
Abstract
Introduction
Chronic pain is a public health issue, leading to substantial healthcare costs and diminished quality of life for sufferers. While the role of anxiety in pain modulation has been extensively studied, the effects of other emotional states on the body’s pain control mechanisms remain less understood. This study sought to explore how different emotions (happiness, anger, sadness, and interest) affect conditioned pain modulation (CPM) and the wind-up phenomenon in healthy adults.
Methods
This randomized controlled, cross-over trial involved 28 healthy participants aged 18–60. Participants watched video clips designed to induce specific emotions: happiness, anger, sadness, and interest. Emotional states were assessed using a 7-point Likert scale. Pain modulation was measured using CPM and the wind-up phenomenon. CPM was assessed with a hot water bath as the conditioning stimulus and pressure pain tolerance as the test stimulus. Wind-up was measured using pinprick needle stimulators and a visual analog scale. Data were analyzed using paired t tests to compare pre- and post-emotion induction values.
Results
Significant changes in emotional self-assessment values were observed for all emotions. Happiness increased CPM (4.6 ± 11.4, p = 0.04277), while sadness − 9.9 ± 23.1, p = 0.03211) and anger − 9.1 ± 23.3, p = 0.04804) decreased it. Interest did not significantly alter CPM (− 5.1 ± 25.8, p = 0.31042). No significant effects were found for the wind-up phenomenon across any emotional states.
Conclusion
This study shows that emotional states significantly affect the body’s ability to modulate pain. Positive emotions like happiness enhance pain inhibition, while negative emotions such as sadness and anger impair it. These findings suggest that emotional modulation techniques could be integrated into pain management strategies to improve patient outcomes. Further research should explore a broader range of emotions and include objective measures to validate these results.
Plain Language Summary
Chronic pain is a widespread problem that affects millions of people and leads to high healthcare costs and decreased quality of life. Understanding how emotions impact pain can help us find better ways to manage it. This study looked at how different emotions (happiness, anger, sadness, and interest) affect the ability of the body to naturally control pain in healthy adults. Participants experienced different tests in a random order, like flipping a coin to decide the order. Each participant took part in all the tests to compare how different conditions affected them. We measured changes in their pain perception using two methods: conditioned pain modulation, which reflects how well the body can suppress pain after experiencing another painful stimulus, and the wind-up phenomenon, which measures how pain intensity increases with repeated stimulation. We found that emotions affected the body’s ability to control pain. Sadness and anger reduced the efficacy of conditioned pain modulation, making it harder for the body to reduce pain. Happiness improved CPM, enhancing the body’s natural ability to stop pain. Interest did not significantly change how pain was felt. We also did not find any significant changes in the wind-up phenomenon for any of the emotions tested. The results suggest that positive emotions like happiness can help reduce pain, while negative emotions like sadness and anger can make pain worse. This could lead to new pain management approaches that include methods to boost positive emotions and reduce negative ones.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Why carry out this study? |
Chronic pain is a significant public health issue, affecting millions of individuals and imposing a substantial economic burden due to healthcare costs and lost productivity. Understanding the modulation of pain by emotional states can help in developing more effective pain management strategies. |
While the relationship between anxiety and pain modulation has been studied, the effects of other emotional states on pain modulation remain underexplored, necessitating further research. |
The study hypothesized that different emotional states (happiness, anger, sadness, and interest) would have distinct effects on endogenous pain modulation, as measured by conditioned pain modulation (CPM) and the wind-up phenomenon. |
What was learned from the study? |
The study found significant changes in CPM for sadness, happiness, and anger, but not for interest. Specifically, sadness and anger decreased CPM, while happiness increased it. |
No significant effects were observed on the wind-up phenomenon across any of the emotional states. |
The study concluded that emotional states significantly affect endogenous pain modulation. Specifically, sadness and anger decreased CPM, while happiness increased it. |
The findings suggest that emotional states can significantly influence endogenous pain modulation. Positive emotions like happiness can enhance pain inhibition, while negative emotions like sadness and anger can impair it. This highlights the potential for integrating emotional modulation techniques into pain management strategies. |
Introduction
Endogenous pain modulation refers to the capacity of the central nervous system to regulate the transmission of pain signals originating from nociceptors to the central nervous system. This can be achieved through either endogenous pain amplification or inhibition. To obtain comprehensive information about this influence, quantitative sensory testing paradigms have been devised.
The inhibition of wide dynamic range neurons causes regulation of pain impulses at spinal cord level via descending pain pathways representing the body’s own pain inhibition [35]. The function of this system can be determined through the use of conditioned pain modulation (CPM) [25]. CPM is defined as a decrease in the response to a painful stimulus after application of a second painful stimulus on remote body areas in comparison to the baseline response. The test stimulus (TS) is applied as baseline; then a second painful stimulus, referred to as the conditioning stimulus (CS), is applied. The TS is then applied once more and compared to the baseline response. The difference between both measurements corresponds to the activity of the endogenous inhibitory system [21].
The body’s own pain amplification process is regulated by central mechanisms. The consistent input from polymodal C-fiber nociceptors leads to the sensitization of dorsal horn neurons [20]. The phenomenon of temporal summation results in a persistent increase in pain perception when a sequence of identical nociceptive stimuli is administered [18]. In clinical settings, this effect is quantified by assessing the “wind-up” phenomenon [17].
It has been hypothesized that one’s emotional state may have an impact on endogenous pain modulation. The negative relationship between anxiety and CPM has been previously examined in a comprehensive review by Wiech and Tracey [45]. Furthermore, it has been demonstrated that anxiety is associated with increased temporal summation [37]. Threat on the other hand did not affect CPM [19]. However, research has not yet explored the correlation between other emotions and these phenomena.
Russell introduced the core affect model, which categorizes emotions on the basis of their positive or negative valence or intensity [39]. Zupan and Eskritt applied this categorization to assign the basic emotions described by Ekman [9, 50]. In addition, they assigned the state “interest” to the quadrant of positive emotions with low intensity (Fig. 1).

Examples from the Russel model, modified according to Zupan [50]
Watching video clips has proven to be a reliable method for inducing a range of emotions. In a study conducted by Zupan and Eskritt a total of 50 film clips were selected and presented to 113 participants for evaluation based on the emotions they elicited [50]. The impact of these emotionally induced states on the activity of the autonomic nervous system was assessed using psychophysiological measurements, such as recording heart rate variability and measuring skin conductance. Alterations in these parameters can be considered evidence of successful emotion induction.
The objective of this study is to evaluate the impact of various emotions on endogenous pain modulation.
Methodology
This study was conducted at the Medical University of Graz in a randomized controlled, cross-over design. The course of the study is shown in Fig. 2.

Flowchart of the study
The institutional review board of the Medical University of Graz approved the study protocol (Ethics committee’s number 34-298 ex 21/22). The study followed all Austrian and European laws and regulations, including the Helsinki Declaration. Participants provided their consent by signing a written informed consent form.
Recruitment of healthy individuals aged 18–60 years was accomplished through the posting of announcements on public notice boards. For respondents, further information was provided by a specialist in anesthesiology and intensive care medicine who was participating in the study. Participants received no financial or other compensation. Exclusion criteria were defined as history of psychiatric illnesses, history of vascular disease, and chronic pain disorders. Likewise, the intake of analgesics, anti-neuropathic drugs, and/or antidepressants were exclusion criteria.
Interventions
On the basis of a computer-generated randomization list sourced from randomization.com, four film clips were presented in a specific order to each participant. Participants were not informed about the anticipated impact of the videos on their emotional states. In a controlled environment without any external audiovisual disturbances, the four video clips were presented to the participants on a monitor.
Sequences from the following films are used to induce emotions [50]: for the emotion happiness, a sequence from the movie “Lottery Ticket” is shown, for anger from the movie “Enough”, for interest from the movie “National Treasure”, and for sadness from the movie “Slumdog Millionaire” (Table 1). After each video clip, outcomes were assessed. Afterwards, a neutral video clip with a calm nature shot was shown for 30 s to reduce potential carryover effects [11]. As in the Zupan study, participants were not asked if they knew the original movies [50].
Initial Examination
Participants were requested to fill out a questionnaire that includes information on their demographic background. Patients were asked about any acute or chronic pain, and the consumption of analgesics or co-analgetic drugs, including antidepressants or gabapentinoids. The Central Sensitization Inventory (CSI) [27] was administered once to evaluate any changes in the sense of central sensitization. In order to ensure we only included healthy volunteers, participants with an increased CSI score were excluded from the study. The Short Suggestibility Scale (SSS) was included into the trial to measure an individual’s ability to respond to suggestions [24].
Central Sensitization Inventory
The CSI is a self-administered assessment instrument, designed to evaluate the presence and severity of central sensitization symptoms. It comprises a total of 35 questions. The score, which ranges from 0 to 100, reflects the extent of symptoms indicative of central sensitization. A higher score indicates a greater degree of symptoms [27]. The CSI was used to ensure that there was no central sensitization in the volunteers before inclusion. A cutoff value of 40 was defined according to previous literature [33].
Short Suggestibility Scale
The SSS is the short form of the multidimensional Iowa Suggestibility Scale and assesses susceptibility to the acceptance and internalization of external influences. The scale consists of 21 items, which are divided into the following categories: consumer suggestibility, persuasibility, sensation contagion, physiological reactivity, and peer conformity [24].
Outcome Parameter
The outcome parameters were assessed as baseline measurement before the first video clip, and after every clip in a predefined sequence: Subjective self-assessment, CPM, wind-up.
Self-Assessment
The subjective self-assessment of affect was rated using a 7-point Likert scale from 1 “not at all” to 7 “very strongly” for the three emotions and general arousal. Participants were asked to rate their current emotional state for each emotion and arousal before and after each video clip. Higher values correspond to higher intensity of emotions. The higher the value, the more intensely the emotion was perceived [16].
Conditioned Pain Modulation
The approach outlined by Mertens et al. served as a standard for assessing CPM [29]. The conditioning stimulus in this case is a hot water bath. To facilitate habituation, the non-dominant hand is initially immersed in a water bath at a temperature of 37 °C for a period of 10 s. This is succeeded by a bath at 46 °C for a duration of 2 min. The test stimulus is pressure pain tolerance (PPT, kg/m2). This is measured before and at the end of the heat exposure using a pressure algometer on the adductor pollicis brevis muscle of the dominant hand. The relative CPM effect is calculated as follows [29]:
(PPTbefore heat − PPTafter heat)/PPTbefore heat.
Wind-up
Pin prick needle stimulators with an intensity of 256 mN were utilized to determine the wind-up phenomenon. The sensitivity of the skin on the ball of the thumb to a single stimulus is compared with sensitivity to a series of stimuli (10 needle stimuli). Stimulation is performed at a stimulation frequency of 1 Hz. The participant assesses the applied stimuli, both the single stimulus and the entire stimulus series, using a visual analog scale (VAS 0–100). The wind-up quotient is calculated from the ratio of the perceived pain intensity over the series of stimuli divided by the pain intensity after the single stimulus [31].
Sample Size and Statistical Analysis
As the current literature did not allow one to draw conclusions about the expected effect of the different stimuli on the main target variable, a sample size of 25 test subjects was defined for the present study. Significance level was defined at 0.05.
The differences between pre and post were expressed by percentage points or difference of the wind-up ratio. After normality was evaluated using the Kolmogorov–Smirnov test, pre and post measurements were compared by t test for paired samples. The Pearson R was calculated for evaluating correlations.
Results
Between July 2022 and February 2023, a total of 28 participants were included in the study (13 men and 15 women). All participants completed the study according to the protocol. Participants’ characteristics are presented in Table 2.
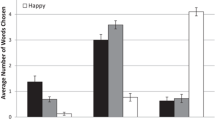
Significant differences in emotional self-assessment values were observed before and after viewing the video clips. The self-assessment value for sadness increased from 1.4 ± 0.9 to 2.6 ± 1.1 (p = 0.00001), happiness scores increased from 4.5 ± 1.6 to 5.3 ± 1.3 (p = 0.00006), anger scores increased from 1.2 ± 0.6 to 4.0 ± 1.8 (p = 0.00001), and interest scores increased from 1.0 ± 0 to 3.25 ± 1.6 (p = 0.00001).
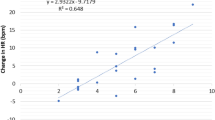
Table 3 presents the main results. Significant changes in CPM for sadness, happiness, and anger, but no significant changes for interest. Specifically, the CPM mean difference pre/post for sadness was − 9.9 ± 23.1 (p = 0.03211), for happiness it was 4.57 ± 11.4 (p = 0.04277), for anger it was − 9.1 ± 23.3 (p = 0.04804), and for interest it was − 5.1 ± 25.8 (p = 0.31042).
Furthermore, there were no significant effects observed on the wind-up phenomenon across any of the emotional states. The wind-up mean difference pre/post for sadness was − 0.089 ± 0.817 (p = 0.56792), for happiness was − 0.303 ± 0.809 (p = 0.05731), for anger was − 0.1964 ± 0.774 (p = 0.19041), and for interest was − 0.0893 ± 0.667 (p = 0.48508).
The Pearson correlation coefficient between the CPM and the wind-up mean difference pre/post and the SSS was R < 0.2 for both parameters and all emotions, indicating a weak correlation. Additionally, when potential gender effects were analyzed, no significant differences were found in either CPM or wind-up for any of the four emotions.
Discussion
Emotions and pain are related in a complex, bidirectional relationship. Despite clear conceptional and functional overlaps, research on their interaction is still limited [14]. Emotional experiences were shown to modulate pain perception [15]. On the other hand, anhedonia is highly prevalent in individuals with chronic pain [13]. Additionally, factors such as exercise, stress, and cognitive strategies can further modulate pain perception [43]. Recent studies confirmed the pivotal role of the amygdala in both emotion and pain processing [28].
Our data demonstrate that short-term alterations of emotions are capable of influencing endogenous pain modulation. Furthermore, we concentrated on two central mechanisms in pain processing: CPM and wind-up.
CPM describes a “pain inhibits pain” phenomenon, where a spatially remote painful stimulus (conditioning stimulus) changes the perceived intensity of a test stimulus. Although traditionally regarded as measure for the descending inhibitory system, recent research has shown that propriospinal processes may also be involved [32]. However, it is still one of the pivotal tests to assess the effectiveness of the physiological pain inhibition [41].
The wind-up phenomenon refers to the progressive increase in pain intensity with repeated stimulation at a constant intensity. This phenomenon is primarily attributed to the activation of N-methyl-d-aspartate (NMDA) receptors in the spinal cord, leading to a heightened response to peripheral nociceptive inputs. It is a pivotal concept in pain medicine as it contributes to the maintenance of pain states [7].
Our data showed that emotions influence CPM. For wind-up, we could, however, not show a significant effect. Previous research showed that patients with chronic affective disorders show reduced CPM [32]. Furthermore, the effect of antidepressants on pain was shown to correlate with CPM [48]. This effect is achieved by increasing 5-HT in synaptic junctions [42]. Our data not only confirms these findings in a healthy population but also shows that the effect is not only valid for emotions with a negative valence; happiness, as an emotion with positive valence, was shown to have a pronounced effect in the other direction. This suggests that in the context of pain medicine, not only should negative emotions be avoided or treated but that positive emotions can also be used to prevent or even treat pain.
The effect of anger on pain perception is complex. Multiple studies have examined the influence of anger induction on pain sensitivity in individuals with pain conditions or in healthy individuals. These studies have consistently observed an increased responsiveness to experimental pain stimulation [3, 44]. Additionally, the way in which anger is managed can potentially affect an individual’s sensitivity to pain. Specifically, individuals who are more inclined to express anger through physical or verbal means (referred to as the anger-out style) exhibit heightened sensitivity. This has been observed in the context of both experimental pain and acute postsurgical pain [1, 4, 34]. Endogenous opioids were shown to play a role [5].
In contrast to anger, the literature for the effect of sadness on pain is still very limited. Especially in chronic conditions, there is frequently an imprecise distinction with depression [2]. Acute sadness increases the intensity of experimentally induced pain in both healthy volunteers and patients with pain chronification [44, 49]. These findings could be correlated to changes in the cortical oscillation in the electroencephalogram (EEG).
Until now, there were no reports on the effect of these two negative emotions on CPM. We could show that anger and sadness both reduce the effect of CPM.
Although the impact of positive emotions on pain has not been investigated as frequently as negative emotions, several studies have demonstrated their capacity to mitigate discomfort [12]. Both supraspinal modulation and descending pain modulation are believed to play a role, as indicated by a decrease in the spinal nociceptive reflex following positive emotion induction [36, 38, 46]. This may contribute to the positive effect of happiness on CPM in our sample.
Attention and nociception are inherently interconnected and possess a reciprocal relationship with one another [30]. Pain has the capacity to captivate attention involuntarily, especially when it is severe, novel, or menacing [26]. Conversely, directing attention away from pain can prevent its further processing and result an analgetic effect [22]. However, our results showed that this does not result in a reduced CPM. One could argue that the application of the conditioning stimulus causes the attention that was previously focused on the content of the movie to be shifted to the pain. Compared to the induced emotions, interest may be less stable.
Yarnitsky introduced a concept of profiling pain modulation by psychophysiological testing based on CPM and temporal summation [47, 48]. Both a less efficient pain inhibition and an enhanced facilitation may result in pronociceptive states. In our experiments, wind-up was not significantly affected. Therefore, one can conclude that negative emotions promote a pain modulation profile of inhibitory nociception (i.e., normal temporal summation and impaired CPM).
Limitations
Our study has several limitations that warrant consideration. Firstly, the emotional effects induced by the movie clips were relatively mild. Various methods for the induction of emotions are described [23]. Video clips combine visual and auditive signals, and are therefore regarded as potent inductors [40]. A meta-analysis confirmed that video clips have a large effect in inducing emotions, which is even more pronounced in negative affect [10]. By assessing self-reported affect, we could demonstrate that the video clips achieved significant alterations to the emotional state. The effect in our sample, however, was only mild. Nevertheless, it was intense enough to cause a change in endogenous pain modulation.
Additionally, the sample size was small, with only 28 participants. This limited sample size reduces the statistical power of our findings and may impact the generalizability of the results. A larger sample size would provide more robust data and improve the reliability of the conclusions drawn.
Age could be a potential confounder in emotional response. However, the age range of our sample was comparable to the Zupan study [50]. We therefore do not suppose that there may be a negative influence of age on the validity of the emotional inductions.
Individuals may experience different emotional reactions to the same clip, which may be influenced by life events. The current study did not exclude or evaluate any potentially triggering content.
Additionally, our study focused on only four emotions: happiness, anger, sadness, and interest. This limited range may not capture the full spectrum of emotional influences on pain modulation. Future research should explore a broader array of emotions, including fear, disgust, and surprise, to provide a more comprehensive understanding of the relationship between emotions and pain modulation. Finally, the correlation between the wind-up phenomenon and the SSS was weak, suggesting that suggestibility may not significantly impact wind-up. Further research is needed to explore this relationship and to evaluate the appropriateness of using the SSS in this context.
Clinical Application
From our data we can derive two hypotheses for clinical application: as video clips that induce happiness are effectively reducing pain, we propose they should be promoted as tools for painful procedures. However, prior attempts to present videos in acute pain situation showed mixed results [6, 8]. Unfortunately, in these studies there was no focus on the emotional component, as videos were primarily used as a distraction. As we have shown, inducing interest is not enough to influence pain perception in a relevant magnitude. Our data suggest that such studies could achieve even better results with video clips that induce happiness.
Moreover, negative emotions can alter central modulation of pain and result in increased pain perception. Therefore, more attention should be paid to avoiding negative emotions in acute pain situations.
Conclusion
Our data show that the induction of emotions affects pain. Happiness increased CPM, while anger and sadness decreased it. Interest did not alter CPM. Therefore, the valence of emotion has a direct influence on the amount of CPM.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Adachi T, Yamada K, Fujino H, et al. Associations between anger and chronic primary pain: a systematic review and meta-analysis. Scand J Pain. 2022;22:1–13.
Bondolfi G, Mazzola V, Arciero G. In between ordinary sadness and clinical depression. Emot Rev. 2015;7:216–22.
Bruehl S, Burns JW, Chung OY, et al. Anger and pain sensitivity in chronic low back pain patients and pain-free controls: the role of endogenous opioids. Pain. 2002;99:223–33.
Bruehl S, Chung OY, Donahue BS, et al. Anger regulation style, postoperative pain, and relationship to the A118G mu opioid receptor gene polymorphism: a preliminary study. J Behav Med. 2006;29:161–9.
Burns JW, Bruehl S, Chont M. Anger regulation style, anger arousal and acute pain sensitivity: evidence for an endogenous opioid “triggering” model. J Behav Med. 2014;37:642–53.
Chuan A, Zhou JJ, Hou RM, et al. Virtual reality for acute and chronic pain management in adult patients: a narrative review. Anaesthesia. 2021;76:695–704.
Curatolo M. central sensitization and pain: pathophysiologic and clinical insights. Curr Neuropharmacol. 2024;22:15–22.
Demirci H, Van Der Storm SL, Huizing NJ, et al. Watching a movie or listening to music is effective in managing perioperative anxiety and pain: a randomised controlled trial. Knee Surg Sports Traumatol Arthrosc. 2023;31:6069–79.
Ekman P. Basic emotions. In: Dalgleish T, Power M, editors. Handbook of cognition and emotion New York: Wiley; 1999. p. 45–60.
Fernández-Aguilar L, Navarro-Bravo B, Ricarte J, et al. How effective are films in inducing positive and negative emotional states? A meta-analysis. PLoS ONE. 2019;14:e0225040.
Fernández-Aguilar L, Ricarte J, Ros L, et al. Emotional differences in young and older adults: films as mood induction procedure. Front Psychol. 2018. https://doi.org/10.3389/fpsyg.2018.01110.
Finan PH, Garland EL. The role of positive affect in pain and its treatment. Clin J Pain. 2015;31:177–87.
Garland EL, Trøstheim M, Eikemo M, et al. Anhedonia in chronic pain and prescription opioid misuse. Psychol Med. 2020;50:1977–88.
Gilam G, Gross JJ, Wager TD, et al. What is the relationship between pain and emotion? Bridging constructs and communities. Neuron. 2020;107:17–21.
Godinho F, Magnin M, Frot M, et al. Emotional modulation of pain: is it the sensation or what we recall? J Neurosci. 2006;26:11454–61.
Harland NJ, Dawkin MJ, Martin D. Relative utility of a visual analogue scale vs. a six-point Likert scale in the measurement of global subject outcome in patients with low back pain receiving physiotherapy. Physiotherapy. 2015;101:50–4.
Herrero JF, Laird JM, López-García JA. Wind-up of spinal cord neurones and pain sensation: much ado about something? Prog Neurobiol. 2000;61:169–203.
Horn-Hofmann C, Capito ES, Wolstein J, et al. Acute alcohol effects on conditioned pain modulation, but not temporal summation of pain. Pain. 2019;160:2063–71.
Horn-Hofmann C, Jablonowski L, Madden M, et al. Is conditioned pain modulation (CPM) affected by negative emotional state? Eur J Pain. 2024;28:421–33.
Horn-Hofmann C, Kunz M, Madden M, et al. Interactive effects of conditioned pain modulation and temporal summation of pain-the role of stimulus modality. Pain. 2018;159:2641–8.
Horn-Hofmann C, Priebe JA, Schaller J, et al. Lack of predictive power of trait fear and anxiety for conditioned pain modulation (CPM). Exp Brain Res. 2016;234:3649–58.
Johnson MH. How does distraction work in the management of pain? Curr Pain Headache Rep. 2005;9:90–5.
Joseph DL, Chan MY, Heintzelman SJ, et al. The manipulation of affect: a meta-analysis of affect induction procedures. Psychol Bull. 2020;146:355–75.
Kotov R, Bellman S, Watson D. MISS: multidimensional iowa suggestibility scale brief manual. 2004. Stony Brook: Stony Brook University. https://renaissance.stonybrookmedicine.edu/sites/default/files/MISSBriefManual.pdf. Accessed 26 Apr 2016.
Le Bars D. The whole body receptive field of dorsal horn multireceptive neurones. Brain Res Brain Res Rev. 2002;40:29–44.
Legrain V, Van Damme S, Eccleston C, et al. A neurocognitive model of attention to pain: behavioral and neuroimaging evidence. Pain. 2009;144:230–2.
Mayer TG, Neblett R, Cohen H, et al. The development and psychometric validation of the central sensitization inventory. Pain Pract. 2012;12:276–85.
Mazzitelli M, Ponomareva O, Presto P, et al. Impaired amygdala astrocytic signaling worsens neuropathic pain-associated neuronal functions and behaviors. Front Pharmacol. 2024;15:1368634.
Mertens MG, Hermans L, Crombez G, et al. Comparison of five conditioned pain modulation paradigms and influencing personal factors in healthy adults. Eur J Pain. 2021;25:243–56.
Moriarty O, Mcguire BE, Finn DP. The effect of pain on cognitive function: a review of clinical and preclinical research. Prog Neurobiol. 2011;93:385–404.
Mücke M, Cuhls H, Radbruch L, et al. Quantitative sensory testing. Schmerz. 2014;28:635–46.
Nahman-Averbuch H, Piché M, Bannister K, et al. Involvement of propriospinal processes in conditioned pain modulation. Pain. 2024. https://doi.org/10.1097/j.pain.0000000000003217.
Neblett R, Cohen H, Choi Y, et al. The Central Sensitization Inventory (CSI): establishing clinically significant values for identifying central sensitivity syndromes in an outpatient chronic pain sample. J Pain. 2013;14:438–45.
Peters ML. Emotional and cognitive influences on pain experience. Mod Trends Pharmacopsychiatry. 2015;30:138–52.
Ramaswamy S, Wodehouse T. Conditioned pain modulation-A comprehensive review. Neurophysiol Clin. 2021;51:197–208.
Rhudy JL, Williams AE, Mccabe KM, et al. Affective modulation of nociception at spinal and supraspinal levels. Psychophysiology. 2005;42:579–87.
Robinson ME, Bialosky JE, Bishop MD, et al. Supra-threshold scaling, temporal summation, and after-sensation: relationships to each other and anxiety/fear. J Pain Res. 2010;3:25–32.
Roy M, Piché M, Chen J-I, et al. Cerebral and spinal modulation of pain by emotions. Proc Natl Acad Sci. 2009;106:20900–5.
Russell JA. Core affect and the psychological construction of emotion. Psychol Rev. 2003;110:145–72.
Siedlecka E, Denson TF. Experimental methods for inducing basic emotions: a qualitative review. Emot Rev. 2019;11:87–97.
Sirucek L, Ganley RP, Zeilhofer HU, et al. Diffuse noxious inhibitory controls and conditioned pain modulation: a shared neurobiology within the descending pain inhibitory system? Pain. 2023;164:463–8.
Tao Z-Y, Wang P-X, Wei S-Q, et al. The role of descending pain modulation in chronic primary pain: potential application of drugs targeting serotonergic system. Neural Plast. 2019;2019:1389296.
Vaegter HB, Fehrmann E, Gajsar H, et al. Endogenous modulation of pain. Clin J Pain. 2019;36:150–61.
Van Middendorp H, Lumley MA, Jacobs JW, et al. The effects of anger and sadness on clinical pain reports and experimentally-induced pain thresholds in women with and without fibromyalgia. Arthritis Care Res. 2010;62:1370–6.
Wiech K, Tracey I. The influence of negative emotions on pain: behavioral effects and neural mechanisms. Neuroimage. 2009;47:987–94.
Williams AE, Rhudy JL. Affective modulation of eyeblink reactions to noxious sural nerve stimulation: a supraspinal measure of nociceptive reactivity? Int J Psychophysiol. 2007;66:255–65.
Yarnitsky D. Role of endogenous pain modulation in chronic pain mechanisms and treatment. Pain. 2015;156:S24–31.
Yarnitsky D, Granot M, Nahman-Averbuch H, et al. Conditioned pain modulation predicts duloxetine efficacy in painful diabetic neuropathy. Pain. 2012;153:1193–8.
Yoshino A, Okamoto Y, Yoshimura S, et al. Distinctive neural responses to pain stimuli during induced sadness in patients with somatoform pain disorder: an fMRI study. NeuroImage Clin. 2013;2:782–9.
Zupan B, Eskritt M. Eliciting emotion ratings for a set of film clips: a preliminary archive for research in emotion. J Soc Psychol. 2020;160:768–89.
Acknowledgements
We thank the participants of the study.
Funding
No funding or sponsorship was received for this study or publication of this article.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by K. Lang-Illievich, C. Klivinyi, J. Ranftl, A. Elhelali, S. Hammer, I.S. Szilagyi, and H. Bornemann-Cimenti. The first draft of the manuscript was written by K. Lang-Illievich and H. Bornemann-Cimenti and all authors commented and contributed to the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
Helmar Bornemann-Cimenti is an Editorial Board member of Pain and Therapy. Helmar Bornemann-Cimenti was not involved in the selection of peer reviewers for the manuscript nor any of the subsequent editorial decisions. All other authors (Kordula Lang-Illievich, Christoph Klivinyi, Julia Ranftl, Ala Elhelali, Sascha Hammer and Istvan S. Szilagyi) declare that they have nothing to disclose.
Ethical Approval
The institutional review board of the Medical University of Graz approved the study protocol (Ethics committee’s number 34-298 ex 21/22). The study followed all Austrian and European laws and regulations, including the Helsinki Declaration. Participants provided their consent by signing a written informed consent form.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Lang-Illievich, K., Klivinyi, C., Ranftl, J. et al. Change in Endogenous Pain Modulation Depending on Emotional States in Healthy Subjects: A Randomized Controlled Trial. Pain Ther (2024). https://doi.org/10.1007/s40122-024-00642-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40122-024-00642-1