
Abstract
Introduction
The aim of the study was to analyze the optical properties of a new hydrophilic enhanced monofocal intraocular lens (IOL) using optical bench analysis and compare it with its monofocal counterpart.
Methods
This laboratory study investigates the enhanced monofocal intraocular lens (L-333) and the monofocal counterpart (L-313) IOL by Teleon Surgical, Spankeren, Netherlands on the optical bench, using OptiSpheric IOL PRO2 (Trioptics, Germany) in order to assess the optical quality according to ISO 11979 with ISO-2 Cornea. IOLs (power 22.0 D) were evaluated regarding through frequency modulation transfer function (MTF), Strehl ratio (SR), and through focus MTF at 50 lp/mm using a 3.0-mm and a 4.5-mm aperture. Tilt and decentration were applied. In addition, wavefront measurements were obtained using WaveMaster® IOL 2 device (Trioptics, Germany) and analyzed.
Results
Centered: The MTF (mean) at 50 lp/mm (L-333/L-313) with 3.0 mm aperture was 0.606/0.724 and with 4.5 mm aperture 0.330/0.409. The SR (mean) with 3.0 mm aperture was 0.586/0.809 and with 4.5 mm aperture 0.330/0.348. Decentered by 1 mm: The MTF (mean) at 50 lp/mm (L-333/L-313) with 3.0 mm aperture was 0.485/0.705 and with 4.5 mm aperture 0.255/0.374. The SR (mean) with 3.0 mm aperture was 0.457/0.739 and with 4.5 mm aperture 0.185/0.268. Tilted by 5 degrees: The MTF (mean) at 50 lp/mm (L-333/L-313) with 3.0 mm aperture was 0.577/0.657 and with 4.5 mm aperture 0.345/0.336. The SR (mean) with 3.0 mm aperture was 0.583/0.702 and with 4.5 mm aperture 0.269/0.237. In through focus MTF and aperture of 3.0 mm, the L-333 showed a peak of 0.41 with some enlarged depth of power of about 2 D. For the aperture of 4.5 mm, the MTF values of L-313 and L-333 were slightly reduced; L-333 showed an MTF peak of 0.23 and some reduced depth of power of about 1.5 D. Wavefront measurements showed no major aberrations for the L-313, while a combination of moderate increase in Z 4-0 and Z 6-0 with opposite sign was revealed for the L-333.
Conclusion
The enhanced monofocal Lentis Quantum (L-333) produces some enlarged depth of focus by combining spherical aberration of different order and opposite sign. The Lentis Quantum performs very well in comparison to the aspherical monofocal counterpart owing to its optical design. Results with large apertures were sufficient too, suggesting that the lens is a good option in eyes with a wide pupil and thus in refractive surgeries of young patients.
Similar content being viewed by others


This is a laboratory study to investigate the new enhanced monofocal IOL and directly compare it to the monofocal counterpart. |
This information should make it easier for the surgeon to select the best possible lens for the individual case. |
The results on the optical bench confirm that the enhanced monofocal IOL has some advantages over the monofocal counterpart without adding typical disadvantages like classic multifocal IOLs. |
Introduction
Cataract surgery ranks as one of the most commonly performed surgical procedures around the world [1]. More than 34 million surgeries are performed annually and monofocal intraocular lenses (IOLs) are used in around 90% of cases. Although there are a lot of so-called premium lenses available from various companies, they only account for around 10% of all cases worldwide. The significantly higher costs are one factor that can play a role in selecting an IOL model depending on the region, health care system, and different cost reimbursement systems.
There has been a paradigm shift. In the past, surgical removal of the opacified lens and restoration of clear vision was the primary goal of cataract surgery. Owing to advances in the surgery itself (technique), lower complication rates, and innovations in implants (new IOL types), surgeries are performed at an earlier stage nowadays. In addition to the permanent removal of the opacified lens, the main goal is to achieve a refractive improvement, too. Phacoemulsification has evolved from a vision restoration procedure to a refractive procedure. The main focus is to improve quality of life and achieve maximum patient satisfaction. As a result of increased life expectancy and an active lifestyle with various hobbies, an increasing number of elderly patients are interested not only in perfect distance vision but also in spectacle independence in near and/or intermediate distances. Presbyopia-correcting lenses were developed to make this possible, but as a result of their optical properties they can also lead to undesirable effects (dysphotopsia), like halo and glare. Three main categories of IOLs can be distinguished: typical multifocal lenses (MIOLs) with refractive or diffractive design, accommodative IOLs, and enhanced depth of focus (EDoF) IOLs [2].
The basic optical principle is to create a single elongated focal point to enhance the depth of focus, in contrast to monofocal IOLs (in which light is focused on one single point) or multifocal IOLs, which have two (bifocal) or three (trifocal) discrete points. The goal is to combine the advantages of both systems without creating additional disadvantages, i.e., to improve intermediate vision without degrading distance vision compared to a typical monofocal lens [3]. The aim is to avoid the overlapping of near and distance images that occurs with conventional MIOLs, thus avoiding the halo effect and reduced contrast sensitivity as much as possible. EDoF IOLs are designed to produce a continuous range of focus without asymmetric IOL power distribution and secondary out-of-focus images. Therefore, EDoF IOLs do not have secondary out-of-focus images at each focal point like typical MIOLS. The severity of these phenomena in MIOLs depends mainly on lens design, power of addition, and pupil size [4,5,6]. Several laboratory studies and optical bench reports have shown that EDoF IOLs provide better optical quality than multifocal lenses with lower risk of dysphotopsia but provide less improvement and (in practice) inadequate uncorrected vision for near distance [7,8,9,10,11,12].
On the basis of the IOL technologies and optic design, some researches have proposed to differentiate two groups of EDoF lenses: pure EDoF IOLs and hybrid MF-EDoF IOLs [2]. Pure EDoF IOLs exclusively use spherical aberration-based optics or the pinhole effect. Hybrid MF-EDoF IOLs combine multifocality with low addition power and the EDoF technology and can be subdivided into diffractive EDoF IOLs, refractive EDoF IOLs, and diffractive-refractive EDoF IOLs.
The Lentis Quantum (L-333) by Teleon Surgical (Spankeren, Netherlands) bridges the gap between standard aspheric monofocal IOLs and premium refractive IOLs. This enhanced monofocal, aberration-neutral IOL is designed with Q-zone technology, which is a progressive surface profile that provides a smooth, stepless transition between zones to avoid any undesirable visual sides effects such as halos and glare. The basic Quantum EDoF principle is to create a single elongated focal range to enhance depth of focus. A “slope-dependent” Q-type asphericity is used for a progressive power profile.
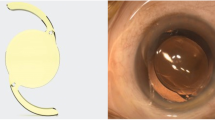
The L-333 is a foldable, one-piece monofocal posterior chamber lens with plate haptic design; the size of the spherical aberration neutral optic is 6.0 mm and the overall diameter is 11.0 mm (Fig. 1). The optic and haptics are equipped with a continuous posterior square edge design to achieve a 360° barrier effect. The material of the lens is called Hydrosmart®, a copolymer consisting of hydrophilic acrylates with hydrophobic surface. The biconvex optical design has a modified posterior aspherical surface. The lens is available from 10.0 to 30.0 diopters (D), in 0.5-D increments, and the refractive index is 1.46. The recommended injector is Medicel’s Viscojet Bio 2.2 and the lens can be implanted through a 2.0-mm clear corneal incision. The actual incision size is of course highly dependent on the IOL injection technique used; accordingly, it differs for wound-assisted, into-the-wound, and into-the-bag techniques.

Lentis Quantum (L-333) by Teleon Surgical (Spankeren, Netherlands) is an enhanced monofocal, aspherical, foldable, one-piece intraocular lens with a plate haptic design and 360° square edges. The overall diameter is 11.0 mm and the optic diameter is 6.0 mm (left). The UV-absorbing material (Hydrosmart®) is a copolymer, consisting of hydrophilic acrylates with hydrophobic surface and a refractive index of 1.46. These specifications are identical for the monofocal counterpart (L-313). Slit lamp image showing the lens well positioned in the capsular bag (right)
The L-333 is called an enhanced monofocal IOL as it provides patients with more vision in the intermediate distance (80 cm) compared with traditional monofocal IOLs but with comparable contrast sensitivity. Teleon Surgical clearly distinguishes this new Lentis Quantum (L-333) lens from the already available Lentis Comfort (L-315 MF15) which is a classic EDoF lens with sector-shaped design and a low near-segment, intended to cover more of the 60 cm range.
According to the American Academy of Ophthalmology (AAO) Consensus Statement for EDoF IOLs, an important criterion for EDoF IOLs is that these lenses are intended to enhance intermediate range of vision while maintaining high-quality distance vision and must not offer any disadvantages to the control group with a monofocal counterpart [13].
Therefore, we tested the L-333 on the optical bench and compared the results to its monofocal counterpart, the L-313, a classic monofocal aspheric lens. The two tested lenses consist of the same material and share exactly the same dimensions and plate haptic design.
Methods
We studied two IOL models (L-333 and L-313, Teleon Surgical, Spankeren, Netherlands), each having the same refractive power of + 22.0 D, on the optical bench with the OptiSpheric IOL PRO 2 and the Wavemaster IOL 2 (Trioptics, Wedel, Germany). This laboratory study is exempt from ethics committee approval as it is an optical bench analysis (in vitro study) without humans involved.
Quality Criteria for Optical Images
The modulation transfer function (MTF) describes the contrast sensitivity of a lens system. The MTF is the imaging power of a lens at different spatial frequencies in the tangential and sagittal directions.
The Strehl number takes into account all the small oscillations that occur on the MTF curve and reflects the overall optical performance of an IOL.
The Strehl ratio (SR) is a measure of the imaging quality of an optical system over its entire spatial frequency range compared to the corresponding ideal (diffraction-limited) system. Thus, a perfect IOL would have an SR value of 1.0. The smaller the SR value, the poorer the optical quality. To simulate photopic and mesopic pupil conditions, measurements were performed with two different aperture sizes (3.0 and 4.5 mm). All measurements were performed independently by the Trioptics company (Wedel, Germany) on its own optical bench, and the results were confirmed with official certificates. All devices used are considered gold-standard and the measurements followed the guidelines of the International Organization for Standardization. The OptiSpheric IOL PRO 2 (Trioptics, Wedel, Germany) device was used to assess the optical quality of the two IOL models (L-333 and L-313). The following parameters were used: ISO-2 cornea (+ 0.28 µm), ISO 11979/2, lens placement in situ in NaCl with 35 °C temperature, 546 nm, and selection of different aperture sizes (3.0 mm vs 4.5 mm). All measurements were repeated three times and performed on two different lenses of the same type. For each measurement, five tangential and five sagittal measurements were obtained and averaged. The following settings were used: centered IOL, decentered IOL (1.0 mm), and tilted IOL (5°).
The WaveMaster IOL 2 (Trioptics, Wedel, Germany), a high-resolution Shack–Hartmann sensor in reverse projection setup, was used to evaluate the aberrations of the IOLs. An in situ model eye was used according to ISO 11979 in saline solution with 546 nm, mask width 4.51, corresponding to standard settings and to a mesopic pupil.
Zernike polynomials up to 10th order were determined by means of the measured wavefront that describe the optical properties of the IOL. It should be noted that spherical aberrations are caused mainly by the optical design of the lens, and asymmetric aberrations (such as Coma, Trifoil) can occur as a result of lens errors. A value of Zernike coefficient greater than 0.1 µm was defined as optically relevant.
Results
Optical Quality Assessment
The through frequency MTF curves of all IOLs measured at the best focus through the 3.0 mm (Figs. 2, 3, 4) and 4.5 mm (Figs. 5, 6, 7) apertures are presented (Tables 1, 2). Centered: The MTF (mean) at 50 lp/mm (L-333/L-313) with 3.0 mm aperture was 0.606/0.724 and with 4.5 mm aperture 0.330/0.409. The SR (mean) with 3.0 mm aperture was 0.586/0.809 and with 4.5 mm aperture 0.330/0.348. Decentered by 1 mm: The MTF (mean) at 50 lp/mm (L-333/L-313) with 3.0 mm aperture was 0.485/0.705 and with 4.5 mm aperture 0.255/0.374. The SR (mean) with 3.0 mm aperture was 0.457/0.739 and with 4.5 mm aperture 0.185/0.268. Tilted by 5°: The MTF (mean) at 50 lp/mm (L-333/L-313) with 3.0 mm aperture was 0.577/0.657 and with 4.5 mm aperture 0.345/0.336. The SR (mean) with 3.0 mm aperture was 0.583/0.702 and with 4.5 mm aperture 0.269/0.237. Strehl findings were in accordance with the MTF results. This indicates, with certain limits, the corresponding expected retinal image quality (Tables 1, 2).

Through frequency modulation transfer function (MTF mean) curves with 3.0 mm aperture and centered IOLs

Through frequency modulation transfer function (MTF mean) curves with 3.0 mm aperture and decentered IOLs

Through frequency modulation transfer function (MTF mean) curves with 3.0 mm aperture and tilted IOLs

Through frequency modulation transfer function (MTF mean) curves with 4.5 mm aperture and centered IOLs

Through frequency modulation transfer function (MTF mean) curves with 4.5 mm aperture and decentered IOLs

Through frequency modulation transfer function (MTF mean) curves with 4.5 mm aperture and tilted IOLs
There was a minor shift of the main focus in relation to the nominal power of each IOL. We did not adjust this shift which is common in such settings and may be due to the manufacturer’s tolerances or to distinct measurement defocus because of different nominal spherical aberration in relation to the ISO-2 cornea applied [14].
Lentis Quantum (L-333) proved to have an enlarged depth of focus compared to the standard monofocal optics of L-313 and could be observed especially for the small aperture, corresponding to photopic pupil sizes. Tests with large apertures, corresponding to mesopic pupil sizes, showed that this benefit in depth-of-focus of the L-333 slightly decreased, showing up as a slightly reduced overall MTF performance.
Through Focus MTF
To compare the depth-of-focus performance of both IOLs, the through focus performance was defined as an MTF better than 0.1. For the aperture of 3.0 mm (Fig. 8), L-313 showed a pronounced peak in MTF of about 0.71 with a depth of power of 1 D. L-333 showed an MTF peak of 0.41 with some enlarged depth of power of about 2 D and two cusps in the MTF curve.

Through focus modulation transfer function (MTF mean) with IOLs centered and aperture 3.0 mm
As expected, for the aperture of 4.5 mm (Fig. 9), the MTF values of L-313 and L-333 were markedly reduced, with a shape of the through focus curves roughly similar to the aperture of 3 mm. L-313 showed an MTF peak of 0.35 and again a depth of power of about 1 D. L-333 showed an MTF peak of 0.23 and some reduced depth of power of about 1.5 D. Note: Both IOLs had the exact same power. During the measurement, changes on the y-axis may occur due to speed and temperature differences during the measurement, but these have no influence on the curve and the actual results. One should only pay attention to the shape of the curve. The results have been confirmed and validated by Trioptics.

Through focus modulation transfer function (MTF mean) with IOLs centered and aperture 4.5 mm
Wavefront
The wavefront maps of L-333 and L-313 and the Zernike coefficients are presented in Figs. 10 and 11.

Wavefront mapping of the lens L-333. Overall peak-to-valley (PV) and root mean square (RMS) in micrometers (left). Measured Zernike coefficients are presented (right). Lower- and higher-order aberrations (HOA) up to 10th order were obtained. Values more than 0.1 µm are considered as optically relevant

Wavefront mapping of the lens L-313. Overall peak-to-valley (PV) and root mean square (RMS) in micrometers (left). Measured Zernike coefficients are presented (right). Lower- and higher-order aberrations (HOA) up to 10th order were obtained. Values more than 0.1 µm are considered as optically relevant
For the enhanced monofocal IOL (L-333), the spherical aberration Z 4-0 was about − 0.14 µm and the secondary spherical aberration Z 6-0 was about 0.14 µm. No other relevant aberration showed up. Peak-to valley (PV) was 0.53 µm and root mean square (RMS) was 0.09 µm. For the monofocal counterpart (L-313), a spherical aberration Z 4-0 of about − 0.13 µm was detected. Horizontal coma of about 0.15 µm and oblique astigmatism of about − 0.11 µm were revealed.
Discussion
Through focus MTF curves show that the Lentis Quantum L-333 enhances the depth of focus to some extent compared to the monofocal counterpart (L-313). Through frequency MTF and Strehl ratio of L-333 were only slightly decreased compared to L-313. This fact could lead to only a minor decrease in contrast sensitivity in a patient’s eyes (real-life conditions).
We have shown that the Lentis Quantum (L-333) enhances the depth of focus seen in the MTF curves by combining spherical aberration (Z 4-0) and secondary spherical aberration (Z 6-0) of opposite sign. This approach was discussed in the literature in recent years, and is applied to other novel IOL optics like the LuxSmart IOL (Bausch&Lomb) [15,16,17,18].
In recent years, vision requirements for elderly people have changed and as a result of popular activities, such as reading or typing on mobile phones and other devices like tablets or using various screens, the intermediate vision (distance of 60–80 cm) is becoming more and more important. Although in the last few decades the quality of typical multifocal IOLs was improved and the implantation of these lenses was also very successful and increased patient satisfaction, cases with undesired side effects, primarily occurrence of dysphotopsia, were described. These halo and glare phenomena have partially reduced overall patient satisfaction. It is also noteworthy that in 2021 only 10% of the lenses implanted worldwide belonged to the group of so-called premium lenses.
There has been an enormous amount of change in the sector of premium IOLs in recent years. All manufacturing companies have worked on the development of such lenses. A variety of EDoF and enhanced monofocal lenses are currently available on the market. The main goal of enhanced monofocal IOLs is to maintain the reliable uncorrected distance visual acuity and low dysphotopsia rates of monofocal IOLs, improve depth of focus for improved functional intermediate vision performance, and increase spectacle independence.
In direct comparison, it is necessary to highlight some differences: there is less depth of focus with enhanced monofocal design but more than with pure monofocals, low halo and glare, and good contrast. Moreover, there are relatively large differences in price.
Pure EDoF lenses should be used as monofocal lenses with a minor improvement for near vision; one can expect to achieve good or adequate intermediate vision (60–80 cm) but reduced quality of near vision (40 cm). Using MIOL hybrid IOLs, one can achieve good distance vision and reduced quality of near vision compared to typical MIOLs but keeping the same quality of retinal image for intermediate vision and at the same time decreasing the risk of halo and glare effects. Therefore, these IOLs are probably a good option for conservative indications or a kind of “new standard” of basic care.
However, if a patient has high demands, especially for near/reading distance (40 cm), then a typical MIOL is the best alternative and possible side effects have to be discussed in advance. It can be emphasized that each lens optic/design shows certain advantages and disadvantages and the selection of the right (best) lens model should be made according to individual needs. Therefore, in addition to exact preoperative measurements, the preoperative conversation between ophthalmologist and patient is particularly important to obtain all information for precise model selection. Laboratory and optical bench studies appear to be an enormously important tool to objectively evaluate the design of the multitude of lens models on the market and provide a means of comparison for surgeons. Nevertheless, careful clinical studies with high numbers of cases and carefully selected measurements/parameters have to be performed to obtain clinical data. Thus far, very few clinical studies have heeded the AAO’s suggestions stated in the Consensus Statement in 2017 [13].
It seems to be especially important to discuss the distance range with patients prior to surgery to select the best and most suitable IOL in the individual case. The Lentis Quantum (L-333) as an enhanced monofocal IOL targets a focus of approximately 80 cm, while the LS-313 MF15, also offered by Teleon Surgical, targets a distance of 60 cm as a “true” EDoF IOL. Since these lenses are otherwise identical in terms of dimensions and material properties, a mix and match procedure also seems very suitable. In this way, an even wider focal range can be achieved (binocularly) in the intermediate range without risk of halo and glare. The authors are currently performing clinical evaluations of this strategy and results will be presented soon.
Limitations of the Study
It should be emphasized that this is a laboratory study. Clinical results and long-term outcomes are of course equally important to assess the overall performance of a new lens and assess the optical design. In addition, the new enhanced monofocal lens should be compared with other direct competitors in the future.
Conclusion
The results on the optical bench regarding MTF and Strehl showed no difference between the monofocal L-313 and the enhanced monofocal L-333. The Lentis Quantum performs very well in comparison to other spherical and aspherical monofocal lenses; owing to its optical design, it shows a kind of tolerance to decentration and tilt compared to typical multifocal IOLs. Good results were also seen at large apertures, making the lens a good option in eyes with a wide pupil and thus in refractive surgeries of young patients.
The Lentis Quantum bridges the gap between standard aspheric monofocal IOLs and premium refractive IOLs. This enhanced monofocal, aberration-neutral IOL is designed with Q-zone technology, which is a progressive surface profile that provides a smooth, stepless transition between zones to avoid undesirable visual sides effects such as halos and glare. The IOL provides patients with more vision in the intermediate distance (80 cm) compared with traditional monofocal IOLs but with comparable contrast sensitivity.
The knowledge of EDoF and enhanced monofocal lenses, their optical principles, their intended focus, and their correct use by the surgeon are necessary to offer the patient the best option. A uniform definition and classification of all models on the market as well as laboratory comparative work including multicenter clinical studies is necessary.
References
Market Scope. IOL market report: mid-year update. St. Louis: Market Scope; 2020.
Alio JL, Plaza-Puche AB, Férnandez-Buenaga R, Pikkel J, Maldonado M. Multifocal intraocular lenses: an overview. Surv Ophthalmol. 2017;62(5):611–34. https://doi.org/10.1016/j.survophthal.2017.03.005.
Savini G, Balducci N, Carbonara C, et al. Functional assessment of a new extended depth-of-focus intraocular lens. Eye (Lond). 2019;33(3):404–10. https://doi.org/10.1038/s41433-018-0221-1.
Savini G, Schiano-Lomoriello D, Balducci N, Barboni P. Visual performance of a new extended depth-of-focus intraocular lens compared to a distance-dominant diffractive multifocal intraocular lens. J Refract Surg. 2018;34(4):228–35. https://doi.org/10.3928/1081597X-20180125-01.
Gallego AA, Bará S, Jaroszewicz Z, Kolodziejczyk A. Visual Strehl performance of IOL designs with extended depth of focus. Optom Vis Sci. 2012;89(12):1702–7. https://doi.org/10.1097/OPX.0b013e3182775e1a.
Böhm M, Petermann K, Hemkeppler E, Kohnen T. Defocus curves of 4 presbyopia-correcting IOL designs: diffractive panfocal, diffractive trifocal, segmental refractive, and extended-depth-of-focus. J Cataract Refract Surg. 2019;45(11):1625–36. https://doi.org/10.1016/j.jcrs.2019.07.014.
McNeely RN, Moutari S, Palme C, Moore JE. Visual outcomes and subjective experience after combined implantation of extended depth of focus and trifocal IOLs. J Refract Surg. 2020;36(5):326–33. https://doi.org/10.3928/1081597X-20200318-01.
Kanclerz P, Toto F, Grzybowski A, Alio JL. Extended depth-of-field intraocular lenses: an update. Asia Pac J Ophthalmol (Phila). 2020;9(3):194–202. https://doi.org/10.1097/APO.0000000000000296.
Rampat R, Gatinel D. Multifocal and extended depth-of-focus intraocular lenses in 2020. Ophthalmology. 2021;128(11):e164–85. https://doi.org/10.1016/j.ophtha.2020.09.026.
Khandelwal SS, Jun JJ, Mak S, Booth MS, Shekelle PG. Effectiveness of multifocal and monofocal intraocular lenses for cataract surgery and lens replacement: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2019;257(5):863–75. https://doi.org/10.1007/s00417-018-04218-6.
Rodov L, Reitblat O, Levy A, Assia EI, Kleinmann G. Visual outcomes and patient satisfaction for trifocal, extended depth of focus and monofocal intraocular lenses. J Refract Surg. 2019;35(7):434–40. https://doi.org/10.3928/1081597X-20190618-01.
Liu J, Dong Y, Wang Y. Efficacy and safety of extended depth of focus intraocular lenses in cataract surgery: a systematic review and meta-analysis. BMC Ophthalmol. 2019;19(1):198. https://doi.org/10.1186/s12886-019-1204-0.
MacRae S, Holladay JT, Glasser A, et al. Special report: American Academy of Ophthalmology Task Force consensus statement for extended depth of focus intraocular lenses. Ophthalmology. 2017;124(1):139–41. https://doi.org/10.1016/j.ophtha.2016.09.039.
Chae SH, Son HS, Khoramnia R, Lee KH, Choi CY. Laboratory evaluation of the optical properties of two extended-depth-of-focus intraocular lenses. BMC Ophthalmol. 2020;20(1):53. https://doi.org/10.1186/s12886-020-1332-6.
Yi F, Iskander DR, Collins M. Depth of focus and visual acuity with primary and secondary spherical aberration. Vis Res. 2011;51(14):1648–58. https://doi.org/10.1016/j.visres.2011.05.006.
Benard Y, Lopez-Gil N, Legras R. Optimizing the subjective depth-of-focus with combinations of fourth- and sixth-order spherical aberration. Vision Res. 2011;51(23–24):2471–7. https://doi.org/10.1016/j.visres.2011.10.003.
Schmid R, Borkenstein AF. Analysis of higher order aberrations in recently developed wavefront-shaped IOLs. Graefes Arch Clin Exp Ophthalmol. 2022;260(2):609–20. https://doi.org/10.1007/s00417-021-05362-2.
Borkenstein AF, Borkenstein EM, Luedtke H, Schmid R. Optical bench analysis of 2 depth of focus intraocular lenses. Biomed Hub. 2021;6(3):77–85. https://doi.org/10.1159/000519139.
Acknowledgements
We would like to thank the company Trioptics (Wedel, Germany) which carried out measurements according to their scientific standards and ISO guidelines and provided us with official certificates for the measurements.
Funding
No funding or sponsorship was received for this study or publication of this article. The journal’s Rapid Service Fee was funded privately without external subsidies by all authors.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
AFB was the leading author, designed the concept of the study, and wrote the draft of the manuscript. All authors critically reviewed the manuscript and contributed significantly to the final manuscript.
Disclosures
Andreas F Borkenstein, Eva-Maria Borkenstein and Ruediger Schmid have no proprietary or commercial interest in the medical devices that are involved in this manuscript and confirm that they have nothing to disclose.
Compliance with Ethics Guidelines
The laboratory study is exempt from ethics committee approval as it is an optical bench analysis (in vitro study) without humans involved.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Borkenstein, A.F., Borkenstein, EM. & Schmid, R. Evaluating Optical Quality of a New Hydrophilic Enhanced Monofocal Intraocular Lens and Comparison to the Monofocal Counterpart: An Optical Bench Analysis. Ophthalmol Ther 11, 2045–2056 (2022). https://doi.org/10.1007/s40123-022-00561-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40123-022-00561-4