
Abstract
Objective
This study aimed to assess the correlation between body mass index (BMI) and plasma lipid profile levels in mild and severe COVID-19 patients.
Method
This was a prospective, observational, cohort study, conducted in a medical referral center specializing in management of COVID-19 cases. Patients were divided into two groups according to infection severity (mild and severe). Blood samples were obtained from all patients who tested positive to a PCR test for measuring biochemical and inflammatory markers such as lactate dehydrogenase, ferritin, C-reactive protein, and d-dimer, as well as lipid profile, including total cholesterol, triacylglycerols, low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C), which were analyzed and compared between the two groups. Pearson’s correlation was used to assess the correlation between BMI and plasma lipid profile among mild and severe cases.
Results
The levels of plasma triacylglycerols, d-dimer, lactate dehydrogenase, ferritin, and C-reactive protein with severe infection were significantly different between patients with mild and severe COVID-19 symptoms (p = 0.036, 0.03, 0.001, 0.014, and 0.006, respectively). A positive correlation between BMI and triglyceride levels was observed only in the severe infection group. However, HDL-C was negatively correlated with BMI.
Conclusion
A routine lipid profile test might help as a marker of inflammation and risk stratification in patients with COVID-19. Especially in middle- or low-income countries, the test can rapidly help clinicians to delineate prognostic measures and hence management and treatment plans for this disease as the levels of the lipid profile were correlated with the patients’ BMI and infection severity.
Similar content being viewed by others

Plasma lipid levels may change in response to hyperinflammation that develops in severe COVID-19 infection. |
COVID-19 patients with severe infection experience temporary hypertriglyceridemia. |
A routine lipid profile may be used for evaluating severity of COVID-19 patients. |
Introduction
Coronavirus disease 2019 (COVID-19), a life-threatening infectious disease, was seen for the first time in Wuhan 2019. The causative agent is the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [1,2,3,4,5]. It spread in a global pattern to become a serious pandemic [6,7,8]. As of March 2022, more than 485,243,022 people were infected with SARS-CoV-2, and about 6,137,553 have died as a result of this infection worldwide [9]. Even though a lot of information has been accumulated about the disease process and its pathophysiological aspects, the effects of this virus on some metabolic processes and physiological functions still need to be thoroughly investigated.
Patients with COVID-19 could have variations in the levels of their plasma lipid profiles. For example, triglyceride levels may be elevated or inappropriately average for a relatively poor nutritious status, while levels of high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and total cholesterol may be decreased [10,11,12,13,14,15,16,17,18,19,20]. Several recent studies reported significantly decreased levels of LDL-C, HDL-C, and phospholipids in plasma in patients with acute COVID-19 when compared to normal individuals [11, 21, 22].
Moreover, contemporary data reported that patients who have dyslipidemia (i.e., increased plasma levels of cholesterol) are more vulnerable to infection with this virus. It is hypothesized that those patients are mostly receiving medications to treat hypercholesterolemia. This type of medication might inhibit the synthesis of cholesterol or decrease its absorption from the small intestine. Though it can increase angiotensin-converting enzyme 2 (ACE2) expression, such ACE2 receptors are located in lipid-rafts enriched in cholesterol, which serve as an entry site for SARS-CoV-2 [23, 24]. On the other hand, 13,981 cases were evaluated in a recent cohort study conducted on patients receiving statins regularly as a treatment for hypercholesterolemia [25]. They concluded that these patients were at a lower risk for mortality and aggravated inflammatory response when they were infected with COVID-19 [25]. Furthermore, acute respiratory distress syndrome (ARDS) was seen to involve increased activity of secretory phospholipase A2 (sPLA2) in the lungs [26, 27]. The components of the surfactant are phospholipids, which include phosphatidylglycerol, and are hydrolyzed or degraded by sPLA2 [28]. Indeed, these data were reported in a recent study that verified lower levels of prostaglandins (PGs) in the bronco-alveolar lavage (BAL) fluid in ARDS patients when compared to normal volunteers. They justified their data by the hydrolysis of PGs through the increased activity of sPLA2 [26]. Previous studies have also revealed a correlation between COVID-19 infection and lipid profile levels (total cholesterol, LDL-C, and HDL-C) [10,11,12,13,14,15,16,17,18,19,20]. However, the correlation between body mass index (BMI) of patients with COVID-19 infection and their plasma lipid profile levels needs further evaluation. Our study aimed to evaluate the relation between the plasma lipid profile levels and BMI in patients infected with COVID-19.
Materials and Methods
Study Population
This was a prospective, non-randomized observational cohort study conducted from October 2020 to March 2021 at the Nasser General Hospital, which was considered a referral medical center located in Shoubra Al Kheimah, Al Qalyubia Governorate Egypt. Eligible patients were aged 25–84 years with PCR (polymerase chain reaction)-confirmed COVID-19. Patients were diagnosed as having COVID-19 disease when they had general COVID-19 symptoms in addition to respiratory symptoms (fever, sense of fatigue, dry cough, or hard breathing). These patients were tested using the COVID-19 IgG/IgM Rapid Test Kit (Abbexa, Cambridge, UK) to confirm the diagnosis. Patients were assessed by the treating specialists and were classified as group 1 (mild COVID-19) or group 2 (severe COVID-19) according to grade and stage.
Patients with any disorders that could interfere with lipid metabolism or cytokine cascades (autoimmune diseases), a known past medical history of dyslipidemia, chronic or acute kidney injury, and inadequate vascular access were excluded. Additionally, patients who had received medications such as corticosteroids, anti-inflammatory medications, and antibiotics prior to blood sampling were excluded to avoid any interference that might be caused by these medications. Clinical valuations involving history taking, present and past medication, as well as disease history were conducted to check that the patients had not had recent surgery or concomitant treatments listed under the exclusion criteria.
The study protocol was exempted from ethics approval from both Nasser General Hospital local ethics committee and Al Ain University as it was an observational non-interventional study. All study participants gave consent to be enrolled in the study.
Variables
Venous blood samples (4 mL) were obtained from all persons who tested positive to a COVID-19 PCR test and were divided into two aliquots: one aliquot was anticoagulated and divided into two test tubes. The first one was for hematological examinations of total leucocytes count (WBCs) using a Hema Screen 18-Automated Haematology Analyser (Hospitex Diagnostics, Sesto Fiorentino, Italy). The second test tube contained plasma separated for d-dimer with an Sysmex® CA-7000 system coagulation analyzer (Sysmex, Kobe, Japan), and detection of hs-C- reactive protein (CRP) with a Hitachi Model 7600 Series Automatic Analyzer (Hitachi High Technologies Corporation, Hitachi, Japan). The kits used in the experiments were d-dimer PLUS (Siemens Healthcare Diagnostics Products GmbH) and reagent kit for hs-CRP test (latex agglutination assay). Their reference values were 0.1417 (90% CL 0.00–0.55) µg/mL for d-dimer, and < 6 mg/L for hs-CRP, respectively.
From other aliquots of blood, samples could clot, and sera were then separated by centrifugation (3,500 rpm, 20 min, 25 °C) and stored at −20 °C for later biochemical determinations (serum creatinine and lactate dehydrogenase (LDH)). Plasma levels of total cholesterol, LDL-C, HDL-C, triacyclglycerols, and phospholipids were estimated using Synchron cx5 autoanalyzer (Beckman, USA) and calculated with the Friedewald formula.
Statistical Analysis
Based on a previous trial [29], we conducted a power analysis (G power version 3.1 statistical software, Franz Faul, Universität Kiel, Kiel, Germany). The findings indicated a minimum sample size of n = 110 patients (55 patients for each group) based on an α of 5% and a power of 80%, considering a possible loss of about 10% of patients. All quantitative variables were tested for normality using the Shapiro–Wilks test, assessing normal distribution graphical presentations, skewness, and kurtosis coefficients. For normally distributed quantitative variables, descriptive data are presented as mean and standard deviation, for non-normally distributed quantitative variables, median and interquartile ranges are used to present central tendency and variability, while for qualitative data frequency and percentages are used. Continuous normally distributed data were tested with the independent t test, and non-normally distributed quantitative data with the Mann–Whitney U test. Qualitative data were tested using the chi-square and Fisher’s exact tests. All statistical tests were two-tailed and considered statistically significant at a p value < 0.05. Correlations between BMI and lipid profile parameters were investigated by Pearson’s correlation test. Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS®) version 21.0.0.0 (SPSS Inc., Chicago, IL, USA).
Results
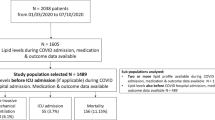
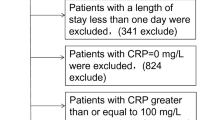
Of 132 patients included in study, 20 patients were excluded as they did not fulfill inclusion criteria, while 112 patients were assigned to informed consent. Baseline characteristics between patients with mild and severe COVID-19 infection (i.e., groups 1 and 2) were not statistically different (Table 1).
As shown in Table 2, most of the biochemical parameters (i.e., plasma triacylglycerols, d-dimer, lactate dehydrogenase, ferritin, CRP, and serum creatinine) evaluated in the study were statistically significantly different between the mild and severe COVID-19 infection groups.
Table 3 represents a correlation between BMI and plasma lipid profile levels of patients with mild and severe COVID-19 infection using Pearson’s correlation. A relatively high correlation was observed between the BMI of severely infected patients and triacylglycerols levels (p = 0.015); however, a significantly negative correlation was observed with HDL-C (p = 0.001).
Discussion
Our study results revealed important changes in hematology parameters in COVID-19-positive patients. The hematology indices show that levels of white blood cells are higher when disease severity increases. Severe COVID 19 disease is usually associated with a significantly exaggerated inflammatory response known as a cytokine storm that is characterized by increased interleukins, leukocytes, neutrophils, other biomarkers such as CRP, and ferritin [30]. However, Zhang et al. reported decreasing leukocyte, lymphocyte, and eosinophil counts for patients infected with severe COVID-19 [31]. This can be explained by the fact that an uncontrolled COVID19 infection and immune response can lead to systemic breakdown and immune impairment [31].
In patients who tested positive for COVID-19, our results have shown a significant increase in LDH, CRP, serum creatinine, and ferritin in patients with severe COVID-19 compared with those with mild COVID-19. Gandini et al. confirmed that hyperferritinemia as a known inflammation factor has been found to be a predictor of ARDS in patients with COVID-19 infection [32]. In addition, hyperinflammation in patients with critical COVID-19 is likely to be beneficial for risk stratification by associated biomarkers (d-dimer, CRP, and ferritin) [33].
Several studies reported that SARS-CoV-2 infection could lead to blood dysfunction, leading to a hypercoagulable state [34,35,36]. Formation of micro-thrombosis that leads to occlusion of the small vessels in the pulmonary circulation of critically ill patients with COVID-19 has been demonstrated by recent evidence in lung pathology dissection [37]. CRP is also an acute-phase reactant (liver-produced inflammatory protein) that can increase under many conditions, such as infection and inflammation [34].
Our results indicate that unlike the plasma total cholesterol, LDL-C and HDL-C levels, the plasma triglyceride levels were increased in patients with serious COVID-19 infection in comparison with those with mild infection. A number of recently published studies showed similar changes in plasma lipid levels in patients with some other infections (Gram-negative bacterial, viral, tuberculosis). In particular, total cholesterol, LDL-C, and HDL-C levels decrease and plasma triglyceride levels in a relatively poor nutritious status are elevated or inappropriately normal [10, 34,35,36,37,38,39].
Our findings showed that there is a relationship between plasma lipid profile and BMI. A positive correlation between BMI and triglyceride levels and disease severity has been observed. On the other hand, HDL-C was negatively correlated with BMI. BMI usually increases due to an increase in adiposity. This is described by increased triglycerides and decreased HDL-C [41]. These data suggest that changes in metabolic parameters might be expected to be related to aerobic fitness and to body fat distribution.
Our results support the evidence that a routine lipid profile test could help as a marker of inflammation and risk stratification in COVID-19 patients. It can help clinicians to delineate prognostic measures and hence management and treatment plans for this disease. In addition to malnutrition, enhanced catabolism during acute illness may explain the low level of HDL but not the increased level of triglycerides. This pattern of dyslipidemia is frequently seen in obese people and patients with diabetes mellitus, which is characterized by enhanced atherogenesis. These patients may be more susceptible to developing a worse scenario in the disease course. Another explanation for this phenomenon may be the cytokine storm and other mediators that influence the inflammatory process in COVID-19. These mediators interfere with lipoprotein lipase (LPL) enzymes and inhibit their function, which might result in suppressed formation of LDL from triglyceride-rich lipoproteins (TRL). This gives rise to the atherogenic pattern of increased triglycerides and decreased HDL levels [41].
Although our study provides a good opportunity for healthcare providers to confirm the diagnosis and severity of COVID-19 patients using lipid profile parameters as indicators, one limitation should be considered. The small sample size means we have to interpret the results with caution and be careful not to generalize the findings. Larger studies investigating this hypothesis are warranted.
Conclusion
A routine lipid profile test could help as a marker of inflammation and risk stratification in COVID-19 patients in addition to other traditional markers. It can help clinicians delineate prognostic measures and hence proper management and treatment plans for this disease as lipid profile levels are correlated with patient BMI and infection severity.
References
Lu H, Stratton CW, Tang YW. Outbreak of pneumonia of unknown etiology in Wuhan, China: the mystery and the miracle. J Med Virol. 2020;92:401–2.
Hui DS, IAE, Madani TA, et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health—the latest 2019 novel coronavirus outbreak in Wuhan, China. Int J Infect Dis. 2020;91:264–6.
Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395:497–506.
Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382:1708–20.
Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323:1061–9.
Young BE, Ong SWX, Kalimuddin S, et al. Epidemiologic features and clinical course of patients infected with SARS-CoV-2 in Singapore. JAMA. 2020;323:1488–94.
Albarello F, Pianura E, Di Stefano F, et al. 2019-novel coronavirus severe adult respiratory distress syndrome in two cases in Italy: an uncommon radiological presentation. Int J Infect Dis. 2020;93:192–7.
Giunta RE, Frank K, Costa H, et al. The COVID-19 pandemic and its impact on plastic surgery in Europe—an ESPRAS survey. Die COVID-19-Pandemie und ihre Auswirkungen auf die Plastische Chirurgie in Europa—Eine ESPRAS Übersicht. Handchir Mikrochir Plast Chir. 2020;52:221–32.
World Health Organization: WHO Coronavirus Disease (COVID-19) Dashboard. 2022. https://covid19.who.int/, Accessed 31 Mar 2022.
Masana L, Correig E, Ibarretxe D, et al. Low HDL and high triglycerides predict COVID-19 severity. Sci Rep. 2021;11(1):7217.
Rezaei A, Neshat S, Heshmat-Ghahdarijani K. Alterations of lipid profile in COVID-19: a narrative review. Curr Probl Cardiol. 2022;47(3): 100907.
Jin H, He J, Dong C, et al. Altered lipid profile is a risk factor for the poor progression of COVID-19: from two retrospective cohorts. Front Cell Infect Microbiol. 2021;30(11): 712530.
Agouridis AP, Pagkali A, Zintzaras E, et al. High-density lipoprotein cholesterol: a marker of COVID-19 infection severity? Atheroscler Plus. 2021;44:1–9.
Feingold KR. The bidirectional link between HDL and COVID-19 infections. J Lipid Res. 2021;62: 100067.
Sampedro-Nuñez M, Aguirre-Moreno N, García-Fraile Fraile L, et al. Finding answers in lipid profile in COVID-19 patients. Endocrine. 2021;74(3):443–54.
Li G, Du L, Cao X, et al. Follow-up study on serum cholesterol profiles and potential sequelae in recovered COVID-19 patients. BMC Infect Dis. 2021;21(1):299.
Zinellu A, Paliogiannis P, Fois AG, et al. Cholesterol and triglyceride concentrations, COVID-19 severity, and mortality: a systematic review and meta-analysis with meta-regression. Front Public Health. 2021;18(9): 705916.
Changaripour S, Sarvazad H, Barghi M, et al. Lipid profile changes in patients with COVID-19 referred to medical centers in Kermanshah, Iran; a case-control study. J Int Med Res. 2022;50(2):3000605221078699.
Zhu Z, Yang Y, Fan L, Ye S, et al. Low serum level of apolipoprotein A1 may predict the severity of COVID-19: a retrospective study. J Clin Lab Anal. 2021;35(8): e23911.
Choi GJ, Kim HM, Kang H. The potential role of dyslipidemia in COVID-19 severity: an umbrella review of systematic reviews. J Lipid Atheroscler. 2020;9(3):435–48.
Hussein MA, Ismail NE, Mohamed AH, et al. Plasma phospholipids: a promising simple biochemical parameter to evaluate COVID-19 infection severity. Bioinform Biol Insights. 2021;15:1–14.
Hussein MA. Administration of exogenous surfactant and cytosolic phospholipase A2α inhibitors may help COVID-19 infected patients with chronic diseases. Coronaviruses. 2021;2:1–20.
Li X, Zhu W, Fan M, et al. Dependence of SARS-CoV-2 infection on cholesterol-rich lipid raft and endosomal acidification. Comput Struct Biotechnol J. 2021;19:1933–43.
Palacios-Rápalo SN, De Jesús-González LA, Cordero-Rivera CD, et al. Cholesterol-rich lipid rafts as platforms for SARS-CoV-2 entry. Front Immunol. 2021;16(12): 796855.
Zhang XJ, Qin JJ, Cheng X, et al. In-hospital use of statins is associated with a reduced risk of mortality among individuals with COVID-19. Cell Metab. 2020;32:176–87.
Seeds MC, Grier BL, Suckling BN. Secretory phospholipase A2-mediated depletion of phosphatidylglycerol in early acute respiratory distress syndrome. Am J Med Sci. 2012;343(6):446–51.
De Luca D, Lopez-Rodriguez E, et al. Clinical and biological role of secretory phospholipase A2 in acute respiratory distress syndrome infants. Crit Care. 2013;24:R163.
Kitsiouli E, Nakos G, Lekka ME. Phospholipase A2 subclasses in acute respiratory distress syndrome. BBA. 2009;1792(10):941–53.
Sun JT, Chen Z, Nie P, et al. Lipid profile features and their associations with disease severity and mortality in patients with COVID-19. Front Cardiovasc Med. 2020;7: 584987.
Samprathi M, Jayashree M. Biomarkers in COVID-19: an up-to-date review. Front Pediatr. 2021;30(8): 607647.
Zhang JJ, Dong Z, Cao YY, et al. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy. 2020;75(7):1730–41.
Gandini O, Criniti A, Ballesio L, et al. Serum Ferritin is an independent risk factor for acute respiratory distress syndrome in COVID-19. J Infect. 2020;81(6):979–97.
Ian H, Raymond P, Michael AL, et al. C-reactive protein, procalcitonin, D-dimer, and ferritin in severe coronavirus disease-2019: a meta-analysis. Ther Adv Respir Dis. 2020;14:1–14.
Khalil RH, Al-Humadi N. Types of acute phase reactants and their importance in vaccination. Biomed Rep. 2020;12(4):143–52.
Levi M, van der Poll T. Coagulation and sepsis. Thromb Res. 2017;149:38–44.
Lin L, Lu L, Cao W. Hypothesis for potential pathogenesis of SARS-CoV2-infection—a review of immune changes in patients with viral pneumonia. Emerg Microbes Infect. 2020;6:1–14.
Lue W, Yu H, Gou J. Clinical pathology of critical patient with novel coronavirus pneumonia (COVID-19). 2020:1–8 (Preprints)
Sproston NR, Ashworth JJ. Role of C-reactive protein at sites of inflammation and infection. Front Immunol. 2018;9:1–11.
Khovidhunkit W, Kim MS, Memon RA, et al. Effects of infection and inflammation on lipid and lipoprotein metabolism: mechanisms and consequences to the host. J Lipid Res. 2004;45:1169–96.
Vekic J, Zeljkovic A, Stefanovic A, et al. Obesity and dyslipidemia. Metabolism. 2019;92:71–81.
Kumari A, Kristensen KK, Ploug M, et al. The importance of lipoprotein lipase regulation in atherosclerosis. Biomedicines. 2021;9(7):782.
Acknowledgements
We are grateful for the support provided by healthcare providers in Nasser General Hospital and are thankful to all patients who gave consent to participate in this important study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Not applicable
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Potential conflicts of interest
All authors report no conflicts of interest relevant to this article.
Institutional review board statement
The study was exempted from ethics approval by the Ethics Committee and Institutional Review Board of Al Ain University as it was descriptive non-interventional study. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Informed consent statement
Written informed consent was obtained from all the participants.
Consent for publication
Consent for publication was received from all the authors.
Availability of data and material
Available upon request from the corresponding author.
Code availability
Not applicable.
Author contributions
AEAW participated in the conception and design of the study, acquisition of data, analysis, and writing and interpretation of data. YOM, HA, and MAH participated in study design and writing while MAB and SG participated in drafting the article and revising it critically for important intellectual content. All authors approved the final version to be submitted.
Rights and permissions
About this article

Cite this article
Mosaad, Y.O., Baraka, M.A., Warda, A.E.A. et al. Plasma lipid profile: a predictive marker of disease severity among COVID-19 patients—an opportunity for low-income countries. Drugs Ther Perspect 38, 286–291 (2022). https://doi.org/10.1007/s40267-022-00916-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40267-022-00916-8