
Abstract
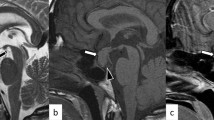
A 57-year-old woman with pre-dialysis chronic kidney disease (CKD) was hospitalized because of fever and fatigue. On admission, increased inflammatory response and pyuria with bacteriuria were observed. Pyelonephritis was successfully treated with antibiotics, whereas her fatigue continued and she developed progressive hypercalcemia and hyponatremia; serum sodium level, 116 mEq/L and corrected serum calcium level, 13.4 mg/dL. Plasma concentrations of adrenocorticotropic hormone and cortisol and serum luteinizing hormone were under the detection level. Although the reaction of other anterior pituitary hormones and the serum antidiuretic hormone (ADH) was preserved, the response of serum luteinizing hormone to administration of luteinizing hormone releasing hormone was impaired. Magnetic resonance imaging showed no structural abnormality in the thalamus, hypothalamus, and pituitary gland. She was diagnosed with adrenal insufficiency caused by partial hypopituitarism in concomitant with pyelonephritis. After starting hydrocortisone replacement, serum levels of sodium and calcium were rapidly normalized. This case highlights the importance of adrenal insufficiency as a differential diagnosis of hypercalcemia in patients with pre-dialysis CKD, especially when hyponatremia was concomitantly observed. Besides, infection should be considered as an important trigger for the development of latent adrenal insufficiency since it could increase the physiological demand of corticosteroid in the body. Also, CKD may enhance the magnitude of hypercalcemia since CKD patients have decreased capacity to increase urinary calcium excretion.


Similar content being viewed by others

References
Assadi F. Hypercalcemia: an evidence-based approach to clinical cases. UJKD. 2009;3:71–9.
Carroll R, Matfin G. Endocrine and metabolic emergencies: hypercalcaemia. Ther Adv Endocrinol Metab. 2010;1:225–34.
Ziegler R. Hypercalcemic crisis. J Am Soc Nephrol. 2001;12(Suppl 17):3–9.
Martin KJ, González EA. Prevention and control of phosphate retention/hyperphosphatemia in CKD-MBD: what is normal, when to start, and how to treat? Clin J Am Soc Nephrol. 2011;6:440–6.
Goldsmith DJ, Massy ZA, Brandenburg V. The uses and abuses of vitamin D compounds in chronic kidney disease-mineral bone disease (CKD-MBD). Semin Nephrol. 2014;34:660–8.
Lunn MR, Muñoz Mendoza J, Pasche LJ, Norton JA, Ayco AL, Chertow GM. Hyperparathyroidism with hypercalcaemia in chronic kidney disease: primary or tertiary? NDT Plus. 2010;3:366–71.
Yamada S, Tsujikawa H, Eriguchi M, Taniguchi M, Tsuruya K. Hypercalcemia and large abdominal mass. NDT Plus. 2011;4:213–4.
Lemley KV. An unusual case of hypercalcemia in a patient with renal insufficiency. Pediatr Nephrol. 2014;29:1529–33.
Downie WW, Gunn A, Paterson CR. Howie GF. Hypercalcaemic crisis as presentation of Addison’s disease. Br Med J. 1977;1:145–6.
Fujikawa M, Kamihira K, Sato K, Okamura K, Kidota S, Lida M. Elevated bone resorption markers in a patient with hypercalcemia associated with post-partum thyrotoxicosis and hypoadrenocorticism due to pituitary failure. J Endocrinol Invest. 2004;27:782–7.
Kato A, Shinozaki S, Goga T, Hishida A. Isolated adrenocorticotropic hormone deficiency presenting with hypercalcemia in a patient on long-term hemodialysis. Am J Kidney Dis. 2003;42:E32-6.
Neary X, Neiman N. L. Adrenal insufficiency, etiology, diagnosis and treatment. Curr Opin Endocrionol Diabetes Obes. 2010;17:217–23.
Cuesta M, Garrahy A, Slattery D, Gupta S, Hannon AM, Forde H, McGurren K, Sherlock M, Tormey W, Thompson CJ. The contribution of undiagnosed adrenal insufficiency to euvolaemic hyponatraemia: results of a large prospective single-centre study. Clin Endocrinol (Oxf). 2016;85:836–44.
Ascoli P, Cavagnini F, Hypopituitarism. Pituitary. 2006;9:335–42.
Andrioli M, Pecori Giraldi F, Cavagnini F. Isolated corticotrophin deficiency. Pituitary. 2006;9:289–95.
Rushworth RL, Torpy DJ. A descriptive study of adrenal crises in adults with adrenal insufficiency: increased risk with age and in those with bacterial infections. BMC Endocr Disord. 2014;14:79.
Fernandez-Rodriguez E, Bernabeu I, Andujar-Plata P, Casanueva FF. Subclinical hypopituitarism. Best Pract Res Clin Endocrinol Metab. 2012;26:461–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All the authors declare no competing interest.
Human and animal rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
A written informed consent was obtained from the patient included in this case study.
About this article

Cite this article
Yamada, S., Arase, H., Morishita, T. et al. Adrenal crisis presented as acute onset of hypercalcemia and hyponatremia triggered by acute pyelonephritis in a patient with partial hypopituitarism and pre-dialysis chronic kidney disease. CEN Case Rep 8, 83–88 (2019). https://doi.org/10.1007/s13730-018-0371-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13730-018-0371-9