
Abstract
Background
The benefit of anticoagulative treatment to prevent thromboembolism has been established in patients with atrial fibrillation and flutter of all age groups. Traditionally, anticoagulation was underused in geriatric patients with atrial fibrillation and flutter.
Objective
The aim of this study was to assess whether the broad introduction of non-vitamin K antagonist oral anticoagulants into clinical medicine has changed the rate of older patients treated with anticoagulants for atrial fibrillation and flutter.
Methods
Hospitalized geriatric patients treated in 2015 were retrospectively studied for the presence of atrial fibrillation and flutter and the use or non-use of anticoagulation. The risk of stroke and the indication for permanent anticoagulation were assessed using the CHA2DS2-VASc score.
Results
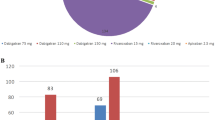
Five hundred and twelve of 1320 patients showed a clear indication for therapeutic anticoagulation (38.8%). Of these, 431 patients (84.2%) had long-standing persistent (> 1 year)/permanent atrial fibrillation and flutter or paroxysmal/persistent (> 7 days) atrial fibrillation and flutter as well as CHA2DS2-VASc scores of ≥ 2 in men and ≥ 3 in women. In this group, 378 patients (87.7%) received anticoagulative treatment. Of all patients anticoagulated for atrial fibrillation and flutter, 221 received non-vitamin K antagonist oral anticoagulants (58.5%), 176 received apixaban (46.6%), 32 received rivaroxaban (8.5%), and 13 received dabigatran (3.4%). One hundred and seven patients received the vitamin K antagonist phenprocoumon (28.3%) and 50 patients received high-dose low-molecular-weight heparins (13.2%). In 21 patients (5.6% of all anticoagulated patients with atrial fibrillation and flutter), hemorrhagic complications were documented. Eleven complications (52.4; 5.0% of all patients treated with non-vitamin K antagonist oral anticoagulants) occurred during treatment with non-vitamin K antagonist oral anticoagulants, four (19.0%) during anticoagulation with phenprocoumon and six (28.6%) during treatment with low-molecular-weight heparins. No intracranial hemorrhages and no fatal bleeding events occurred.
Conclusion
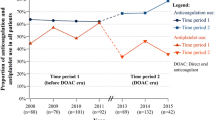
The introduction of non-vitamin K antagonist oral anticoagulants and an increased awareness of their benefits led to an increased use of anticoagulation from 52.8% (2011) to 87.7% (2015) in geriatric patients with atrial fibrillation and flutter at our institution.


Similar content being viewed by others

References
Heeringa J, van der Kuip DA, Hofman A, et al. Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study. Eur Heart J. 2006;27:949–53.
Djukic M, Bergmann D, Jacobshagen C, Nau R. Insufficient use of anticoagulants in geriatric in-patients with atrial fibrillation and flutter. Dtsch Med Wochenschr. 2015;140:e195–200.
Tavernier R, Wolf M, Kataria V, et al. Screening for atrial fibrillation in hospitalised geriatric patients. Heart. 2018;104:588–93.
Cameron C, Coyle D, Richter T, et al. Systematic review and network meta-analysis comparing antithrombotic agents for the prevention of stroke and major bleeding in patients with atrial fibrillation. BMJ Open. 2014;4:e004301.
Mant J, Hobbs FDR, Fletcher K, et al. Midland Research Practices Network (MidReC). Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): a randomised controlled trial. Lancet. 2007;370:493–503.
Appelros P, Farahmand B, Terént A, Åsberg S. To treat or not to treat: anticoagulants as secondary preventives to the oldest old with atrial fibrillation. Stroke. 2017;48:1617–23.
Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace. 2016;18:1609–78.
Zarraga IG, Kron J. Oral anticoagulation in elderly adults with atrial fibrillation: integrating new options with old concepts. J Am Geriatr Soc. 2013;1:143–50.
Rojas-Fernandez CH, Goh J, Hartwick J, et al. Assessment of oral anticoagulant use in residents of long-term care homes: evidence for contemporary suboptimal use. Ann Pharmacother. 2017;51:1053–62.
Connolly SJ, Ezekowitz MD, Yusuf S, RE-LY Steering Committee and Investigators, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139–51.
Granger CB, Alexander JH, McMurray JJV, ARISTOTLE Committees and Investigators, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365:981–92.
Patel MR, Mahaffey KW, Garg J, et al. ROCKET AF Investigators. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883–91.
Potpara TS, Lip GY. Postapproval observational studies of non-vitamin K antagonist oral anticoagulants in atrial fibrillation. JAMA. 2017;317:1115–6.
Yao X, Abraham NS, Sangaralingham LR, et al. Effectiveness and safety of dabigatran, rivaroxaban, and apixaban versus warfarin in nonvalvular atrial fibrillation. J Am Heart Assoc. 2016;5:3725.
Alalwan AA, Voils SA, Hartzema AG. Trends in utilization of warfarin and direct oral anticoagulants in older adult patients with atrial fibrillation. Am J Health Syst Pharm. 2017;74(16):1237–44.
Henrard S, Vandenabeele C, Marien S, Boland B, Dalleur O. Underuse of anticoagulation in older patients with atrial fibrillation and CHADS2 score ≥ 2: are we doing better since the marketing of direct oral anticoagulants? Drugs Aging. 2017;34:841–50.
Halvorsen S, Atar D, Yang H, et al. Efficacy and safety of apixaban compared with warfarin according to age for stroke prevention in atrial fibrillation: observations from the ARISTOTLE trial. Eur Heart J. 2014;35:1864–72.
Hohnloser SH, Basic E, Hohmann C, Nabauer M. Effectiveness and safety of non-vitamin K oral anticoagulants in comparison to phenprocoumon: data from 61,000 patients with atrial fibrillation. Thromb Haemost. 2018;118:526–38.
Connolly SJ, Eikelboom J, Joyner C, AVERROES Steering Committee and Investigators, et al. Apixaban in patients with atrial fibrillation. N Engl J Med. 2011;364:806–17.
Ng KH, Shestakovska O, Connolly SJ, et al. Efficacy and safety of apixaban compared with aspirin in the elderly: a subgroup analysis from the AVERROES trial. Age Ageing. 2016;45(1):77–83.
Pollack CV Jr, Reilly PA, Eikelboom J, et al. Idarucizumab for dabigatran reversal. N Engl J Med. 2015;373:511–20.
Nutescu EA, Burnett A, Fanikos J, Spinler S, Wittkowsky A. Pharmacology of anticoagulants used in the treatment of venous thromboembolism. J Thromb Thrombolysis. 2016;41:15–31.
Harper P, Young L, Merriman E. Bleeding risk with dabigatran in the frail elderly. N Engl J Med. 2012;366:864–6.
Dowlatshahi D, Butcher KS, Asdaghi N, Canadian PCC Registry (CanPro) Investigators, et al. Poor prognosis in warfarin-associated intracranial hemorrhage despite anticoagulation reversal. Stroke. 2012;43:1812–7.
Sharma M, Cornelius VR, Patel JP, Davies JG, Molokhia M. Efficacy and harms of direct oral anticoagulants in the elderly for stroke prevention in atrial fibrillation and secondary prevention of venous thromboembolism: systematic review and meta-analysis. Circulation. 2015;132:194–204.
Başaran Ö, Dogan V, Beton O, et al. Suboptimal use of non-vitamin K antagonist oral anticoagulants: results from the RAMSES study. Medicine (Baltimore). 2016;95:e4672.
Nielsen PB, Skjøth F, Søgaard M, Kjældgaard JN, Lip GY, Larsen TB. Effectiveness and safety of reduced dose non-vitamin K antagonist oral anticoagulants and warfarin in patients with atrial fibrillation: propensity weighted nationwide cohort study. BMJ. 2017;356:j510.
Gage BF, Birman-Deych E, Kerzner R, Radford MJ, Nilasena DS, Rich MW. Incidence of intracranial hemorrhage in patients with atrial fibrillation who are prone to fall. Am J Med. 2005;118(6):612–7.
Garwood CL, Corbett TL. Use of anticoagulation in elderly patients with atrial fibrillation who are at risk for falls. Ann Pharmacother. 2008;42:523–32.
Flaker GC, Pogue J, Yusuf S, Atrial Fibrillation Clopidogrel Trial With Irbesartan for Prevention of Vascular Events (ACTIVE) Investigators, et al. Cognitive function and anticoagulation control in patients with atrial fibrillation. Circ Cardiovasc Qual Outcomes. 2010;3:277–83.
Acknowledgements
We thank Cynthia Bunker, Department of Neuropathology, University Medical Center Göttingen, for her careful language editing of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No sources of funding were received for the conduct of this study or preparation of this article.
Conflict of Interest
Roland Nau received honoararia for lectures from Bayer, Bristol-Myers Squibb, and Pfizer. Claudius Jacobshagen received honoraria from Bayer, Boehringer-Ingelheim, Bristol-Myers-Squibb, Pfizer, and Daichii-Sankyo. Marija Djukic, Larissa Maria Braun, and Steffen Unkel have no conflicts of interest directly relevant to the content of this article.
Ethics Approval
The study was approved by the Ethics Committee of the University Medical Center Göttingen.
Rights and permissions
About this article

Cite this article
Djukic, M., Braun, L.M., Unkel, S. et al. Introduction of Non-Vitamin K Antagonist Anticoagulants Strongly Increased the Rate of Anticoagulation in Hospitalized Geriatric Patients with Atrial Fibrillation. Drugs Aging 35, 859–869 (2018). https://doi.org/10.1007/s40266-018-0571-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40266-018-0571-1