
Abstract
Purpose
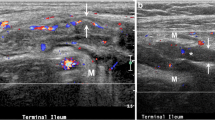
The aim of this work is to investigate the role of power Doppler sonography as an additional predictor of surgical recurrence in Crohn’s disease.
Methods
A sample of 33 patients, with ileal or ileocolonic Crohn’s disease, that had underwent intestinal resection, were retrospectively enrolled. All patients had bowel ultrasonography 7–16 months after resection. Power Doppler sonography of the preanastomotic ileum was evaluated as a possible prognostication tool to assess the risk of long-term need for reoperation.
Results
The absolute incidence of surgical recurrence in those who had a positive power Doppler was 42 %, while that of those who had a negative power Doppler was 28.6 %. Combining the power Doppler with bowel wall thickness, the surgical recurrence risk grew from 41.2 % of those with a positive power Doppler and thickness >3 mm to 55.6 % of those with a positive power Doppler and thickness >6 mm.
Conclusions
Power Doppler look to be another useful prediction tool for the personalization of patient’s care. It could be useful to perform power Doppler in all patients with a wall thickness >5 mm: for those who have a positive power Doppler it may be indicated as a more aggressive prophylactic therapy.
Riassunto
Scopo
L’obiettivo di questo lavoro è investigare il ruolo del power Doppler ecografico come fattore predittivo aggiuntivo della recidiva chirurgica nella malattia di Crohn.
Metodo
Un campione di 33 pazienti, con malattia di Crohn ileale o ileo-colica, che sono stati sottoposti a resezione intestinale, sono stati arruolati retrospettivamente. A tutti i pazienti è stata effettuata un’ecografia intestinale nei 7–16 mesi successivi alla resezione. E’ stato valutato il power Doppler ecografico dell’ileo pre-anastomotico come un possibile predittore del rischio di necessità di una nuova operazione nel lungo termine.
Risultati
L’incidenza assoluta di recidiva chirurgica nei pazienti con power Doppler positivo è risultata essere del 42 %, mentre quella nei pazienti con power Doppler negativo è risultata essere del 28.6 %. Unendo i risultati del power Doppler con quelli dello spessore di parete, il rischio di recidiva chirurgica aumenta dal 41.2 % di quelli con power Doppler positivo e spessore di parete intestinale >3 mm al 55.6 % di quelli con power Doppler positivo e spessore di parete >6 mm.
Conclusioni
Il power Doppler sembra essere un ulteriore utile fattore predittivo per personalizzare la terapia del paziente. Potrebbe essere utile valutare il power Doppler in tutti i pazienti con uno spessore di parete intestinale maggiore di 5 mm: per i pazienti con un risultato positivo al power Doppler potrebbe essere indicata una terapia profilattica più aggressiva.


Similar content being viewed by others


References
Cammarota T, Ribaldone DG, Resegotti A, Repici A, Danese S, Fiorino G et al (2013) Role of bowel ultrasound as a predictor of surgical recurrence of Crohn’s disease. Scand J Gastroenterol 48:552–555
Bernstein C, Rawsthorne P, Cheang M, Blanchard JF (2006) A population-based case control study of potential risk factors for IBD. Am J Gastroenterol 101:993–1002
Esteban JM, Aleixandre A, Hurtado MJ, Maldonado L, Mora FJ, Nogues E (2003) Contrast-enhanced power Doppler ultrasound in the diagnosis and follow-up of inflammatory abdominal masses in Crohn’s disease. Eur J Gastroenterol Hepatol 15:253–259
Robotti D, Cammarota T, Debani P, Sarno A, Astegiano M (2004) Activity of Crohn disease: value of color-power-Doppler and contrast-enhanced ultrasonography. Abdom Imaging 29:648–652
Bolondi L, Gaiani S, Brignola C, Campieri M, Rigamonti A, Zironi G et al (1992) Changes in splanchnic hemodynamics in inflammatory bowel disease. Non-invasive assessment by Doppler ultrasound flowmetry. Scand J Gastroenterol 27:501–507
Parente F, Maconi G, Bollani S, Anderloni A, Sampietro G, Cristaldi M et al (2002) Bowel ultrasound in assessment of Crohn’s disease and detection of related small bowel strictures: a prospective comparative study versus X ray and intraoperative findings. Gut 50:490–495
Maconi G, Carsana L, Fociani P, Sampietro GM, Ardizzone S, Cristaldi M et al (2003) Small bowel stenosis in Crohn’s disease: clinical, biochemical and ultrasonographic evaluation of histological features. Aliment Pharmacol Ther 18:749–756
Mayer D, Reinshagen M, Mason RA, Muche R, von Tirpitz C, Eckelt D et al (2000) Sonographic measurement of thickened bowel wall segments as a quantitative parameter for activity in inflammatory bowel disease. Z Gastroenterol 38:295–300
Haber HP, Busch A, Ziebach R, Stern M (2000) Bowel wall thickness measured by ultrasound as a marker of Crohn’s disease activity in children. Lancet 355:1239–1240
Castiglione F, deSio I, Cozzolino A, Rispo A, Manguso F, Del Vecchio Blanco G (2004) Bowel wall thickness at abdominal ultrasound and the one-year-risk of surgery in patients with Crohn’s disease. Am J Gastroenterol 99:1977–1983
Maconi G, Parente F, Bollani S, Cesana B, Bianchi Porro G (1996) Abdominal ultrasound in the assessment of extent and activity of Crohn’s disease: clinical significance and implication of bowel wall thickening. Am J Gastroenterol 91:1604–1609
Best WR, Becktel JM, Singleton JW (1979) Rederived values of the eight coefficients of the Crohn’s disease activity index (CDAI). Gastroenterology 77:843–846
Conflict of interest
We have no conflict of interest.
Informed consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. All patients provided written informed consent to enrolment in the study and to the inclusion in this article of information that could potentially lead to their identification.
Human and animal studies
The study was conducted in accordance with all institutional and national guidelines for the care and use of laboratory animals.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ribaldone, D.G., Cammarota, T., Resegotti, A. et al. Power Doppler sonography to predict the risk of surgical recurrence of Crohn’s disease. J Ultrasound 18, 51–55 (2015). https://doi.org/10.1007/s40477-014-0101-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40477-014-0101-x