
Abstract
Predicting the outbreak of a pandemic is an important measure in order to help saving people lives threatened by Covid-19. Having information about the possible spread of the pandemic, authorities and people can make better decisions. For example, such analyses help developing better strategies for distributing vaccines and medicines. This paper has modified the original Susceptible-Infectious-Recovered (SIR) model to Susceptible-Immune-Infected-Recovered (SIRM) which includes the Immunity ratio as a parameter to enhance the prediction of the pandemic. SIR is a widely used model to predict the spread of a pandemic. Many types of pandemics imply many variants of the SIR models which make it very difficult to find out the best model that matches the running pandemic. The simulation of this paper used the published data about the spread of the pandemic in order to examine our new SIRM. The results showed clearly that our new SIRM covering the aspects of vaccine and medicine is an appropriate model to predict the behavior of the pandemic.
Similar content being viewed by others

Introduction
Covid-19 is an infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Chauhan, 2020). The detection of the first case of Covid-19 was reported in Wuhan, China, in December 2019. Since then, the virus continues to spread around the world, threatening the lives of millions of people around the globe. Their livelihood from a financial perspective is also threatened. The disease continues to spread around the world, and the virus continues to mutate through several dominant variants such as alpha, delta, and omicron strains that make contracting the virus even more difficult. Headlines on the topic in the news have decreased as people have to live with it, but the threat still remains and it should not be ignored. Despite the past three years and due to the rapid development, a lot of information about the virus is still unknown. Therefore, the research on this topic is still current and must be continued until the virus is hopefully defeated and, above all, a solid strategy against a recurring pandemic is created.
Measures to control the virus require, among other things, knowledge of the behavior of the virus in relation to its spread (see, e.g., Masudin et al., 2021; Pérez Vergara et al., 2021; Raju, 2021). This information helps to narrow down the virus, or at least gives clues to avoid its spread. The measures themselves are challenging because they are neither clear nor regionally uniform. Furthermore, the impact of wearing masks, lock-downs or quarantines, etc., varies from region to region. This is mainly due to the enforcement capabilities of the authorities, but also to the people themselves, who differ in terms of background and discipline.
However, from a scientific point of view, the work to combat the virus should not rest. There is already a lot of work that is continuing (e.g., Goodarzian et al., 2021; Musulin et al., 2021; Qayyum et al., 2021). In addition to the analysis of the biological structure of the virus, the analysis of the behavior of the virus in terms of its national and international spread is also of great importance (Ahmed et al., 2021; Al Qundus et al., 2021; Mokline & Ben Abdallah, 2022). Such analysis helps to predict the spread better and thus gains an advantage over the virus. We can better prepare ourselves by developing appropriate strategies (e.g., more efficient distribution of vaccines and drugs) against the spread of the virus.
The Covid-19 pandemic is not the first of its kind. Before that, SARSCoV-1 2002,Footnote 1 the influenza A (H1N1) virus (S-OIV) 2009,Footnote 2 MERS-CoV 2012Footnote 3 (e)pandemics had different effects and spread differently. Nevertheless, science has drawn many conclusions from such pandemics. Models have been developed to describe and predict the spread of a pandemic. A widely used model is the Susceptible-Infectious-Recovered (SIR) model originally proposed by Kermack and McKendrick (1927). It divides the population into three groups: Susceptible, Infectious and Recovered. This classification is based on the three phases of a pandemic in relation to its spread in a population. It is generally accepted at an abstract level and applicable to all previous pandemics of this type of CORONA virus.
However, there are many variants of the SIR model that fit the different behavior of CORONA viruses. The course of a spread depends on factors that characterize the disease. For example, the SIR model does not consider reinfection in its basic formulation. A person can be infected and at the same time infects others for a certain period of time, after which the person is considered cured (or even dead). In a study in the UK, participants participated in regular SARS-CoV-2 PCR and antibody testing (every 2–4 weeks) and completed two-weekly questionnaires on symptoms and exposures. Between June 18 and November 09, 2020, 44 reinfections were detected among 6614 participants (Hall et al., 2021). A new study from several universities in the USA concludes that corona reinfection could be possible on average every 16 months; those who have undergone infection with SARS-CoV-2 become reinfected after three months to five years, the US researchers predict (Peeples, 2021). The susceptible-exposed-infectious-recovered (SEIR) model divides the state of infection into two further states: the exposed state, in which a person is already infected but not yet contagious, and the infected state (Li & Muldowney, 1995). Other models such as Susceptible-Asymptomatic-Infectious-Recovered (SAIR) considering asymptomatic patients (Robinson & Stilianakis, 2013), network-susceptible-exposed-infectious-recovered (network-SEIR) tracing contacts (Liu et al., 2020; Shang, 2013), A Multi-Risk-SIR model (MR-SIR) that examines measures targeted to at-risk/age groups (Acemoglu et al., 2020) considers all other initial phases between the infection period and recovery: in the intensive care unit of a hospital. Repeated infections after recovery (whether from the exposed or recovered state) are also possible. The different transition metrics between these stages also play an important role. The metrics in turn depend on various factors, such as the duration of an exposure/infection period and the measures taken, which in turn are influenced by the susceptibility of a population. Obviously, how complex a model can be. The challenge is to cover all possible variants of virus behavior.
Covid-19 brings supply chain management into sharper focus (Sarker et al., 2021). Information systems and sustainable supply chains are essential to a sustainable community and the integration of Big Data management. The sustainable supply chain competition (Gupta et al., 2019; Settembre-Blundo et al., 2021) is developing capabilities to understand natural hazards on an environmental and social level (Al Qundus et al., 2020a). Good supply management strategies and applications for multi-criteria decision making (2020b; Al Qundus et al., 2019) can meet people’s needs even during a pandemic.
The paper contributes in several ways. It aims to provide an overview of the different variants of the SIR model and introduces a new variant of the SIR model. The new variant, which we call SIRM (Susceptible, Infected, Recovered, and Immune), considers the behavior of Covid-19 in relation to infection. In this study, the proposed model SIRM was first mathematically evaluated, taking into account the mathematical constraints of SIR model, such as that the sum of all groups in all phases must equal to the population size. A dataset of the daily Covid-19 statistics in Germany was collected. In this study, the dataset was applied to the SIRM model, which shows very promising results. The results presented serve as a second evaluation of the proposed model using real data sets. The novelty of the SIRM model, in addition to the reinfection aspect, is the introduction of a new state (Immune) that represents the subset of the vaccinated population and the population cured by drugs. To our knowledge, these aspects, particularly the effects of medicine on the distribution of Covid-19 or any other previous pandemic, have not been considered in any published work, underscoring the novelty of this work.
The remainder of the paper is organized as follows: Section “Related Work” provides an overview of the variants of the SIR Model. Section “Variants of SIR Model” introduces the most popular variants of SIR model. Section “SIRM” presents the proposed SIRM model. Section “Research Methodology” provides the research methodology covering section “Analysis” that introduces the mathematical evaluation and section “Data” that describes the used data set. Section “Results” presents the achieved results, which then are discussed in section “Discussion”. Section “Contribution” covers the contribution, and section “Managerial Implications” provides implications for management science. Section “Conclusion” concludes the work with a short summary and gives hints on interesting future perspectives.
Related Work
This section briefly reviews related work, focusing on the work that inspired the proposed approach. The literature search revealed a number of methods relying on several models for investigating the distribution of infectious diseases, i.e., Covid-19. Some are tractable, and others are challenging to interpret.
The impact of Covid-19 is analyzed in Priya et al. (2021) from economic, energy, and environmental perspectives with disastrous consequences for the entire economy. Such studies range from the tourism industry, as reported in Altuntas et al. (2022), to social media platforms, which include various webbased tools that allow internet users to share information virtually, as discussed in Reveilhac and Blanchard (2022) and Sharevski et al. (2022), to the education sector and Sustainability, as reviewed in Chakraborty and Kar (2021) and Kumar et al. (2021c).
Many researchers examined different domains and aspects, such as observing a link between recovery and supply chain coordination in respond to the pandemic (Ivanov, 2021), applying a systematic analysis of the impact of epidemic outbreaks on supply chains (Queiroz et al., 2020), developing an interactive simulation-based methodology to support planning and decision making in complex dynamic systems. Especially when multiple objectives and parameter uncertainties are present (Dunke & Nickel, 2021), investigating lean principles among entrepreneurs (Ufua et al., 2022) and addressing Covid-19 vaccine distribution in developing countries with a model for equitable (Tam et al., 2021; Tavana et al., 2021).
While (Kumar et al., 2021b) modified the traditional Susceptible-Exposed-Infectious-Recovered (SEIR-V) considering social media, particularly Twitter, on the number of influenza and Covid-19 infection cases and deaths to develop a dynamic transmission model to examine the impact of social media and behavioral intervention for these infectious diseases. The SIR model and its variants have been applied to many pandemics in different countries. Currently, the models are used in particular to predict and to study the behavior of Covid19, e.g., in the USA and the largest European countries (Kumar et al., 2021a), in India (Saxena et al., 2021), Ukraine and Qatar (Nesteruk & Benlagha, 2021).
Johnston et al. (2021) have discussed the SIR model and the effect of medicine and vaccines on the Covid-19 distribution. They found that prior medications or vaccines have a significant effect on reducing the total number of deaths. The authors introduce an SIR-type model to include asymptomatic carriers and deceased populations. The model examines the effect of a medicine as well as a vaccine on symptomatically infected individuals, leading to reduction in recovery time and death rates. The authors used data on the number of deaths and cases in the USA since the pandemic began in 2020, and the study simulates this effect with various implications. The results of this simulation show logical conclusions such as: “The earlier the drug or vaccine is released in the population, the lower the number of deaths, as expected.” It is claimed that a vaccine is much more effective than a medicine, provided that the vaccine is used at the beginning of an epidemic.
However, in the case of Covid-19, a medicine has not yet been developed, and the effectiveness of vaccines is still being studied. Therefore, such a comparison is not yet possible. Moreover, the converse can be claimed that a medicine is more effective than a vaccine against spreading a pandemic, since a medicine destroys the virus.
Nevertheless, this work is extremely relevant and inspiring for our work. One of the differences is that our study addresses measurable aspects and neglects others, such as death rates, which do not provide accurate information. In most cases, it is not possible to determine whether a person died because of Covid-19, and the number differs from country to country and even from statistic to statistic. This aspect may lead to bias in the observation. In addition, the above limitations refer to the SIR model itself, so a logical distribution would not be possible. We agree that such a distribution of a pandemic cannot be fully explained by a simple system of equations, but this is generally the case due to theory and not the real world.
Batistela et al. (2021) proposed compartmental model where they modified the SIR model with Susceptible-Infected-Removed-Sick (SIRSi) Model. The authors examined data from three major cities in the Brazilian state of Sao Paulo, which provided estimates of duration and maximum disease incidence. The proposed model accounts for the possibility of unreported or asymptomatic cases, as well as differences in immunity within a population, such as when acquired immunity may be transient. To this end, local asymptotic stability and endemic equilibrium conditions are demonstrated. Their study shows that transient immunity favors a second wave of infection. This depends on the time interval in which a cured individual becomes susceptible again. The logical consequence of a shorter period of reinfection is a larger number of infected patients. The SIRSi model also takes into account the birth–death ratio in the given population and introduces a feedback from the recovered group that did not acquire immunity or lost it after a certain time. The influence of the recurrence feedback is studied analytically and numerically. In addition, the model allows deriving information on unreported and asymptomatic cases. The proposed model with re-susceptibility feedback, fitted to data of confirmed infections, suggests the possibility that recovered patients may have transient or durable immunity. Here, just as the previous model, the death rate was considered, despite erroneous statistics. Vaccination effects were also barely addressed.
Khalilpourazari and Doulabi (2021) proposed a new algorithm that uses machine learning (ML) and evolutionary computation (EC) to model and predict the Covid-19 pandemic in Quebec, Canada. In the context of Covid-19, the reinforcement learning (RL) algorithm can make predictions about the spread of the pandemic. They developed a hybrid reinforced learning-based model and evaluate its accuracy. The developed algorithm is expected to be able to solve complex optimization problems. The authors applied the algorithm to several well-known benchmarks and showed high-quality solutions. However, like many other RL solutions proposed for lockdown strategies to prevent the spread of the pandemic, this study does not consider the impact of vaccination.
Singh and Gupta (2021) proposed a generalized SIR epidemic model (GSIR) as an improved framework for predictive monitoring of the Covid-19 pandemic. It relies on a mathematical model to simulate the spread of this disease in different environments, taking into account cases reported on multiple days. Covid-19 data from different countries were used for the experimental evaluation. Several studies on spread prediction and continuous monitoring show that the model can provide such continuous prediction and monitoring of Covid-19 pandemic with multiple waves. Existing growth function models of the epidemic were presented as special cases of the GSIR model. The parameters used in modeling reflected new aspects such as political decisions, social awareness and medicine availability during the pandemic. Despite the promising results for continuous prediction of the Covid-19 pandemic, the proposed GSIR model relied on a methodology to estimate information important to the study. However,Footnote 4 information such as medicine availability during the pandemic is difficult to obtain. Aspects such as political decisions and social behavior obviously play an important role in the spread of a pandemic, but are difficult to generalize or even model.
Variants of SIR Model
This section provides an overview of the main variants of the SIR Model and what aspects are considered in each of them.
There are numerous models (susceptible-infectious-susceptible SIS Model (Moreno et al., 2002), susceptible-infectious-carrier-recovered Carrier State Model (Cao et al., 2015), susceptible-exposed-infectious-susceptible SEIS Model (Fan et al., 2001), immune-susceptible-exposed-infectious-recovered-susceptible MSEIRS model (Crowe Jr, 2001)) dealing with the prediction of the spread of pandemics. These models take into account the case that a person can be infected several times and, in some cases never becomes immune. For this purpose, transitions are defined when modeling the course of a pandemic, e.g., from a recovered state back to a susceptible state. No such progression has been demonstrated in Covid-19. There are news reports of people becoming reinfected, but this phenomenon cannot be generalized. Therefore, and because of the limited scope of this work, these studies will not be pursued. Instead, this paper will focus on those studies that do not consider reinfection.
The susceptible-infectious-recovered SIR model (Kermack & McKendrick, 1927) as illustrated in Fig. 1 is one of the most widely used models. This model reflects a distribution that intuitively corresponds to the course of most diseases. A person from group S can become infected (group I) is sick with it for a certain period of time and possibly contagious, and then recovers (group R) from it—or dies-, in both cases the person is no longer contagious. The entire population could fall sick or the disease is being controlled, e.g., through measures.

Illustrates the original SIR states Susceptible (S), Infectious (I) and Recovered (R)
The transitions transmission event (TE) and γ are factors representing probabilities between states. TE should be minimized by measures like wearing masks or keeping distances, while γ should be maximized by measures like medical care.
The susceptible-exposed-infectious-recovered SEIR model (Li & Muldowney, 1995) as shown in Fig. 2 has several extensions like SAIR, network-SEIR, SEIRPLUS etc. The model is suitable for describing diseases where there is a period when a person is infected but not yet contagious. The occurrence of symptoms is insignificant. After this exposed state, the course is similar to the SIR model. A disease with such a character can be more harmful to the patient, but it is usually easier to monitor (or control) its spread. The major challenge in taking measures to prevent the spread of a pandemic is to isolate the infectious group from the rest of the population. The additionally exposed group represents a kind of advance warning.

Represents the SEIR states Susceptible (S), Exposed (E), Infectious (I) and Recovered (R)
The SEIRPLUS shown in Fig. 3 is relatively extensive in its representation. Mainly the infected group is divided into three additional states: pre-symptomatic (Ipre), asymptomatic (Iasym), symptomatic (Isym) and hospitalized (strongly symptomatic, IH) (S.M., 2020). This splitting is similar to the SAIR model, but it is granulated more finely. People in the Ipre group are contagious but have not yet developed symptoms. They may develop symptoms and then belong to Group Isym, or they never experience symptoms and then belong to Group Iasym.

Shows the SEIRPLUS* states Susceptible (S), Exposed (E), Infectious (Ipre), Infectious-(a)symptomatic (I(a)pre), Recovered (R) and symptomic being hospitalized (H), death (F) * = derived from https://github.com/ryansmcgee/seirsplus
An infection occurs when there is contact between a person from group S and at least one person from the groups Ipre, asym, sym. This excludes group (E), where a person is infected but not contagious. This is similar to the SEIR model.
In addition, the condition fatal (F) is provided in the case of death. A subset of the Isym develops into a severe clinical condition and must be hospitalized (IH) (S.M., 2020) and could enter this state (F). A person from Iasym, sym, which then gains recovered (R), has a better course.
SIRM
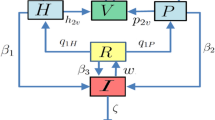
The SIRM model as illustrated in Fig. 4 consists of the states Susceptible (S), Infectious (I), Recovered (R), and Immune (M), which are derived from SIR Model. Immune state takes into account the impact of the use of vaccine and medicine and covers the population subgroup. The transition factors are defined as follows:
-
TE: Transmission Event shows how susceptible become infected
-
β: the vaccination rate from susceptible to immunity
-
ω: the medicine rate from infected to immune
-
γ: the recovery rate from infected to recovered
-
ξ: the rate of recurrence from recovery to susceptible
-
ξ*: the recurrence rate from infected to susceptible.
ξ and ξ* are shown in the illustration, but are not detectable in the course of Covid-19 disease (see sections “Related Work” and “Introduction”), that is why they have not been further considered in this research.

Represents the developed SIRM states Susceptible (S), Infectious (I), Recovered (R), and Immune (M)
The SIRM model proposed in this work is still in its conceptual development. The required transition probabilities between its states cannot be estimated due to the lack of information about the effects of the vaccines and medicine on the course of the Covid-19 outbreak. The vaccines and medicine have not yet been approved or distributed at the time of this work. This prevents the model from being used with real data. As a concept, the model is consistent with the original SIR model and some of its variants. The creation of the SIRM model was based on the same mathematical background as the SIR model. The fulfillment of the derived mathematical rules is presented and justified in section “Research Methodology.”
Research Methodology
This section presents the research methodology conducted. It includes the analysis of the mathematical evaluation and the data set used in this study.
Analysis
Although the SIRM model proposed in this work is still in progress, it can be validated mathematically. A more detailed explanation of the mathematical (transition) symbols has been intentionally omitted in section “Related Work”, since they are similar not only in meaning but also in mathematical background. Most models also share this mathematical concept. There is a generally valid equation (condition) that must always be considered: The sum of the groups (states) of a model must be equal to the population (S) in each step (time t).
The basic mathematics behind the SIR model is based on three groupsFootnote 5: Susceptible S(t), all people who are able to get infected, infectious I(t), people who leave the S(t) group, and recovered R(t), people who leave the infected group and get well. A person in the R(t) group, who is neither infected anymore nor can become infected, will not become susceptible again.
\(\frac{{{{d}}S}}{{{{d}}t}},\frac{{{{d}}I}}{{{{d}}t}},\frac{{{{d}}R}}{{{{d}}t}},\) and \(\frac{{{{d}}M}}{{{{d}}t}}\) represent rates of change, i.e., how the number of susceptible, infected, recovering, and immune individuals changes with regard to time t, respectively.
Equation (1) represents the number of susceptibles at time t. − aSI represents the probability a of susceptibles S come together in contact (multiply) with infected people I. In other words, the probability of interactions between susceptibles and infectious. This must be subtracted from the total group at the time (S(t)). On the other hand, the subgroup aSI is added to the group I shown in Eq. (2). − bI indicates the number of infected that have been cured. b reflects the factors for reducing the number of infected in favor to recovered.Footnote 6 Therefore, the subgroup bI is in both Eqs. (1) and (3): subtracted once and added once, respectively. However, not everyone in bI wins the fight against the disease, some die. Ideally, b and r are equal.



The SIRM model is a new variant of the SIR model. The terms in blue reflect the extension in the equation system of equations. vM in Eq. (1) represents the subgroup of people who have been vaccinated and are immune.Footnote 7 While cM represents the subgroup of infected persons who have been treated with medication.Footnote 8vM and cM become immune in different ways and therefore form a new group, which is summarized in Eq. (4). v and c are factors for the effect of vaccine and medication. These in turn depend on many aspects, such as the distribution strategy of a vaccine and how well a medicine has been tested before use.
Our extension is in harmony with the SIR model and fulfills the general condition of the sum of the population. This extension supports the prediction of the pandemic spread by including vaccine and medicine in the SIR model.
Data
In order to explore the distribution of Covid-19, the investigation began with a Knowledge Base (KB) that includes the rules derived from several well-known and reliable online resources of organizations such as World Health Organization,Footnote 9 Havard Medical School,Footnote 10 Mayo Clinc,Footnote 11 many Government Departments of Health asFootnote 12 and many other online sources managed by doctors such as familyDoctor.Footnote 13 All these resources agree on symptoms and therefore this information is significant. However, our study focuses on information about the rate of reinfection, -if any-, the effect of vaccines and medicine, and the duration and course of the disease. As of March 19, 2020, according to Hendrik Streeck (researcher from Bonn; examined more than 100 infected persons),Footnote 14 there are further symptoms: “About two thirds of the patients complained of a lack of sense of smell and taste.”—“About one third also had diarrhoea.”—“Dry cough and low-grade fever at 91 percent.”
The next step was exploring the data including statistics about Covid-19 cases, several vaccines and vaccination rate, infections and reinfections and recovered rate. Since we are familiar with the system for compiling such statistics in Germany, this study takes into account the data collected there. The data consists of two files covid de vaccines.csv and covid-de.csv covering the columns: date, doses, doses first, doses second, pfizer cumul, moderna cumul, astrazeneca cumul, persons first cumul, persons full cumul, as well as, state, county, age group, gender, date, cases, deaths, recovered, respectively. The data is located in Kaggle,Footnote 15 which contains two files:
-
covid de.csv contains the important data on infection numbers
-
covid de vaccines.csv contains optional data on the vaccination numbers (useful, for example, to determine the parameters to be used per time window).
Results
The development of the SIRM model could be formally evaluated by satisfying the mathematical conditions of the SIR, as described in detail in section “Research Methodology”. Examination of the case study data, i.e., the number of infections in Germany, revealed a polynomial distribution, as can be clearly seen in Fig. 5.

Illustrates the real data distribution considered in the period of the time from 2020-03-27 to 2021-08-10 using the Signal-Savgol-filter
Figure 5 shows such a distribution of Covid-19 infections over the period from March 2020 to August 2021. It can be seen that harmonization forms over smaller sections (time periods), resembling a normalization of the data. By day 200, there is a density of the data that continues between day 420 to day 500. From day 200 to day 400, the polynomial behavior is clearly visible and the density of the infection numbers is also at its lowest.
To obtain a better distribution of the data, the data were normalized and passed through a filter. The filter is a smooth function (signal-savgol-filter), which is represented by the blue line in Fig. 5. Here, a polynomial is easier to recognize. The goal is to apply the mathematical formulation of the SIRM model, which resembles the blue line and follows its course.
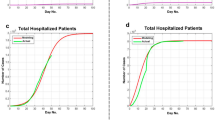
The data were split in terms of distribution difference and passed to the SIRM model. In the flat curves, where the data are densest, the SIRM model takes a very tight curve to the curve of infection numbers. Figure 6 shows this relationship, where the blue line represents the original numbers, while the red line represents the numbers predicted by the SIRM model.

Illustrates the data distribution of the cases (gray curve) comparing to the SIRM model prediction (red curve) in the period of time from 2021-01-01 to 2021-03-01
The larger Fig. 7 shows the overall trend of the data along with the predictions of the model. The red line also has a polynomial shape that can provide an overview of the evolution and spread of Covid-19 using these data.

Illustrates the data distribution of the cases (gray curve) comparing to the SIRM model prediction (red curve) in the period of time from 2020-03-27 to 2021-08-10
The SIRM model is formally correct and has been shown to be effective in a use case with real data.
The next section “Discussion” presents the results in more detail and discusses the observation made as well as the model has been corrected taking into account to make a balance between generalization and overfitting.
Discussion
This section discusses the results achieved to highlight the contribution and link to the impact on management.
Contribution
In our approach, we followed the GRISP model (Chapman et al., 2000) for examining the data, especially in the initial steps of understanding the business model and preparing the data. Real data usually do not follow any logic, especially if they come from nature. This was confirmed by our investigation, especially the distribution of infection numbers is very broad in many time intervals. Many outliers and aggregations of individual data within the data complicate any possible modeling. We also examined different types of natural disasters and different evolutions of the SIR model and its variants. The SIRM model is mathematically correct and can compete with any variant of the SIR model, although it takes into account new and unstudied aspects (vaccination and medicine) that could upset other variants of the SIR model, and thus generally outperforms them.
In the small time intervals, the SIRM model performs well in prediction, as can be seen well in Fig. 6. We were also able to obtain this result in the different segments of the entire period considered. The segments must not exceed 200 days, which is a very good amount of time. This time interval is more than sufficient to predict the spread of the Covid-19 and even to take measures to prevent a worse outbreak. In this way, the proposed model can be applied in its initial phase, but the time intervals may vary and then need to be calibrated.
This good performance of the SIRM model unfortunately decreases when the considered time interval becomes longer. In Fig. 7, it is possible to partially see how the two courses of the original and of the model deviate slightly from each other. Although it is not possible to predict more accurate infection numbers, the curve is being clearly visible, and the model can provide a very good estimate of whether the Covid-19 virus will adopt extreme behavior (in a positive or negative sense) over the long term. To improve performance over the entire time scale, the model was adjusted with a correction factor during implementation. This factor is a constant of (p ∗ 1e + 6) + 0.00005 and was calculated experimentally, so it does not affect the correctness of the model in any way. The error corrector provides the link between the SIRM model and the actual behavior.
Managerial Implications
We live in the time of Covid-19 and consequently not only our health but also our lifestyle is affected by it (see, e.g., Dastisheh & Raju, 2020; Klafke et al., 2021). Countries are trying various approaches to combat the spread of the virus. In addition to laboratory testing, the healthcare industry working on vaccine and medicine development needs to obtain information about the spread of the virus. This information indirectly indicates the impact and performance of the vaccines and medicines being developed. In our study, a new model was developed that takes these aspects into account and provides information not only on the spread of the pandemic but also on the effects of medicine and vaccines. Managers can rely on such information to convince governments and people how effective their products (e.g., medicines and vaccines) are. This work aims to promote the sharing of information related to Covid-19 distribution so that medical company managers can both focus on areas of future need to help combat the virus and benefit from the predictions of the SIRM model.
Future Work Directions
Further work on the SIRM model could include the following research directions:
-
Comparison of multiple data sets from different countries to examine their overlap.
-
Examination of the distribution of Covid-19 with a view to exploring and defining segments or areas of the world.
-
Develop a list of correction factors appropriate for such areas.
-
Extend the SIRM range to increase the prediction time intervals and, in the best case, cover the entire timeline.
-
Calibrate the SIRM model as datasets with statistics on vaccinations and medications become available.
-
Investigate death rate and include it as a metric in the SIRM model that could improve its performance.
-
Investigate the ratio of recurrences (ξ) from healthy to susceptible.
-
Investigate the ratio of recurrences (ξ*) from infected to susceptible.
Conclusion
This paper examines some of the most important models for pandemic outbreak prediction. These models are essentially derived from the SIR model. Pandemics may vary slightly in their course, but such variations can mean that the outbreak cannot be predicted, which means that lives are at risk. It is important to develop variants of predictive models that reflect the character of a pandemic. This work in progress provides a variant of the SIR model, which we call the SIRM model. It consists of the states susceptible-infectious-recovered-immune. The SIRM model fills the gap of considering vaccine and medicine in predicting the outbreak of a pandemic. However, in the case of Covid-19, where vaccine and medicine still need to be developed and approved. The next steps are to improve and to evaluate the SIRM model based on information about the number of new Covid-19 cases while the vaccine or medicine or both are in use.
This work provides the following contributions, which also open several interesting future perspectives:
-
Provision of a new SIRM model focusing on Covid-19, which like the SIR model can also be used to predict the spread of other pandemics.
-
Mathematical theory of the classic SIR model in addition to the novel metrics developed that were not considered in the SIR model or in other more advanced versions of the SIR model.
-
Evaluation of the developed model on the mathematical basis and using real data that confirmed the developed mathematical theory and can be followed in future evaluations.
-
Spread simulation using real data, providing insights into the spread of the pandemic in the countries from which these data were obtained.
-
Highlighting the impact of vaccination and medications on the spread of Covid-19 and providing evidence of the importance of these factors to motivate further investigation.
-
Possibility of obtaining acceptable results without using some metrics such as death rate that are commonly used in the literature but are difficult to achieve in reality.
Notes
For further details, see www.ncbi.nlm.nih.gov/pmc/articles/PMC7074995/.
For further details see www.nejm.org/doi/full/10.1056/NeJMoa0903810.
For further details, see https://doi.org/10.1093/ije/dyaa033.
After the experience we have had in dealing with information coming from the authoritarian.
In terms of the spread degree at time t.
b should be, therefore, maximized. Such factors can be immune system or measures against an infection.
Thus, no longer susceptible to the disease.
Thus, no longer belong to the infected group.
watson.de, www.watson.de/deutschland/coronavirus/283900337-symptome-des-virus-virologe-haben-neue-corona-symptome-entdeckt. Published and Accessed 19 March 2020.
www.kaggle.com/headsortails/covid19-tracking-germany last access 20.10.2021.
References
Acemoglu, D., Chernozhukov, V., Werning, I., & Whinston, M. D. (2020). A multi-risk SIR model with optimally targeted lockdown (Vol. 2020). National Bureau of Economic Research.
Ahmed, S., Taqi, H. M., Farabi, Y. I., Sarker, M., Ali, S. M., & Sankaranarayanan, B. (2021). Evaluation of flexible strategies to manage the covid-19 pandemic in the education sector. Global Journal of Flexible Systems Management, 22(2), 81–105.
Al Qundus, J., Dabbour, K., Gupta, S., Meissonier, R., & Paschke, A. (2020a). Wireless sensor network for AI-based flood disaster detection. Annals of Operations Research, 1–23.
Al Qundus, J., Paschke, A., Gupta, S., Alzouby, A. M., & Yousef, M. (2020b). Exploring the impact of short-text complexity and structure on its quality in social media. Journal of Enterprise Information Management.
Al Qundus, J., Paschke, A., Kumar, S., & Gupta, S. (2019). Calculating trust in domain analysis: Theoretical trust model. International Journal of Information Management, 48, 1–11.
Al Qundus, J., Schäfermeier, R., Karam, N., Peikert, S., & Paschke, A. (2021). Roc: An ontology for country responses towards COVID-19. arXiv preprint arXiv:2104.07345.
Altuntas, F., Altuntas, S., & Dereli, T. (2022). Social network analysis of tourism data: A case study of quarantine decisions in covid-19 pandemic. International Journal of Information Management Data Insights, 2(2), 100108.
Batistela, C. M., Correa, D. P., Bueno, A. M., & Piqueira, J. R. C. (2021). Sirsi compartmental model for covid-19 pandemic with immunity loss. Chaos, Solitons & Fractals, 142, 110388.
Cao, J., Wang, Y., Alofi, A., Al-Mazrooei, A., & Elaiw, A. (2015). Global stability of an epidemic model with carrier state in heterogeneous networks. IMA Journal of Applied Mathematics, 80(4), 1025–1048.
Chakraborty, A., & Kar, A. K. (2021). How did covid-19 impact working professionals–a typology of impacts focused on education sector. The International Journal of Information and Learning Technology.
Chapman, P., Clinton, J., Kerber, R., Khabaza, T., Reinartz, T., Shearer, C., & Wirth, R. (2000). CRISP-DM 1.0: Step-by-step data mining guide. SPSS inc, 9, 13.
Chauhan, S. (2020). Comprehensive review of coronavirus disease 2019 (COVID19). Biomedical Journal, 43(4), 334–340.
Crowe, J. E., Jr. (2001). Respiratory syncytial virus vaccine development. Vaccine, 20, S32–S37.
Dastisheh, A., & Raju, V. (2020). Impact of COVID-19 on sponsorship marketing. Journal: Global Journal of Emerging Sciences, 14–19.
Dunke, F., & Nickel, S. (2021). Simulation-based multi-criteria decision making: an interactive method with a case study on infectious disease epidemics. Annals of Operations Research, 1–30.
Fan, M., Li, M. Y., & Wang, K. (2001). Global stability of an SEIS epidemic model with recruitment and a varying total population size. Mathematical Biosciences, 170(2), 199–208.
Goodarzian, F., Ghasemi, P., Gunasekaren, A., Taleizadeh, A. A., & Abraham, A. (2021). A sustainable-resilience healthcare network for handling covid-19 pandemic. Annals of Operations Research, 1–65.
Gupta, S., Chen, H., Hazen, B. T., Kaur, S., & Gonzalez, E. D. S. (2019). Circular economy and big data analytics: A stakeholder perspective. Technological Forecasting and Social Change, 144, 466–474.
Hall, V. J., Foulkes, S., Charlett, A., Atti, A., Monk, E. J., Simmons, R., Wellington, E., Cole, M., Saei, A., Oguti, B., & Munro, K. (2021). Do antibody positive healthcare workers have lower SARS-CoV-2 infection rates than antibody negative healthcare workers? Large multi-centre prospective cohort study (the siren study), England: June to November 2020.
Ivanov, D. (2021). Exiting the covid-19 pandemic: after-shock risks and avoidance of disruption tails in supply chains. Annals of Operations Research, 1–18.
Johnston, M., Stewart, L., Sun, J., & Zhang, D. (2021). Sir model of time dependent drug and vaccine distribution on covid-19. https://github.com/lairdstewart/SIR-Model-of-Time-Dependent-Drug-and-Vaccine-Distribution-on-COVID-19/blob/main/Final%20Draft.pdf.
Kermack, W. O., & McKendrick, A. G. (1927). A contribution to the mathematical theory of epidemics. Proceedings of the Royal Society of London. Series A Containing Papers of a Mathematical and Physical Character, 115(772), 700–721.
Khalilpourazari, S., & Doulabi, H. H. (2021). Designing a hybrid reinforcement learning based algorithm with application in prediction of the COVID-19 pandemic in Quebec. Annals of Operations Research, 1–45.
Klafke, R., Picinin, C. T., & Chevarria, D. G. (2021). Considerations regarding donation and value co-creation in times of COVID-19 pandemic. Global Journal of Flexible Systems Management, 22(4), 357–376.
Kumar, A., Choi, T.-M., Wamba, S. F., Gupta, S., & Tan, K. H. (2021a). Infection vulnerability stratification risk modelling of COVID-19 data: A deterministic SEIR epidemic model analysis. Annals of Operations Research, 1–27.
Kumar, S., Xu, C., Ghildayal, N., Chandra, C., & Yang, M. (2021b). Social media effectiveness as a humanitarian response to mitigate influenza epidemic and COVID-19 pandemic. Annals of Operations Research, 1–29.
Kumar, V., Alshazly, H., Idris, S. A., & Bourouis, S. (2021c). Evaluating the impact of COVID-19 on society, environment, economy, and education. Sustainability, 13(24), 13642.
Li, M. Y., & Muldowney, J. S. (1995). Global stability for the SEIR model in epidemiology. Mathematical Biosciences, 125(2), 155–164.
Liu, C., Wu, X., Niu, R., Wu, X., & Fan, R. (2020). A new SAIR model on complex networks for analysing the 2019 novel coronavirus (COVID-19). Nonlinear Dynamics, 101(3), 1777–1787.
Masudin, I., Ramadhani, A., Restuputri, D. P., & Amallynda, I. (2021). The effect of traceability system and managerial initiative on indonesian food cold chain performance: A COVID-19 pandemic perspective. Global Journal of Flexible Systems Management, 22(4), 331–356.
Mokline, B., & Ben Abdallah, M. A. (2022). The mechanisms of collective resilience in a crisis context: The case of the ‘COVID-19’ crisis. Global Journal of Flexible Systems Management, 23(1), 151–163.
Moreno, Y., Pastor-Satorras, R., & Vespignani, A. (2002). Epidemic outbreaks in complex heterogeneous networks. The European Physical Journal B-Condensed Matter and Complex Systems, 26(4), 521–529.
Musulin, J., Baressi Šegota, S., Štifanić, D., Lorencin, I., Anđelić, N., Šušteršič, T., Blagojević, A., Filipović, N., Ćabov, T., & Markova-Car, E. (2021). Application of artificial intelligence-based regression methods in the problem of COVID-19 spread prediction: A systematic review. International Journal of Environmental Research and Public Health, 18(8), 4287.
Nesteruk, I., & Benlagha, N. (2021). Predictions of COVID-19 pandemic dynamics in Ukraine and Qatar based on generalized sir model.
Peeples, L. (2021). COVID reinfections likely within one or two years, models propose. Nature.
Pérez Vergara, I. G., López Gómez, M. C., Lopes Martínez, I., & Vargas Hernández, J. (2021). Strategies for the preservation of service levels in the inventory management during COVID-19: A case study in a company of biosafety products. Global Journal of Flexible Systems Management, 22(1), 65–80.
Priya, S. S., Cuce, E., & Sudhakar, K. (2021). A perspective of COVID 19 impact on global economy, energy and environment. International Journal of Sustainable Engineering, 14(6), 1290–1305.
Qayyum, A., Razzak, I., Tanveer, M., & Kumar, A. (2021). Depth-wise dense neural network for automatic COVID19 infection detection and diagnosis. Annals of Operations Research, 1–21.
Queiroz, M. M., Ivanov, D., Dolgui, A., & Wamba, S. F. (2020). Impacts of epidemic outbreaks on supply chains: mapping a research agenda amid the COVID-19 pandemic through a structured literature review. Annals of Operations Research, 1–38.
Raju, V. (2021). Implementing flexible systems in doctoral viva defense through virtual mechanism. Global Journal of Flexible Systems Management, 22(2), 127–139.
Reveilhac, M., & Blanchard, A. (2022). The framing of health technologies on social media by major actors: Prominent health issues and COVID-related public concerns. International Journal of Information Management Data Insights, 2(1), 100068.
Robinson, M., & Stilianakis, N. I. (2013). A model for the emergence of drug resistance in the presence of asymptomatic infections. Mathematical Biosciences, 243(2), 163–177.
Sarker, M., Moktadir, M., & Santibanez-Gonzalez, E. D. (2021). Social sustainability challenges towards flexible supply chain management: Post-COVID-19 perspective. Global Journal of Flexible Systems Management, 22(2), 199–218.
Saxena, R., Jadeja, M., & Bhateja, V. (2021). Propagation analysis of COVID19: An sir model-based investigation of the pandemic. Arabian Journal for Science and Engineering, 1–13.
Settembre-Blundo, D., González-Sánchez, R., Medina-Salgado, S., & García-Muiña, F. E. (2021). Flexibility and resilience in corporate decision making: A new sustainability-based risk management system in uncertain times. Global Journal of Flexible Systems Management, 22(2), 107–132.
Shang, Y. (2013). SEIR epidemic dynamics in random networks. International Scholarly Research Notices, 2013.
Sharevski, F., Huff, A., Jachim, P., & Pieroni, E. (2022). (Mis) perceptions and engagement on Twitter: COVID-19 vaccine rumors on efficacy and mass immunization effort. International Journal of Information Management Data Insights, 2(1), 100059.
Singh, P., & Gupta, A. (2021). Generalized SIR (GSIR) epidemic model: An improved framework for the predictive monitoring of COVID-19 pandemic. ISA Transactions.
S.M., R. (2020). Seirsplus. https://github.com/ryansmcgee/seirsplus/wiki/Extended-SEIRS-Model-Description.
Tam, L. T., Ho, H. X., Nguyen, D. P., Elias, A., & Le, A. N. H. (2021). Receptivity of governmental communication and its effectiveness during COVID-19 pandemic emergency in Vietnam: A qualitative study. Global Journal of Flexible Systems Management, 22(1), 45–64.
Tavana, M., Govindan, K., Nasr, A. K., Heidary, M. S., & Mina, H. (2021). A mathematical programming approach for equitable COVID-19 vaccine distribution in developing countries. Annals of Operations Research, 1–34.
Ufua, D. E., Olujobi, O. J., Tahir, H., Al-Faryan, M. A. S., Matthew, O. A., & Osabuohien, E. (2022). Lean entrepreneurship and SME practice in a post COVID-19 pandemic era: A conceptual discourse from nigeria. Global Journal of Flexible Systems Management, 1–14.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Al Qundus, J., Gupta, S., Abusaimeh, H. et al. Prescriptive Analytics-Based SIRM Model for Predicting Covid-19 Outbreak. Glob J Flex Syst Manag 24, 235–246 (2023). https://doi.org/10.1007/s40171-023-00337-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40171-023-00337-0