
Abstract
Purpose
We compared the effect of an educational pamphlet and a mobile application regarding prevention and emergency management of sport-related traumatic dental injuries (TDIs) on knowledge and self-reported preventive practice of 11–17-year-old Karate and Taekwondo athletes.
Methods
Participants were invited through an online link published by the Public Relations of the corresponding federations. They completed an anonymous questionnaire consisting of demographics, self-reported experience of TDIs, knowledge of emergency management of TDIs, self-reported preventive practice of TDIs, and the reason for not using mouthguard. The respondents were randomly allocated to pamphlet or mobile application group with the same content. Three months after the intervention, the questionnaire was completed by the athletes again. Repeated measures ANOVA and a linear regression model served for statistical analysis.
Results
In pamphlet group, 51 athletes and in mobile application group 57 athletes completed both baseline and follow-up questionnaires. At baseline, the mean score was 1.98 ± 1.20 and 1.82 ± 1.24 (out of 7) for the knowledge and 3.70 ± 1.64 and 3.33 ± 1.95 (out of 7) for practice in the pamphlet and application group, respectively. In 3-month follow-up, the mean score of knowledge and self-reported practice was significantly higher compared to baseline in both groups (p < 0.001) with no statistically significant difference between the two groups (p = 0.83 and p = 0.58, respectively). Most of the athletes were very satisfied or satisfied with both types of the educational intervention.
Conclusion
Both pamphlet and mobile application seem to be useful to improve awareness and practice regarding TDI prevention in adolescent athletes.
Similar content being viewed by others

Background
Traumatic dental injuries (TDIs) are considered as a public health problem due to their frequency, cost, and impact on quality of life (Andersson 2013; Lam 2016; American Academy of Pediatric Dentistry [AAPD] 2018). These injuries are more common in certain groups affecting nearly one-quarter of adolescents and adults at least once during their life (Glendor 2008; Lam 2016). Moreover, lifestyle habits and behaviors increase the risk of TDIs (Andersson 2013; Lam 2016). All sports are associated with a risk of orofacial injuries as 20–30% of all TDIs are caused by sport incidents at ages above 7 years old (Tuna and Ozel 2014; AAPD 2018; Knapik et al. 2019). TDIs frequently occur in young athletes and in contact sports; therefore, these groups are important in TDIs etiology (Ferrari and De Medeiros 2002; Azami-Aghdash et al. 2015).
Martial arts, especially in contact forms, are among sports that carry the highest risk of dental trauma (Young et al. 2015). A systematic review on the prevalence of dentofacial injuries among combat sports practitioners concluded that a quarter of combat sports athletes experience at least one of these injuries (Polmann et al. 2020). The popularity of martial arts among the young generation puts them at a higher risk of orofacial injuries including TDIs (Shirani et al. 2010). Taekwondo and Karate are two popular martial arts in adolescents (Ziaee et al. 2010, 2015): According to the statistics of Tehran (the capital city) Municipality in 2015, around 16,500 men and 7500 women athletes have officially been engaged in Taekwondo, putting this sport in the fifth popularity rank among all sports. The corresponding figures for male and female Karate athletes have been 11,000 and 7000, respectively, according to the same statistics (http://amarista.ir/content/statistics/1022/). These sports are more concerning regarding the occurrence of orofacial injuries due to their aggressive offensive/defensive nature, which necessitates striking and blocking various parts of the body and the face with techniques along with maximum force and minimum safety equipment (Shirani et al. 2010).
Most of the TDIs in sports are easily preventable through using mouthguards (Ferrari and De Medeiros 2002; AAPD 2018). Protective equipment such as helmets, facemasks, and mouthguards have been successfully used to prevent or reduce the frequency and severity of sport-related TDIs (Tulunoglu and Özbek 2006; AAPD 2018). However, despite all proven advantages of preventive equipment such as mouthguards, many athletes have a poor compliance since their use is not mandatory in some sports, or due to their negative attitude regarding the interference of the mouthguard with how the game is played or the athlete’s function, esthetics, and enjoyment (Tulunoglu and Özbek 2006; AAPD 2018).
If a TDI occurs, a better prognosis rate is closely related to the correct management of the traumatized tooth at the site of the accident immediately after the dental trauma (Nagata et al. 2018). The dental profession is responsible for providing public education on the risk of sports-related TDIs and available preventive strategies (Bourguignon and Sigurdsson 2009; Levin and Zadik 2012; AAPD 2018). The best strategy for prevention of TDIs is to receive education on both primary prevention and secondary prevention in the form of prompt management in case of occurrence (Bourguignon and Sigurdsson 2009; Levin and Zadik 2012; Sigurdsson 2013). Children and adolescents and those in the vicinity, including coaches and parents, should receive education (Levin and Zadik 2012; Sigurdsson 2013). This education should be provided for both genders equally (Bourguignon and Sigurdsson 2009). Different forms of educational resources including posters, pamphlets, videos, websites, social media, and mobile healthcare applications are available (Iskander et al. 2016). Educational pamphlet as printed media is an effective and low-cost resource for providing information on different levels of dental trauma prevention (Arikan and Sönmez 2012). Besides, mobile applications are an accessible tool to inform people about best management practices at virtually any place, including at the scene of an accident (Iskander et al. 2016). According to last formal report of the Statistical Center of Iran in 2017, 29.7% of children under 15 years and 89.6% of Iranian aged 15–24 have a cell phone (Statistical Center of Iran 2021).
Studies have shown the lack of information and knowledge regarding dental trauma emergency care in different groups of athletes (Emerich et al. 2013). In fact, current evidences suggest that sports persons and coaches globally have poor knowledge on prevention and emergency management of TDI (Tewari et al. 2021). The same stuation exists reagrding compliance in mouthguard use (Tulunoglu and Özbek 2006; AAPD 2018), while considerable body of evidence is available on the effectiveness of wearing mouthguard on prevention of dentoalveolar injuries among athletes (Fernandes et al. 2019). To date, limited information is available regarding the comparative effect of different educational media on prevention of TDIs in sports. This study was conducted to compare the effects of an educational pamphlet and a mobile application regarding prevention and emergency management of sport-related TDIs on knowledge and self-reported preventive practice of 11–17-year-old Karate and Taekwondo athletes.
Methods
Study design and subjects
The subjects of this interventional study included male and female adolescent Karate and Taekwondo athletes aged 11–17 years old. Frequent occurrence of TDIs in adolescent athletes in contact sports underlines the importance of TDI prevention in this group (Ferrari and De Medeiros 2002; Azami-Aghdash et al. 2015). Among sports, martial arts consist of a variety of formal traditions both in the noncombat form with a lower risk of injury and in the combat form with increased risk of injury (Koutures and Demorest 2018).
According to the Iran Federation of Sports Medicine, female athletes are professionally engaged in three types of martial arts including Karate, Taekwondo and Wushu. Karate and Taekwondo athletes were selected as the study population since a larger number of female athletes practice in these two federations. The inclusion criteria were male or female gender, age 11–17 years old, having a cellphone, and being a member of the official social network of Taekwondo or Karate Federation. The only exclusion criterion was reluctance to participate in the study.
Considering the shutdown of sports clubs due to the COVID-19 pandemic, the Public Relations of Karate and Taekwondo federations called upon athletes to participate in the study by publishing an online link in their social networks (WhatsApp Inc., Mountain View, California, USA), each having more than 5000 members. The link included an online questionnaire prepared in Google Docs (Google Inc., Googleplex, Mountain View, California, USA) and was forwarded to athletes on a daily basis for a week from 8 to 15 September 2020. Two reminders were sent in the social networks during this period. To increase the motivation of the athletes, they were informed that they would receive a reward (cash gift to five participants in each intervention group by lottery) if they participate in the study. The sampling continued till the sufficient sample size for the descriptive part of the study, 295 individuals, was achieved (Esmaeilpoor et al. 2021). All participants then randomly were assigned to the two groups of the interventional part of the study.
Sample size calculation
A minimum sample size of 79 was calculated using multiple regression power analysis tab of PASS II considering α = 0.05, β = 0.2 and R2 = 0.15.
Data collection
This interventional study was performed in three phases. At baseline, volunteer athletes joined the study via an online link and fulfilled an online self-administrated questionnaire. The athletes were asked to write their cellphone number in the questionnaire to make sure that they could be accessed during the research process. In the second phase, one of the researchers (SR) assigned the athletes to two intervention groups of educational pamphlet and mobile application through simple randomization by random-number-generating function of Microsoft Excel version 2016. To have similar numbers of the two genders in the two groups, random assignment was done separately for girls and boys. In the third phase, the same questionnaire was completed by the athletes 3 months after the intervention. The answers were then scored and the data were statistically analyzed to compare the pre- and post-test results. Both intervention groups received a reminder 45 days after the intervention, which was the same pamphlet in the pamphlet group and a notification in the mobile application group.
Interventions
The educational intervention included a pamphlet and a mobile application with a similar content based on the latest evidence and scientific guidelines (AAPD 2018; Bourguignon et al. 2020; Fouad et al. 2020). Both the educational pamphlet and the mobile application contained information in two parts: 1. the importance of TDI prevention including the preventive role of mouthguards and different types of this appliance, and 2. proper emergency management of TDIs including soft tissue damage, crown fracture, tooth luxation, tooth avulsion, and alveolar bone damage. The educational material was prepared in the native language (Farsi) and included colorful pictures. Due to the shutdown of sports clubs during the COVID-19 pandemic, an electronic version of the educational pamphlet was prepared, which was sent to the athletes’ cellphones. Additionally, the final version of the mobile application was shared through Myket, the Iranian application market, by sending its link (https://myket.ir/app/ir.health.teeth) to the participants in the application group (see Appendix 1 for some photos of the pamphlet as well as some screenshots of the application).
Both interventional groups received one reminder 45 days after the intervention, which was the same pamphlet in the pamphlet group and a notification in the mobile application group.
Due to the nature of the interventions, it was impossible to have participants and researcher blinding. However, the statistical analyst was blind to the groups.
Questionnaire
The athletes were asked to fulfill an anonymous self-administrated valid and reliable questionnaire (Esmaeilpoor et al. 2021) before and 3 months after the interventions. They were asked to write a unique code at the beginning of the first and second questionnaires, which was used to assess individual changes throughout the study. In addition to demographics (age, gender, years of practice, number and duration of training sessions per week, and previous training on prevention and management of orofacial injury) the questionnaire included the following parts:
-
Self-reported experience of TDIs: a “yes/no” question.
-
Knowledge of emergency management of TDIs: seven questions with multiple-choice as well as “yes, no, and I do not know” answers. A score of 0 was given to false or “I do not know” answers and a score of 1 was assigned to correct answers. The knowledge score of each athlete was calculated by summing up the scores of seven questions (range: 0 to 7).
-
Self-reported preventive practice: five questions on the use of protective gear (mouthguard and helmet) using multiple-choice as well as “yes, no, and I do not know” answers. Unfavorable and “I do not know” answers scored 0 and favorable answers scored 1. One question on the type of mouthguard had a weighted score based on the answer (custom-made = 3, mouth-formed = 2, stock = 1, not using = 0). The self-reported preventive practice score of each athlete was calculated through summing up the scores of five questions (range: 0 to 7).
-
One question on the reason for not using a mouthguard: a multiple-choice question.
-
Satisfaction: four questions on satisfaction with the educational material simplicity and comprehensibility, attractiveness, impact on the use of mouthguard, and general opinion about educational content on a 5-point Likert scale from “not at all satisfied” (score 1) to “extremely satisfied” (score 5). The participants were asked to complete the questionnaire once more after 3 months.
Ethical considerations
This study is registered in Iranian Registry of Clinical Trials, IRCT20130617013695N4, and was approved by the Ethics Committee of Tehran University of Medical Sciences (IR.TUMS.DENTISTRY.REC.1399.016). This interventional study was completely voluntary and the responses were anonymous. Moreover, all respondents were free to leave the study in each phase. In the beginning of the study, all participants were informed about the objectives of the study and those who were willing to participate in the study completed the questionnaire. Informed consent was obtained from the participants and their parents via a link sent to their parents’ cellphones.
Statistical analysis
The data were analyzed using the SPSS software version 22.0 (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp). A linear regression model (backward method) was used for multivariate assessment. Age, gender, years of practice, number and duration of training sessions per week, and previous training on prevention and management of orofacial injury were entered in the model as covariates. Repeated measures ANOVA was applied for statistical analysis. In this test, knowledge and self-reported practice before and after the intervention were considered as repeated factors and the type of intervention was considered a between-subject factor. P values less than 0.05 were considered significant.
Results
In September 2020, a total of 295 participants completed the baseline questionnaire. Then, they were randomly divided to two groups, including pamphlets (n = 143) and mobile application (n = 152). In total, 108 participants completed the follow-up questionnaire (January 2021), including 51 in the pamphlet group and 57 in the mobile application group. There were some participants discontinued the study prior to post-testing due to the online nature of the study and personal reasons. The flowchart of sampling has been included as Supplementary file 1.
Demographics
The mean age of the study population was 14.37 ± 1.84 years. The mean age of the subjects was 14.83 ± 1.89 years in the pamphlet and 13.62 ± 1.66 years in application group. Moreover, 68.6% (n = 35) of the participants in the pamphlet group and 70.2% (n = 40) of the subjects in the application group were females. In addition, 52.9% (n = 27) of the subjects in the pamphlet group and 87.7% (n = 50) of the subjects in the application group were Taekwondo players. Table 1 shows more details on baseline characteristics of participants.
As for the TDI, 55.5% (n = 60) of the subjects including 62.7% (n = 32) in the pamphlet and 49.1% (n = 28) in the application group had a positive history of orofacial injury.
Knowledge scores before and after the intervention
Table 2 shows the distribution of the athletes’ answers to knowledge questions regarding TDIs before and after the interventions. Before the intervention, the mean knowledge score of the athletes was 1.98 ± 1.20 and 1.82 ± 1.24 (out of 7) in the pamphlet and application group, respectively. In 3-month follow-up, the mean knowledge score increased to 4.39 ± 2.05 in the pamphlet and to 4.14 ± 2.23 in the application group. The mean knowledge score increased significantly in both groups compared to the baseline (p < 0.001 in both groups). There was no statistically significant difference in the mean knowledge score between the two groups in the 3-month follow-up (p = 0.83).
None of demographic characteristics had a significant relationship with the baseline knowledge score except for hours of training per week (β = 0.24, p = 0.01). Moreover, no significant relationship was observed between the difference in the knowledge score and demographic characteristics.
Self-reported practice score before and after the intervention
Table 3 shows the distribution of the athletes’ answers to self-reported practice questions regarding TDIs before and after the interventions. Before the intervention, the mean score of the self-reported practice was 3.70 ± 1.64 and 3.33 ± 1.95 (out of 7) in the pamphlet and application group, respectively. In the 3-month follow-up, the mean score of self-reported practice increased to 4.50 ± 1.34 in the pamphlet and 4.35 ± 1.48 in the application group. The mean score of self-reported practice increased significantly in both groups compared to the baseline (p < 0.001 in both groups). No significant difference was observed in the mean score of self-reported practice between the two groups in the 3-month follow-up (p = 0.58).
There was a significant relationship between baseline self-reported practice score and age (β = 0.29, p = 0.002) and years of practice (β = 0.24, p = 0.01). Among demographic variables, only age had a significant relationship with the difference in the self-reported practice score (β = − 0.32, p = 0.001).
The Pearson correlation coefficient showed a significant correlation between knowledge and self-reported preventive practice in the 3-month follow-up (r = 0.22, p = 0.03).
Reasons for not using mouthguard
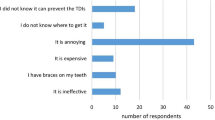
The most common reason for not using mouthguards indicated was an annoying feeling reported by 15.7% of all respondents (Fig. 1).

Reasons for not using the mouthguard stated by athletes in intervention groups (pamphlet group: n = 23; application group: n = 14)
Athletes’ satisfaction on educational pamphlet and mobile application
Regarding the participants’ satisfaction in the 3-month follow-up, the percentage of the participants who selected Likert scores 5 and 4 (very satisfied and satisfied, respectively) for all items regarding educational materials including simplicity and comprehensibility, attractiveness, impact on the mouthguard use, and general opinion about the educational content was above 70% for both interventions, except for attractiveness of mobile application which was about 63%. The item with the highest satisfaction was general opinion about educational content, which was selected by 91.2% and 100% in the pamphlet and mobile application group, respectively, indicating very satisfied and satisfied.
Discussion
This study was conducted to compare the effects of an educational pamphlet and a mobile application regarding prevention and emergency management of sport-related TDIs on knowledge and self-reported preventive practice of 11–17-year-old Karate and Taekwondo athletes. The results showed no significant difference in knowledge and self-reported preventive practice after 3-month follow-up between the two intervention groups. Improvement of the scores of knowledge and self-reported preventive practice in both groups indicated the effectiveness of both interventions.
This was the first study of the effect of educational intervention on TDIs among adolescent athletes in Iran. Another advantage of this study was the presence of a high number of female adolescent athletes. The target group was high-risk individuals for TDIs practicing two popular martial arts, Karate and Taekwondo, as contact sports, which are popular among Iranian adolescents. A meta-analysis has reported the pooled prevalence of dentofacial injuries for Karate and Taekwondo to be 43.5% (95% CI 30.0–57.5%) and 37.5% (95% CI 20.8–56.0%), respectively (Polmann et al. 2020). Moreover, adolescent athletes aged 11–17 years old from both genders were selected and randomly divided into two groups (pamphlet and application) considering demographic similarities. However, this study had some limitations. Due to COVID-19 pandemic, all contact sports clubs were closed in Iran at the time of data collection, which led to some problems regarding the distribution of questionnaires and educational pamphlets. We instead prepared the electronic version of educational pamphlet, which was sent to the athletes’ cellphones. Moreover, to overcome this problem, these steps were coordinated with the authorities of the Taekwondo and Karate federations. Furthermore, rewards were used to increase the participation of athletes in the study. While the results might not be generalizable to all athlete populations or other combat sports, the finings seem to have some implication for training adolescent athletes engaged in martial arts.
The data gathering tool was a valid and reliable questionnaire. The questionnaire was anonymous and contained a code in order to match baseline and follow-up questionnaires. The athletes were requested to report the mouthguard use status and previous experience of TDIs; however, like all questionnaire-based studies, recall bias and social desirability were expected (Knapik et al. 2019). Thus, the findings might be an optimistic estimation of the real situation, and the results should be interpreted cautiously. Moreover, some athletes might have started to use mouthguard after a TDI, which was not taken into account by the questionnaire.
The athletes’ baseline knowledge in both intervention groups was far from the maximum obtainable score, indicating the lack of sufficient knowledge regarding TDIs in target group, which was consistent with the results of previous studies by Al-Musawi et al. (2017), Rouhani et al. (2015), Sepet et al. (2014), Al-Afraj et al. (2016) and Mojarad et al. (2020). A global lack of sufficient knowledge on prevention and early management of TDIs can be seen among athletes and coaches in all sports (Tewari et al. 2021). These findings indicate the need for athletes’ knowledge improvement regarding TDIs.
The prognosis of TDI treatment, especially in case of tooth avulsion as a dental emergency, depends not only on the dentist’s expertise, but also on the knowledge of proper immediate management at the site of injury (Levin and Zadik 2012; Collins et al. 2016). Therefore, it is necessary that coaches and athletes have the basic knowledge for emergency management of sport-related TDIs (Glendor 2008; Levin and Zadik 2012). It has been suggested that coaches, physical education teachers, sports students, and athletes should receive trainings on the subject either formally or through campaigns with posters and/or audio–visual media (Tewari et al. 2021), similar to what we produced and tested in the present study.
In the present study, the knowledge level of the athletes was generally low, especially on dental avulsion management in different aspects such as possibility of replantation, the critical replantation time and the best store medium until replantation. These findings were similar to other previous studies indicating the athletes’ lack of knowledge, especially on management of tooth avulsion (Sepet et al. 2014; Rouhani et al. 2015; Kroon et al. 2016; Galic et al. 2018). In the present study, a small number of athletes knew the proper first aid and emergency procedures of dental avulsion, as a dental emergency, indicating insufficient knowledge in this regard, which was consistent with the findings of a study conducted by Al-Afraj et al. (2016). Other studies also found similar results; for instance, Sepet et al. (2014) found that only a quarter of sport participants kept the avulsed tooth in saline solution. Moreover, Vidovic et al. (2015) found that only 44% of athletes were aware of possibility of replanting the avulsed tooth. Aljohani et al. (2017) reported that only 12% of Taekwondo athletes were aware of the possibility of an avulsed tooth replantation and 25% had the knowledge of maximum time for an avulsed tooth for replantation.
All of these findings support that all participants involved in sports with the risk of sport-related TDIs are more likely to protect themselves from orofacial injuries only through education and increased awareness on prevention and proper management of TDIs, which would facilitate informed decision making on mouthguard use (Kroon et al. 2016).
The self-reported TDI preventive practice score of the athletes in both groups was insufficient, indicating the need for improvement. However, 71.5% of the participants used mouthguards during training and matches. This figure was higher than findings of similar studies in south Korea (56%) (Lee et al. 2013) and Saudi-Arabia (56%) (Al-Arfaj et al. 2016); however, it is lower than the result of a study by Vidovic et al. in Croatia (96%) (2015).
Galic et al. (2018) found that even though most of the athletes acknowledged the importance of mouthguard use for prevention of TDIs, only 41% of them actually used it. Sepet et al. (2014) reported that whilst 55.4% of sport participants were aware of the protective effect of mouthguards, only 11.2% reported routine mouthguard. It seems that sport rules, coaches and athletes’ perception regarding mouthguard use as well as the discomfort of wearing a mouthguard affect the use of this protective gear. The specific and cultural features of each sport also play a role in the adherence to the use of the mouthguard (Fernandes et al. 2019). Moreover, since practice is influenced by the level of knowledge, any deficiency in the athletes’ practice can be a reflection of lack of knowledge. These findings highlight the need for educational programs on the role of mouthguard use in prevention of TDIs for athletes. In addition, the sports committees should regulate mandatory use of mouthguard as a protective equipment, since TDIs endanger not only the athletes’ health and physical integrity, but also their sports performance (Fernandes et al. 2019).
In the present study, the most common reason for not wearing a mouthguard was its discomfort, which was similar to findings of previous studies (Lee et al. 2013; Sepet et al. 2014; Vidovic et al. 2015; Aljohani et al. 2017). This might be due to the type of the mouthguard used by athletes; of all participants who reported mouthguard use, only 7.4% used custom-made mouthguards, 35.8% used mouth-formed mouthguards, and 56.8% used stock mouthguards. These results are comparable with the findings of studies by Vidovic et al. (2015), Biagi et al. (2010), and Emerich et al. (2013), in which the athletes indicated that mouthguards might cause speech problems, breathing difficulties, and jaw and muscle pain, or might be distorted or fall out during the sport activity. These problems are less common in custom-made mouthguards as they properly match with teeth and gingival tissue; however, this type of mouthguards is relatively more expensive than other types (Galic et al. 2018). Nonetheless, considering the cost and complexity of TDI treatment, AAPD recommends mandating the use of custom-made mouthguards in sporting activities that carry a risk of orofacial injury (AAPD 2018).
The present study found that using a pamphlet and mobile application had similar results in improving knowledge and preventive practice regarding TDIs among athletes. Various interventional methods have been used to improve knowledge and preventive practice. For instance, Al-Musawi et al. (2017) compared the effects of lecture, lecture/smartphone application, and smartphone application on the knowledge level of three groups of elementary teachers regarding tooth avulsion and showed that using application alone was an effective tool for laypeople to obtain knowledge on management of tooth avulsion. Arikan and Sönmez (2012) found an improvement in the knowledge of primary school teachers after using an educational leaflet on emergency management of TDIs. ElBardissy (2019) reported that a smartphone application on emergency management of different TDIs was an effective means for providing accessible knowledge for dental students. de Castro Berry et al. (2017) developed a mobile application about trauma in primary dentition for dental professionals that provided them with quick access to and safe information about this topic.
Liew et al. (2020) found that an educational workshop was effective in improving knowledge on dental trauma among rugby players. Emerich et al. (2013) showed that an educational lecture and a subsequent educational session on dental trauma significantly improved the knowledge level of sport university students.
Educational pamphlets are a fast and inexpensive tool for providing information on a special subject for a large number of people (Arikan and Sönmez 2012). Moreover, the availability of pamphlets facilitates the access to the educational content. Nowadays, smartphone applications are an integral part of the learning process and contribute significantly to a new way of educating in health (ElBardissy 2019). Providing quick information as well as optimizing navigation and time increase the effectiveness of applications in short- and long-term learning (de Castro Berry et al. 2017). Depending on the audience, their skills and financial level, pamphlets and mobile applications can be selected and used for educational purposes.
In the present study, the older the athletes, the smaller the change in the self-reported practice scores. This may be related to more experience of older athletes on sport-related TDIs resulting in higher self-reported practice scores at baseline that were less influenced by the interventions.
Conclusions
Educational interventions regarding prevention and emergency management of TDIs using the pamphlet and mobile application were effective in improving knowledge and self-reported preventive practice of adolescent athletes in the 3-month follow-up. Focusing on high-risk groups such as young athletes may be valuable since behavioral change will likely benefit them most.
Data availability
The datasets used during the current study are available from the corresponding author upon reasonable request.
References
Al-Arfaj I, Al-Shammari A, Al-Subai T, Al-Absi G, AlJaffari M, Al-Kadi A, El Tantawi M, Al-Ansari A. The knowledge, attitude and practices of male sports participants to sports-related dental trauma in Khobar and Dammam, Saudi Arabia—A pilot survey. Saudi Dent J. 2016;28(3):136–41. https://doi.org/10.1016/j.sdentj.2016.02.001.
Aljohani YR, Alfaifi KH, Redwan SK, Sabbahi DA, Zahran MH. Dental injuries in taekwondo athletes practicing in Saudi Arabia. Saudi Med J. 2017;38(11):1143–7. https://doi.org/10.15537/smj.2017.11.21111.
Al-Musawi A, Al-Sane M, Andersson L. Smartphone App as an aid in the emergency management of avulsed teeth. Dent Traumatol. 2017;33(1):13–8. https://doi.org/10.1111/edt.12298.
American Academy of Pediatric Dentistry. Policy on prevention of sports-related orofacial injuries. 2018. https://www.aapd.org/media/policies_guidelines/p_sports.pdf. Accessed 20 Nov 2021.
Andersson L. Epidemiology of traumatic dental injuries. J Endod. 2013;39(3 Suppl):S2-5. https://doi.org/10.1016/j.joen.2012.11.021.
Arikan V, Sönmez H. Knowledge level of primary school teachers regarding traumatic dental injuries and their emergency management before and after receiving an informative leaflet. Dent Traumatol. 2012;28(2):101–7. https://doi.org/10.1111/j.1600-9657.2011.01042.x.
Azami-Aghdash S, Ebadifard Azar F, Pournaghi Azar F, Rezapour A, Moradi-Joo M, Moosavi A, Ghertasi OS. Prevalence, etiology, and types of dental trauma in children and adolescents: systematic review and meta-analysis. Med J Islam Repub Iran. 2015;29(4):234.
Berry M, Souza MI, Campos V, Oliveira AE, Carvalho P, Tomé Y. ClickTrauma: An App About Dental Trauma in Primary Dentition. JISfTeH. 2017. https://journals.ukzn.ac.za/index.php/JISfTeH/article/view/252\. Accessed 4 Oct 2022.
Biagi R, Cardarelli F, Butti AC, Salvato A. Sports-related dental injuries: knowledge of first aid and mouthguard use in a sample of Italian children and youngsters. Eur J Paediatr Dent. 2010;11(2):66–70.
Bourguignon C, Sigurdsson A. Preventive strategies for traumatic dental injuries. Dent Clin North Am. 2009;53(4):729–49. https://doi.org/10.1016/j.cden.2009.06.002.
Bourguignon C, Cohenca N, Lauridsen E, Flores MT, O’Connell AC, Day PF, Tsilingaridis G, Abbott PV, Fouad AF, Hicks L, Andreasen JO, Cehreli ZC, Harlamb S, Kahler B, Oginni A, Semper M, Levin L. International association of dental traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and Luxations. Dent Traumatol. 2020;36(4):314–30. https://doi.org/10.1111/edt.12578.
Collins CL, McKenzie LB, Ferketich AK, Andridge R, Xiang H, Comstock RD. Dental injuries sustained by high school athletes in the United States, from 2008/2009 through 2013/2014 academic years. Dent Traumatol. 2016;32(2):121–7. https://doi.org/10.1111/edt.12228.
ElBardissy A. Dental trauma: assessment of undergraduate dental students: theoretical knowledge and practical use of smartphone application ‘injured tooth.’ Egypt Dent J. 2019;65(4):3079–92. https://doi.org/10.21608/edj.2019.73986.
Emerich K, Wlodarczyk P, Ziolkowski A. Education of Sport University students regarding first-aid procedures after dental trauma. Eur J Paediatr Dent. 2013;14(1):37–41.
Esmaeilpoor A, Mohebbi SZ, Moghadam N, Ahmadian M, Razeghi S, Khami MR. Self-reported experience of orofacial injury, preventive practice, and knowledge of Iranian adolescent martial art athletes towards sports-related orofacial injuries. BMC Sports Sci Med Rehabil. 2021;13(1):134. https://doi.org/10.1186/s13102-021-00363-4.
Fernandes LM, Neto JCL, Lima TFR, Magno MB, Santiago BM, Cavalcanti YW, de Almeida LFD. The use of mouthguards and prevalence of dento-alveolar trauma among athletes: a systematic review and meta-analysis. Dent Traumatol. 2019;35(1):54–72.
Ferrari CH, de FerreriaMederios JM. Dental trauma and level of information: mouthguard use in different contact sports. Dent Traumatol. 2002;18(3):144–7. https://doi.org/10.1034/j.1600-9657.2002.00017.x.
Fouad AF, Abbott PV, Tsilingaridis G, Cohenca N, Lauridsen E, Bourguignon C, O’Connell A, Flores MT, Day PF, Hicks L, Andreasen JO, Cehreli ZC, Harlamb S, Kahler B, Oginni A, Semper M, Levin L. International association of dental traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of Permanent Teeth. Dent Traumatol. 2020;36(4):331–42. https://doi.org/10.1111/edt.12573.
Galic T, Kuncic D, PoklepovicPericic T, Galic I, Mihanovic F, Bozic J, Herceg M. Knowledge and attitudes about sports-related dental injuries and mouthguard use in young athletes in four different contact sports-water polo, karate, taekwondo and handball. Dent Traumatol. 2018;34(3):175–81. https://doi.org/10.1111/edt.12394.
Glendor U. Epidemiology of traumatic dental injuries—a 12 year review of the literature. Dent Traumatol. 2008;24(6):603–11. https://doi.org/10.1111/j.1600-9657.2008.00696.x.
Iskander M, Lou J, Wells M, Scarbecz M. A poster and a mobile healthcare application as information tools for dental trauma management. Dent Traumatol. 2016;32(6):457–63. https://doi.org/10.1111/edt.12278.
Knapik JJ, Hoedebecke BL, Rogers GG, Sharp MA, Marshall SW. Effectiveness of mouthguards for the prevention of orofacial injuries and concussions in sports: systematic review and meta-analysis. Sports Med. 2019;49(8):1217–32. https://doi.org/10.1007/s40279-019-01121-w.
Koutures C, Demorest RA. Participation and injury in martial arts. Curr Sports Med Rep. 2018;17(12):433–8. https://doi.org/10.1249/JSR.0000000000000539.
Kroon J, Cox JA, Knight JE, Nevins PN, Kong WW. Mouthguard use and awareness of junior rugby league players in the Gold Coast, Australia: a need for more education. Clin J Sport Med. 2016;26(2):128–32. https://doi.org/10.1097/JSM.0000000000000206.
Lam R. Epidemiology and outcomes of traumatic dental injuries: a review of the literature. Aust Dent J. 2016;61(Suppl 1):4–20. https://doi.org/10.1111/adj.12395.
Lee JW, Heo CK, Kim SJ, Kim GT, Lee DW. Mouthguard use in Korean Taekwondo athletes—awareness and attitude. J Adv Prosthodont. 2013;5(2):147–52. https://doi.org/10.4047/jap.2013.5.2.147.
Levin L, Zadik Y. Education on and prevention of dental trauma: it’s time to act! Dent Traumatol. 2012;28(1):49–54. https://doi.org/10.1111/j.1600-9657.2011.01060.x.
Liew A, Abdullah D, Lokeman MA, Kamaruddin MAF, Zainal MKM, Soo E. Effectiveness of an educational workshop in improving knowledge on dental trauma among rugby players. J Int Dent Medical Res. 2020;13:337–45.
Mojarad F, Farhadian M, Torkaman S. The prevalence of sports-related dental injuries and the rate of awareness of mouthguard use among child athletes. J Pediatr Res. 2020;7:358–64.
Nagata JY, Góis VLA, Münchow EA, Albuquerque MTP. Dental trauma education intervention as a positive influence among undergraduate students. Eur J Dent. 2018;12(4):502–7. https://doi.org/10.4103/ejd.ejd_148_18.
Polmann H, Melo G, Conti Réus J, Domingos FL, de Souza BDM, Padilha AC, Duque TM, Porporatti AL, Flores-Mir C, De Luca CG. Prevalence of dentofacial injuries among combat sports practitioners: a systematic review and meta-analysis. Dent Traumatol. 2020;36(2):124–40.
Rouhani A, Akbari M, Ghoddusi J, Rahmandust MR. Knowledge of sportsmen and coaches about dental trauma in 2011 in Mashhad. J Isfahan Dent Sch. 2015;11(3):239–47.
Sepet E, Aren G, DoganOnur O, Pinar Erdem A, Kuru S, Tolgay CG, Unal S. Knowledge of sports participants about dental emergency procedures and the use of mouthguards. Dent Traumatol. 2014;30(5):391–5. https://doi.org/10.1111/edt.12105.
Shirani G, KalantarMotamedi MH, Ashuri A, Eshkevari PS. Prevalence and patterns of combat sport related maxillofacial injuries. J Emerg Trauma Shock. 2010;3(4):314–7. https://doi.org/10.4103/0974-2700.70744.
Sigurdsson A. Evidence-based review of prevention of dental injuries. Pediatr Dent. 2013;35(2):184–90.
Statistical Center of Iran. Households and people using mobile phones 2017. 2021. https://www.amar.org.ir/Portals/0/amarmozuii/infographics/Presentation3-Mobile%20-%20980703.pdf. Accessed 20 Nov 2021.
Tewari N, Johnson RM, Mathur VP, Rahul M, Goel S, Ritwik P, Bansal K, Atif M. Global status of knowledge for prevention and emergency management of traumatic dental injuries in sports persons and coaches: a systematic review. Dent Traumatol. 2021;37(2):196–207.
Tulunoglu I, Ozbek M. Oral trauma, mouthguard awareness, and use in two contact sports in Turkey. Dent Traumatol. 2006;22(5):242–6. https://doi.org/10.1111/j.1600-9657.2006.00386.x.
Tuna EB, Ozel E. Factors affecting sports-related orofacial injuries and the importance of mouthguards. Sports Med. 2014;44(6):777–83. https://doi.org/10.1007/s40279-014-0167-9.
Vidovic D, Bursac D, Skrinjaric T, Glavina D, Gorseta K. Prevalence and prevention of dental injuries in young taekwondo athletes in Croatia. Eur J Paediatr Dent. 2015;16(2):107–10.
Young EJ, Macias CR, Stephens L. Common dental injury management in athletes. Sports Health. 2015;7(3):250–5. https://doi.org/10.1177/1941738113486077.
Ziaee V, Rahmani SH, Rostami M. Injury rates in Iranian taekwondo athletes; a prospective study. Asian J Sports Med. 2010;1(1):23–8. https://doi.org/10.5812/asjsm.34877.
Ziaee V, Shobbar M, Lotfian S, Ahmadinejad M. Sport injuries of karate during training: an epidemiologic study in Iran. Asian J Sports Med. 2015;6(2): e26832. https://doi.org/10.5812/asjsm.26832.
Acknowledgements
This study was funded and supported by Tehran University of Medical Sciences (TUMS); Grant no. 99.2.133.48370. We also thank Dr. Mohammad J. Kharazifard for his constructive contribution to data analysis of the study. We are highly thankful to the Department of Sports Medicine of Tehran University of Medical Sciences, Iran Sports Medicine Federation, Iran Karate Federation, and Iran Taekwondo Federation for helping and supporting us in this study. We would like to thank Dr. Farhad Moradi Shahpar, Dr. Laleh Hakemi, Dr. Mohammadebrahim Marjani, Farahnaz Arbab, Hossein Parsi, and Hasan Shokrian for assisting us in collecting data.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This study is registered in Iranian Registry of Clinical Trials, IRCT20130617013695N4; “retrospectively registered” at 04-22-2022.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Azizzadeh, A., Mohebbi, S.Z., Esmaeilpoor, A. et al. Impacts of educational interventions on the knowledge of prevention and emergency management of traumatic dental injuries in 11–17-year-old martial arts athletes: a randomized controlled trial. Eur Arch Paediatr Dent 24, 263–272 (2023). https://doi.org/10.1007/s40368-023-00790-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40368-023-00790-6