, Fudim M, Harrell FE, Wang TJ, Robbins MA. Racial differences in the prevalence of severe aortic stenosis. J Am Heart Assoc. 2014;3:e000879.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No funding was received for this study.
Conflict of Interest
Dr. O’Neill has served as a proctor and consultant for Edwards Lifesciences, has served as a consultant for St. Jude Medical and Medtronic, and is the director of Neovasc Inc. All other authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Sleder, A., Tackett, S., Cerasale, M. et al. Socioeconomic and Racial Disparities: a Case-Control Study of Patients Receiving Transcatheter Aortic Valve Replacement for Severe Aortic Stenosis. J. Racial and Ethnic Health Disparities 4, 1189–1194 (2017). https://doi.org/10.1007/s40615-016-0325-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40615-016-0325-x