
Abstract
Immunoglobulin G (IgG) nephropathy refers to a rare group of diseases characterized by deposits of IgG in the mesangial region. However, IgG nephropathy is controversial as a single disease entity, and its pathogenesis remains to be elucidated. In the present report, we discuss a case of IgG nephropathy in which we observed activation of the classical complement pathway.
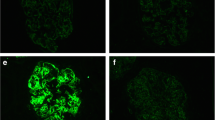
A 47-year-old woman was admitted to our hospital with nephrotic syndrome. Light-microscopic examination revealed neither proliferative nor sclerotic lesions in the glomeruli. However, unusual and large deposits were observed in the paramesangial area. An immunofluorescence study revealed predominant IgG and C1q and slight C3 deposits in the paramesangial area, suggesting immune-complex-type glomerular disease. An electron microscopic study also revealed different sizes of non-organized electron-dense deposits with a similar pattern of distribution, which were accompanied by foot process effacement. Clinically, there was no evidence of systemic diseases, such as infectious or autoimmune diseases (including systemic lupus erythematosus). Based on these findings, she was diagnosed with IgG nephropathy and treated with prednisolone. Steroid therapy was effective, and complete remission was maintained.
Additional immunological examination revealed that IgG deposits were polyclonal and consisted mainly of the IgG1 and IgG3 subclasses. Furthermore, staining was positive for C4d and C5b-9. The present findings indicate that the pathogenesis of IgG nephropathy in our patient may have involved activation of the classical complement pathway.




Similar content being viewed by others


Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Sato M, Kojima H, Nabeshima K, Nakajima Y, Koshikawa S. Primary glomerulonephritis with predominant mesangial immunoglobulin G deposits–a distinct entity? Nephron. 1993;64:122–8.
Yoshikawa N, Iijima K, Shimomura M, Nakamura H, Ito H. IgG-associated primary glomerulonephritis in children. Clin Nephrol. 1994;42:281–7.
Kano K, Ueda Y, Iidaka K, Ichimura T. Glomerulonephritis with predominant paramesangial IgG deposition. Pathol Int. 1996;46:306–9.
Fakhouri F, Darré S, Droz D, Lemaire M, Nabarra B, Machet MC, Chauveau D, Lesavre P, Grünfeld JP, Noël LH, Knebelmann B. Mesangial IgG glomerulonephritis: a distinct type of primary glomerulonephritis. J Am Soc Nephrol. 2002;13:379–87.
Jourde-Chiche N, Moal V, Daniel L, Purgus R, Legis T Jr, Vacher-Coponat H, Moussi-Frances J, Berland Y. Early IgG glomerulonephritis recurrence in a kidney transplant recipient. Clin Nephrol. 2008;70:340–3.
Huerta A, Bomback AS, Liakopoulos V, Palanisamy A, Stokes MB, D’Agati VD, Radhakrishnan J, Markowitz GS, Appel GB. Renal-limited “lupus-like” nephritis. Nephrol Dial Transplant. 2012;27:2337–42.
Lim BJ, Hong SW, Jeong HJ. IgG nephropathy - confusion and overlap with C1q nephropathy. Clin Nephrol. 2009;72:360–5.
Jennette JC, Hipp CG. C1q nephropathy: a distinct pathologic entity usually causing nephrotic syndrome. Am J Kidney Dis. 1985;6:103–10.
Mii A, Shimizu A, Masuda Y, Fujita E, Aki K, Ishizaki M, Sato S, Griesemer A, Fukuda Y. Current status and issues of C1q nephropathy. Clin Exp Nephrol. 2009;13:263–74.
Lau KK, Gaber LW, Delos Santos NM, Wyatt RJ. C1q nephropathy: features at presentation and outcome. Pediatr Nephrol. 2005;20:744–9.
Fukuma Y, Hisano S, Segawa Y, Niimi K, Tsuru N, Kaku Y, Hatae K, Kiyoshi Y, Mitsudome A, Iwasaki H. Clinicopathologic correlation of C1q nephropathy in children. Am J Kidney Dis. 2006;47:412–8.
Markowitz GS, Schwimmer JA, Stokes MB, Nasr S, Seigle RL, Valeri AM, D’Agati VD. C1q nephropathy: a variant of focal segmental glomerulosclerosis. Kidney Int. 2003;64:1232–40.
Hisano S, Fukuma Y, Segawa Y, Niimi K, Kaku Y, Hatae K, Saitoh T, Takeshita M, Iwasaki H. Clinicopathologic correlation and outcome of C1q nephropathy. Clin J Am Soc Nephrol. 2008;3:1637–43.
Onitsuka S, Tanabe K, Toma H, Yamaguchi Y. Mesangial proliferative glomerulonephritis with predominant mesangial IgG deposition in renal allograft. Nephron. 2000;86:404–6.
Jalalah SM. IgG glomerulonephritis: a morphologic study of a rare entity. Saudi J Kidney Dis Transpl. 2009;20:798–801.
Iskandar SS, Browning MC, Lorentz WB. C1q nephropathy: a pediatric clinicopathologic study. Am J Kidney Dis. 1991;18:459–65.
Fogo AB, Lusco MA, Najafian B, Alpers CE. AJKD atlas of renal pathology: C1q nephropathy. Am J Kidney Dis. 2015;66:e13-4.
van de Lest NA, Zandbergen M, Wolterbeek R, Kreutz R, Trouw LA, Dorresteijn EM, Bruijn JA, Bajema IM, Scharpfenecker M, Chua JS. Glomerular C4d deposition can precede the development of focal segmental glomerulosclerosis. Kidney Int. 2019;96:738–49.
Drachenberg CB, Papadimitriou JC, Chandra P, Haririan A, Mendley S, Weir MR, Rubin MF. Epidemiology and pathophysiology of glomerular C4d staining in native kidney biopsies. Kidney Int Rep. 2019;4:1555–67.
Cooper NR. The classical complement pathway: activation and regulation of the first complement component. Adv Immunol. 1985;37:151–216.
Vidarsson G, Dekkers G, Rispens T. IgG subclasses and allotypes: from structure to effector functions. Front Immunol. 2014;5:520.
Pickering WP, Bailey RR, Gardner J. IgG nephropathy: an uncommon form of primary glomerulonephritis? N Z Med J. 1996;109:365.
Sepandj F, McFarlane C, Trillo A. Nephrotic syndrome secondary to primary immunoglobulin-G mesangioproliferative glomerulonephritis. Nephrol Dial Transplant. 1998;13:1889–90.
Assadi FK. IgG-associated mesangial glomerulonephritis in a patient with Down syndrome. Med Sci Monit. 2004;10:CS54-6.
Kharroubi M, Ben Fatma L, Rais L, Jebali H, Mami I, Zouaghi MK. Primary glomerulonephritis with predominant mesangial Immunoglobulin G deposits. Tunis Med. 2018;96:442–4.
Acknowledgements
We thank Ms. Arimi Ishikawa and Ms. Asae Kurosawa for their technical assistance.
Funding
No funding to declare.
Author information
Authors and Affiliations
Contributions
MA, HA, TK, AM, and YS treated the patient and evaluated the clinical images. AM and AS were responsible for the pathological diagnosis. MA, AM, and TK contributed to clinical data acquisition. MA, AM, and AS interpreted the data and prepared the manuscript. All authors read and approved the final version of this manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no conflict of interest exists.
Ethical approval
No experimental study was conducted. All procedures performed in this case were in accordance with the ethical standards of the institutional committee and with the 1975 Helsinki declaration and its later amendments or comparable ethical standards.
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. This work does not contain any studies with animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Arai, M., Mii, A., Hirama, A. et al. A possible role of classical complement pathway activation in the pathogenesis of immunoglobulin G nephropathy: a case report. CEN Case Rep 12, 14–22 (2023). https://doi.org/10.1007/s13730-022-00710-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13730-022-00710-5