
Abstract
Background
In the era of personalized therapy, targeted treatment in specific patient populations is mandated.
Objective
We evaluated the efficacy and safety of neoadjuvant treatment on locally advanced breast cancer (LABC) with a monoclonal agent against vascular endothelial growth factor (VEGF), bevacizumab plus chemotherapy combination of liposomal doxorubicin, cyclophosphamide and paclitaxel (PLAC-B).
Methods
Patients enrolled were at premenopausal status and characterized by human epidermal growth factor receptor 2 (HER2)-negative, hormone-receptor positive (estrogen receptor/progesterone receptor-positive [ER/PR+]) or triple-negative (TNBC), LABC (T > 3 cm), with high-grade ductal carcinoma. Patients had to have a measurable disease and Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0, with adequate hematologic, renal, and hepatic function. Patients received intravenous liposomal doxorubicin 30 mg/m2, cyclophosphamide 600 mg/m2, paclitaxel 120 mg/m2, and bevacizumab 8 mg/kg on day 1 of 15-day cycles for four cycles (four administrations as neoadjuvant treatment). The primary endpoint was complete clinical (cCR) and pathologic (pCR) response rates, while secondary endpoints included safety, breast-conserving surgery (BCS) conversion rate, and disease-free survival (DFS).
Results
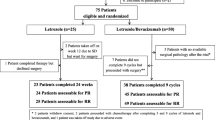
Sixty-two women were enrolled; 20 were ER/PR+ and 42 had TNBC. All underwent surgery, six received mastectomy, and 56 (90.3%) received BCS, with an equal conversion rate from initial indication for mastectomy. cCR was 25.8%. pCR in the breast and axilla occurred in 24 patients (38.7%). pCR was 42.9% for TNBC and 30% for ER/PR+. Hematologic adverse events (AEs) included neutropenia (74.2% total; 22.6% grade 3 [G3]) and febrile neutropenia (6.5% G3); non-hematologic G3 AEs included nausea (6.5%), mucositis (9.7%), and infection (3.2%), all of which were managed without negative sequelae. Over a 3-year follow-up, all patients were alive and DFS was 87.1%.
Conclusion
PLAC-B as neoadjuvant treatment of this subpopulation with TNBC and ER/PR+ patients is effective and safe. Further studies are necessitated.

Similar content being viewed by others


References
American Cancer Society. Cancer facts & figures 2017. https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2017.html. Accessed 17 Sept 2017.
Yao H, He G, Yan S, Chen C, et al. Triple-negative breast cancer: is there a treatment on the horizon? Oncotarget. 2017;8(1):1913–24.
Wahba HA, El-Hadaad HA. Current approaches in treatment of triple-negative breast cancer. Cancer Biol Med. 2015;12:106–16.
Edge SB, Compton CC. The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–4.
Cleator S, Heller W, Coombes RC. Triple-negative breast cancer: therapeutic options. Lancet Oncol. 2007;8:235–44.
Schwartz GF, Hortobagyi GN. Proceedings of the consensus conference on neoadjuvant chemotherapy in carcinoma of the breast, April 26–28, 2003, Philadelphia, Pennsylvania. Cancer. 2004;100(12):2512–32.
Jain RK. Tumor angiogenesis and accessibility: role of vascular endothelial growth factor. Semin Oncol. 2002;29(6 Suppl 16):3–9.
Linderholm BK, Hellborg H, Johansson U, et al. Significantly higher levels of vascular endothelial growth factor (VEGF) and shorter survival times for patients with primary operable triple-negative breast cancer. Ann Oncol. 2009;20:1639–46.
Bell R, Brown J, Parmar M, et al. Final efficacy and updated safety results of the randomized phase III BEATRICE trial evaluating adjuvant bevacizumab-containing therapy in triple-negative early breast cancer. Ann Oncol. 2017;28(4):754–60.
Miller K, O’Neill AM, Dang CT, et al. Bevacizumab (Bv) in the adjuvant treatment of HER2-negative breast cancer: final results from Eastern Cooperative Oncology Group E5103 [abstract no. 500]. J Clin Oncol. 2014;32:5s.
Lenzer J. FDA committee votes to withdraw bevacizumab for breast cancer. BMJ. 2013;343:d4244.
Nahleh ZA, Barlow WE, Hayes DF, et al. SWOG S0800 (NCI CDR0000636131): addition of bevacizumab to neoadjuvant nab-paclitaxel with dose-dense doxorubicin and cyclophosphamide improves pathologic complete response (pCR) rates in inflammatory or locally advanced breast cancer. Breast Cancer Res Treat. 2016;158(3):485–95.
Miles DW, Dieras V, Cortes J, Duenne AA, Yi J, O’Shaughnessy J. First-line bevacizumab in combination with chemotherapy for HER2-negative metastatic breast cancer: pooled and subgroup analyses of data from 2447 patients. Ann Oncol. 2013;24:2773–80.
Jubb AM, Harris AL. Biomarkers to predict the clinical efficacy of bevacizumab in cancer. Lancet Oncol. 2010;11:1172–83.
Sikov WM, Berry DA, Perou CM, et al. Impact of the addition of carboplatin and/or bevacizumab to neoadjuvant once-per-week paclitaxel followed by dose-dense doxorubicin and cyclophosphamide on pathologic complete response rates in stage II to III triple-negative breast cancer: CALGB 40603 (Alliance). J Clin Oncol. 2015;33(1):13–21.
von Minckwitz G, Eidtmann H, Rezai M, et al. Neoadjuvant chemotherapy and bevacizumab for HER2-negative breast cancer. N Engl J Med. 2012;366(4):299–309.
Earl HM, Hiller L, Dunn JA, et al. Efficacy of neoadjuvant bevacizumab added to docetaxel followed by fluorouracil, epirubicin, and cyclophosphamide, for women with HER2-negative early breast cancer (ARTemis): an open-label, randomised, phase 3 trial. Lancet Oncol. 2015;16(6):656–66.
Bear HD, Tang G, Rastogi P, et al. Neoadjuvant plus adjuvant bevacizumab in early breast cancer (NSABP B-40 [NRG Oncology]): secondary outcomes of a phase 3, randomised controlled trial. Lancet Oncol. 2015;16(9):1037–48.
Wolff AC, Hammond ME, Hicks DG, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol. 2013;31(31):3997–4013.
Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumors: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228–47.
Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649–55.
Basch E, Reeve B, Mitchell SA, et al. Development of the National Cancer Institute’s patient-reported outcomes version of the common terminology criteria for adverse events (PRO-CTCAE). J Natl Cancer Inst. 2014;106(9):dju244. https://doi.org/10.1093/jnci/dju244
Francis PA, Regan MM, Fleming GF, et al. Adjuvant ovarian suppression in premenopausal breast cancer. N Engl J Med. 2015;372(5):436–46.
Simon R. Optimal two-stage designs for phase II clinical trials. Control Clin Trials. 1989;10(1):1–10.
Zielinski C, Láng I, Inbar M, et al. Bevacizumab plus paclitaxel versus bevacizumab plus capecitabine as first-line treatment for HER2-negative metastatic breast cancer (TURANDOT): primary endpoint results of a randomised, open-label, non-inferiority, phase 3 trial. Lancet Oncol. 2016;17(9):1230–9.
Bear HD, Tang G, Rastogi P, et al. The effect on surgical complications of bevacizumab added to neoadjuvant chemotherapy for breast cancer: NRG oncology/NSABP protocol B-40. Ann Surg Oncol. 2014;24(7):1853–60.
Golshan M, Cirrincione CT, Sikov WM, et al. Impact of neoadjuvant chemotherapy in stage II-III triple negative breast cancer on eligibility for breast-conserving surgery and breast conservation rates: surgical results from CALGB 40603 (Alliance). Ann Surg. 2015;262(3):434–9.
Tolaney SM, Boucher Y, Duda DG, et al. Role of vascular density and normalization in response to neoadjuvant bevacizumab and chemotherapy in breast cancer patients. Proc Natl Acad Sci USA. 2015;112(46):14325–30.
Kansal KJ, Dominici LS, Tolaney SM, et al. Neoadjuvant bevacizumab: surgical complications of mastectomy with and without reconstruction. Breast Cancer Res Treat. 2013;141(2):255–9.
Zhang H, Huang Z, Zou X, Liu T. Bevacizumab and wound-healing complications: a systematic review and meta-analysis of randomized controlled trials. Oncotarget. 2016;7(50):82473–81.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Ekaterini C. Tampaki, Athanasios Tampakis, Constantinos E. Alifieris, Dimitrios Krikelis, Anastasia Pazaiti, Michalis Kontos, and Dimitrios T. Trafalis declare that they have no conflicts of interest.
Funding
No funding was received for this work.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in this study.
Rights and permissions
About this article

Cite this article
Tampaki, E.C., Tampakis, A., Alifieris, C.E. et al. Efficacy and Safety of Neoadjuvant Treatment with Bevacizumab, Liposomal Doxorubicin, Cyclophosphamide and Paclitaxel Combination in Locally/Regionally Advanced, HER2-Negative, Grade III at Premenopausal Status Breast Cancer: A Phase II Study. Clin Drug Investig 38, 639–648 (2018). https://doi.org/10.1007/s40261-018-0655-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40261-018-0655-z