
Abstract
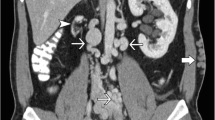
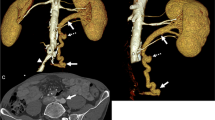
Renal vein thrombosis in a transplanted kidney is an uncommon but critical complication that can result in graft loss if management is delayed. A 31-year-old male with known atresia of the inferior vena cava who received a deceased donor renal transplant 7 years previously presented to hospital with severe graft site pain and a week of nausea, vomiting, and chills. Serum creatinine was markedly elevated from baseline. Sonographic examination revealed external iliac vein thrombosis with extension of the thrombus into the transplant renal vein. Urgent angiographic administration of tissue plasminogen activator and suction thrombectomy was performed, then followed by heparin and clopidogrel post procedure. Within 24 h, his serum creatinine improved, and within 2 weeks returned to his baseline. He was started on lifelong warfarin anti-coagulation to reduce the risk of rethrombosis secondary to his uncorrectable aberrant venous anatomy. Due to the turbulent and sometimes reversed flow in the major veins, lifelong anticoagulation should be strongly considered for such transplant patients with recipient aberrancy of the large veins.




Similar content being viewed by others

References
Delbeke D, Sacks GA, Sandler MP. Diagnosis of allograft renal vein thrombosis. Clin Nucl Med 1989; 415–20.
Schweiger J, Reiss R, Cohen JL, et al. Acute renal allograft dysfunction in the setting of deep venous thrombosis: a case of successful urokinase thrombolysis and a review of the literature. Am J Kidney Dis. 1993;22(2):345–50.
Duckett T, Bretan PN, Cochran ST, et al. Non-invasive radiological diagnosis of renal vein thrombosis in renal transplantation. J Urol. 1991;146:403–6.
Krishnaswamy SK, Rajan M, Prabahar A. Successful thrombolysis of renal allograft venous thrombosis – a case report. Indian J Transpl. 2014;8:57–9.
Ehrlich RM, Smith RB. Surgical complications of renal transplantation. Urology. 1977;10:43–39.
Muscianese L, Seese RR, Graham W, Williams JH. Congenital atresia of the inferior vena cava and antithrombin III deficiency in a young adult: compounding risk factors for deep vein thrombosis. BMJ Case Rep. 2015. https://doi.org/10.1136/bcr-2014-205729.
Malone PC, Agutter PS. The aetiology of deep venous thrombosis. QJM Int J Med. 2006;99(9):581–93.
Fathi T, Samhan M, Gawish A, et al. Renal allograft venous thrombosis is salvageable. Transpl Proc. 2007; 39(4):1120–1121.
Muradahli D, Chawla T. Organ transplantation. In: Rumack CM, editor. Diagnostic ultrasound. 4th ed. Philadelphia: Mosby; 2011. pp. 639–706.
Freitas C, Fructuso M, Rocha MJ, Almeida M, Pedroso S, Martins LS, Dias L, Castro Henriques A, Almeida R, Cabrita A. Late venous thrombosis of renal allograft: two cases with different treatment and outcome. Nefrologia. 2011;31(1):115–7.
Witz M, Korzets Z. Renal vein occlusion: diagnosis and treatment. Isr Med Assoc J. 2007;9(5):402–5.
Hogan JL, Rosenthal SJ, Yarlagadda SG, Jones JA, Schmitt TM, Kumer SC, Kaplan B, Deas SL, Nawabi AM. Late-onset renal vein thrombosis: a case report and review of the literature. Int J Surg Case Rep. 2015; 6C:73–76.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no conflict of interest exists.
Informed consent
Informed consent was obtained from the individual included in the study.
Ethical approval
All procedures performed were in accordance with the ethical standards of the institutional research committee of the University of Saskatchewan and the Saskatoon Health Region (Bio REB#12-44).
About this article

Cite this article
Thiessen, L., MacDonell, S., Wall, C. et al. Transplant renal vein thrombosis in a recipient with aberrant venous anatomy. CEN Case Rep 7, 264–267 (2018). https://doi.org/10.1007/s13730-018-0340-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13730-018-0340-3