
Abstract
Introduction
Divergent objectives and narratives among members of a healthcare team may lead to suffering, underscoring the need to align patient care with the patient’s self-identified priorities and goals. Shared decision making (SDM) with patients who may not be able to make healthcare decisions for themselves presents a unique challenge to healthcare providers, caregivers, and patients. Children and the elderly are two such groups where substituted decision making is often required. Family meetings, wherein stakeholders in a patient’s care are gathered, present opportunities to align expectations and clinical goals. There is a clear need for a technique exploring all facets of the patient’s story within the context of the biopsychosocial-spiritual model. We sought to promote narrative equity among stakeholders and maintain patient focus during family meetings. We describe the use of Mind Mapping in the family meeting to meet these objectives.
Methods
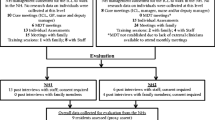
Using two clinical scenarios, one involving a geriatric patient and another involving a pediatric patient, we describe the stepwise development of Mind Maps and how their use informed discussions among stakeholders in the family meeting.
Results
Stakeholders found the Mind Maps easy to draw and helpful in eliciting their own priorities and preferences. Group exploration and refinement of the Mind Maps helped stakeholders to appreciate others’ sometimes divergent perspectives, to ensure that the patient’s voice was heard, and to ensure that care decisions were patient focused.
Discussion
Mind Mapping was easily performed in two clinical scenarios, allowing the patient, family, and medical team to explore the biopsychosocial-spiritual model extensively, to appreciate each stakeholder’s priorities, and to identify areas for further development. We have found that Mind Mapping helps define the ‘topography’ of relationships, prioritizes team discussions, finds shared interests in seemingly divergent objectives, and identifies which team member may best lead a discussion on a particular topic.
Conclusion
Mind Mapping may be a useful tool for family meetings, particularly for geriatric and pediatric patients with multiple stakeholders involved.
Plain Language Summary
Patient-focused healthcare, which prioritizes the needs and desires of the patient when creating a plan of care, relies on the patient’s voice being clearly and accurately heard. This is especially important when the patient cannot make medical decisions alone, as may be the case for elderly patients or children. Unfortunately, there are times when the patient’s voice may be ‘drowned out’ by family members, friends, or members of the healthcare team. Family meetings offer an opportunity for all parties involved in the patient’s care to gather together to ensure agreement on treatment goals and next steps. In this manuscript, we explore the technique of Mind Mapping as a tool to encourage all family meeting participants to speak and be heard. Using two clinical scenarios, one involving an elderly patient and the other a pediatric patient, we describe in a stepwise fashion how to perform Mind Mapping, what was done in these two cases, and how the Mind Maps changed how health care was delivered. We have found Mind Mapping effective in planning for family meetings, encouraging all persons involved in the patient’s care to share their perspectives, ensuring that the patient’s story is heard, and confirming that care plans reflect the patient’s desires and needs.




Similar content being viewed by others


References
Hudson P, Quinn K, O’Hanlon B, Aranda D. Family meetings in palliative care: multidisciplinary clinical practice guidelines. BMC Palliat Care. 2008;7:1–12.
Roberto KA, Blieszner R. Diverse family structures and the care of older persons. Can J Aging. 2015;34:305–20.
Uccelli MM. The impact of multiple sclerosis on family members: a review of the literature. Neurodegener Dis Manag. 2014;4:177–85.
Trettetieg S, Vatne S, Rokstad AMM. Meaning in family caregiving for people with dementia: a narrative study about relationships, values, and motivation, and how day care influences these factors. Multidiscip Healthc. 2017;10:445–55.
Miller AL, Miller SE, Clark KM. Child, caregiver, family, and social-contextual factors to consider when implementing parent-focused child feeding interventions. Curr Nutr Rep. 2018;7:303–9.
Zenlea IS, Thompson B, Fierheller D, et al. Walking in the shoes of caregivers of children with obesity: supporting caregivers in paediatric weight management. Clin Obes. 2017;7:300–6.
Coe NB, Skira MM, Larson EB. A comprehensive measure of the costs of caring for a parent: differences according to functional status. Am Geriatr Soc. 2018;66:2003–8.
Baile WF, Buckman R, Lenzi R, et al. SPIKES—a six-step protocol for delivering bad news: application to the patient with cancer. Oncologist. 2000;5:302–11.
www.achonline.org. Accessed March 6, 2020.
Sullivan L. Doctor offers patient communication PEARLS. Caring Ages. 2008;9:4.
Milan FB, Parish SJ, Reichgott MJ. A model for educational feedback based on clinical communication skills strategies: beyond the "feedback sandwich”. Teach Learn Med. 2006;18:42–7.
Ledford CJ, Canzona MR, Seehusen DA, et al. Differences in physician communication when patients ask versus tell about religion/spirituality: a pilot study. Fam Med. 2015;47:138–42.
Singer AE, Ash T, Ochotorena C, et al. A systematic review of family meeting tools in palliative and intensive care settings. Am J Hosp Palliat Care. 2016;33:797–806.
Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Int Med. 2012;27:1361–7.
Kahn J. See one, do one, teach one, but practice first. Palliat Med. 2016;19:675–6.
Buzan T, Buzan B. The mind map book: how to use radiant thinking to maximize your brain’s untapped potential. New York: Plume Books; 1993.
Pringle J. Health mind mapping has the potential to facilitate patient engagement in self-management of long-term conditions. Evid Based Nurs. 2019;22:23.
Petrie KJ, Weinman J. Patients' perceptions of their illness: The dynamo of volition in health care. Curr Direct Psychol Sci. 2012;21:60–5.
Broadbent E, Petrie KJ, Ellis CJ, et al. A picture of health—myocardial infarction patients' drawings of their hearts and subsequent disability. A longitudinal study. J Psychosom Res. 2004;57:583–7.
Brett-Maclean P. Body mapping: embodying the self living with HIV/AIDS. CMAJ. 2009;180:740–1.
Mollberg N, Surati M, Demchuk C, et al. Mind mapping for lung cancer: towards a personalized therapeutics approach. Adv Ther. 2011;28:173–94.
Buitron de la Vega P, Coe C, Paasche-Orlow MK, et al. “It’s like a mirror image of my illness”: exploring patient perceptions about illness using health mind mapping—a qualitative study. J Gen Intern Med 2018; 33:1692–9.
Engel GL. The clinical application of the biopsychosocial model. Am J Psychiatry. 1980;137:535–44.
Sulmasy DP. A biopsychosocial-spiritual model for the care of patients at the end of life. Gerontologist. 2002;42:24–33.
Kukulka K, Washington KT, Govindarajan R, Mehr DR. Stakeholder perspectives on the biopsychosocial and spiritual realities of living with ALS: implications for palliative care teams. Am J Hosp Palliat Care. 2019;26:851–7.
Edwards S, Cooper N. Mind mapping as a teaching resource. Clin Teach. 2010;7:236–9.
Chen AP, Chang AH, Hsu EB. Using mind mapping technology for personal preparedness planning. Am J Disaster Med. 2019;14:96–100.
D’Antoni AV, Zipp GP, Olson VG, Cahill TF. Does the mind map learning strategy facilitate information retrieval and critical thinking in medical students? MC Med Educ. 2010;10:61.
Burgess-Allen J, Owen SV. Using mind mapping techniques for rapid qualitative data analysis in public participation processes. Health Expect. 2010;13:406–15.
Nelson JE, Walker AS, Luhrs CM, et al. Family meetings made simpler: a toolkit for the ICU. J Crit Care 2009; 24:626e7–14.
Gay EB, Pronovost PJ, Bassett RD, Nelson JE. The intensive care unit family meeting: making it happen. J Crit Care 2009; 24:629e1–12.
Stapleton RD, Engelberg RA, Wenrich MD, et al. Clinician statements and family satisfaction with family conferences in the intensive care unit. Crit Care Med. 2006;34:1679–85.
Watson AC, October TW. Clinical nurse participation at family conferences in the pediatric intensive care unit. Am J Crit Care. 2016;25:489–97.
Schenker Y, Crowley-Matoka M, Dohan D, et al. I don’t want to be the one saying ‘we should just let him die’: intrapersonal tensions experienced by surrogate decision makers in the ICU. J Gen Intern Med. 2012;27:1657–65.
Fetherstonhaugh D, McAuliffe L, Bauer M, Shanley C. Decision-making on behalf of people living with dementia: how do surrogate decision-makers decide? J Med Ethics. 2017;43:35–40.
Batteux E, Ferguson E, Tunney RJ. On the likelihood of surrogates conforming to the substituted judgment standard when making end-of-life decisions for their partner. Med Decis Mak. 2019;39:651–60.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This project was not funded.
Conflict of interest
Dr Russell, Ms Carr, and Dr Kieran do not have any conflicts of interest relevant to this project.
Availability of data and material
All data generated or analyzed during this study are included in this published article (and its supplementary information files).
Author contributions
MLR: concept generation, data collection, manuscript writing and editing. AHC: concept generation, data collection, manuscript writing and editing. KK: data collection, manuscript writing and editing.
Additional information
Digital features
To view digital features for this article go to https://doi.org/10.6084/m9.figshare.12769868.
Rights and permissions
About this article

Cite this article
Russell, M.L., Carr, A.H. & Kieran, K. Using Mind Mapping in Family Meetings to Support Shared Decision Making with Pediatric and Geriatric Patients. Patient 13, 709–717 (2020). https://doi.org/10.1007/s40271-020-00447-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40271-020-00447-2