
Abstract
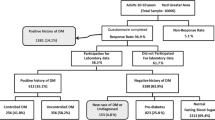
To study the prevalence of Type 2 Diabetes Mellitus (T2DM) in a population of United Arab Emirates (UAE) residents through the creation of the “Emirates Family Registry” (EFR). Major hospitals and diabetes centres in the UAE were contacted to establish a bio-banking facility referred to as the EFR. Through assistance made available by the Ministry of Health and collaborators of this network, demographic data of T2DM patients were collected and collated in a database for analysis and longitudinal studies. Clinical specimens were collected for biochemical profiling (such as; glucose, lipids, HbA1c levels). In the first 24 months of the operation the EFR recruited 23,064 adult volunteers from three major hospitals and nine primary care centres throughout the UAE. Within this cohort, 88% were patients classified as T2DM patients from the medical records. The cohort was divided into age categories with 59% of T2DM patients aged between 40 and 59 years old. UAE nationals comprised 30% of the database of which 21% were diagnosed with T2DM. However the percentage of adults with T2DM was higher in other ethnic groups effecting almost 33% of the Indians who live in the UAE. A total of 741 UAE Nationals consented to donate blood; in phase I of the study; for biochemical testing after which 23% were diagnosed with T2DM, 30% with pre-T2DM and 47% were healthy. This study is consistent with the previously reported high prevalence of T2DM in the UAE. Furthermore, analyses of the factors that predispose to the disease have revealed that obesity, a large waist circumference, consanguineous marriage, family history, lack of physical activity, unhealthy dietary practices, high total cholesterol, and high triglycerides levels were more prevalent in T2DM patients. The classification of these features will contribute to defining more effective and specific plans to screen for and manage diabetes and its complications in UAE and other developing countries.

Similar content being viewed by others
References
El-Sharkawy T. Diabetes in the United Arab Emirates and other Arab Countries: need for epidemiological and genetic studies. Genetic disorders in the Arab world. Dubai: centre for Arab genomic studies; 2004. p. 57.
Rasheed A. Expat numbers rise rapidly as UAE population touches 6 m. United Arab Emirates: Gulf News; 2009.
Malik M, Bakir A, Saab BA, King H. Glucose intolerance and associated factors in the multi-ethnic population of the United Arab Emirates: results of a national survey. Diabetes Res Clin Pract. 2005;69:188–95.
Reed RL, Revel AD, Carter AO, Saadi HF, Dunn EV. A controlled before-after trial of structured diabetes care in primary health centres in a newly developed country. Int J Qual Health Care. 2005;17:281–6.
Niazi TN, Cannon-Albright LA, Couldwell WT. Utah population database: a tool to study the hereditary element of nonsyndromic neurosurgical diseases. Neurosurg Focus. 2010;28:E1.
Nystrom L, Dahlquist G, Ostman J, Wall S, Arnqvist H, Blohme G, et al. Risk of developing insulin-dependent diabetes mellitus (IDDM) before 35 years of age: indications of climatological determinants for age at onset. Int J Epidemiol. 1992;21:352–8.
Phillips P, Wilson D, Beilby J, Taylor A, Rosenfeld E, Hill W, et al. Diabetes complications and risk factors in an Australian population. How well are they managed? Int J Epidemiol. 1998;27:853–9.
Sekikawa A, Eguchi H, Tominaga M, Manaka H, Sasaki H, Chang YF, et al. Evaluating the reported prevalence of type 2 diabetes mellitus by the Oguni diabetes registry using a two-sample method of capture-recapture. Int J Epidemiol. 1999;28:498–501.
Villegas R, Shu XO, Li H, Yang G, Matthews CE, Leitzmann M, et al. Physical activity and the incidence of type 2 diabetes in the Shanghai women’s health study. Int J Epidemiol. 2006;35:1553–62.
Scott LJ, Mohlke KL, Bonnycastle LL, Willer CJ, Li Y, Duren WL, et al. A genome-wide association study of type 2 diabetes in Finns detects multiple susceptibility variants. Science. 2007;316:1341–5.
Oguma Y, Sesso HD, Paffenbarger Jr RS, Lee IM. Weight change and risk of developing type 2 diabetes. Obes Res. 2005;13:945–51.
Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27:1047–53.
de Costa CM. Consanguineous marriage and its relevance to obstetric practice. Obstet Gynecol Surv. 2002;57:530–6.
Chen Y, Rennie DC, Dosman JA. Synergy of BMI and family history on diabetes: the humboldt study. Public Health Nutr. 2009;1–5.
Bener A, Zirie M, Al-Rikabi A. Genetics, obesity, and environmental risk factors associated with type 2 diabetes. Croat Med J. 2005;46:302–7.
Okosun IS, Cooper RS, Rotimi CN, Osotimehin B, Forrester T. Association of waist circumference with risk of hypertension and type 2 diabetes in Nigerians, Jamaicans, and African-Americans. Diabetes Care. 1998;21:1836–42.
Ding EL, Hu FB. Smoking and type 2 diabetes: underrecognized risks and disease burden. JAMA. 2007;298:2675–6.
Centers for Disease Control and Prevention. National diabetes fact sheet: general information and national Estimates on diabetes in the United States. Department of Health and Human Services. 2005.
Acknowledgements
Publication number HA09-0005 of the Centre for Forensic Science at the University of Western Australia. Funding for this project was provided by the Emirates Foundation. We would like to thank the Al-Baraha Hospital for assisting with biochemical tests performed in this study.
Conflict of Interest
All the authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Alsafar, H., Jama-Alol, K.A., Hassoun, A.A.K. et al. The prevalence of Type 2 Diabetes Mellitus in the United Arab Emirates: justification for the establishment of the Emirates Family Registry. Int J Diabetes Dev Ctries 32, 25–32 (2012). https://doi.org/10.1007/s13410-012-0062-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13410-012-0062-6