
Abstract
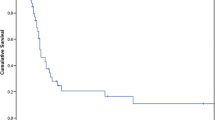
Treatment of adrenal metastases from cancer of the esophagogastric junction (EGJ) is not defined. The aim of the present work is to analyze retrospectively our experience in treating patients with adrenal metastases from EGJ adenocarcinoma. 102 patients with Siewert 1 or 2 EGJ adenocarcinoma underwent esophagectomy between May 2001 and Jan 2009. Five patients were diagnosed an adrenal metastases from EGJ adenocarcinoma, synchronous (s) in one and metachronous (m) in four, in the latter 11 months (mean) after esophagectomy. At diagnosis, three patients had synchronous metastases to mediastinal nodes (1 s and 2 m), 1 (m) had synchronous metastases to bone, and 1 (m) had an isolated adrenal metastasis. Three patients with synchronous node metastasis received chemotherapy followed by adrenalectomy 3, 8 and 16 months (mean 9) after diagnosis; one patient also received postoperative mediastinal radiotherapy. These patients are alive with no evidence of disease 16, 40 and 50 months after diagnosis of adrenal metastasis. The patient with bone metastasis received chemotherapy only and died 12 months after diagnosis of metastatic disease. The patient with isolated metastasis underwent laparoscopic adrenalectomy only, developed early bone metastases and died 15 months after surgery. In conclusion, our experience indicates that patients with adrenal metastases from adenocarcinoma of the EGJ may benefit from adrenalectomy if the gland is the only site of metastasis beyond lymphnodal disease. Chemotherapy should be considered before adrenalectomy to achieve better disease control and identify aggressive disease that would contraindicate adrenalectomy.
Similar content being viewed by others

References
Lo CY, van Heerden JA, Soreide JA, Grant CS, Thompson GB, Lloyd RV, Harmsen WS (1996) Adrenalectomy for metastatic disease to the adrenal glands. Br J Surg 83:528–531
Lam KY, Lo CY (2002) Metastatic tumours of the adrenal glands: a 30-year experience in a teaching hospital. Clin Endocrinol (Oxf) 56:95–101
Kim SH, Brennan MF, Russo P, Burt ME, Coit DG (1998) The role of surgery in the treatment of clinically isolated adrenal metastasis. Cancer 82:389–394
D’Angelica M, Gonen M, Brennan MF, Turnbull AD, Bains M, Karpeh MS (2004) Patterns of initial recurrence in completely resected gastric adenocarcinoma. Ann Surg 240:808–816
Song KY, Park SM, Kim SN, Park CH (2008) The role of surgery in the treatment of recurrent gastric cancer. Am J Surg 196:19–22
de Manzoni G, Pedrazzani C, Pasini F, Durante E, Gabbani M, Grandinetti A, Guglielmi A, Griso C, Cordiano C (2003) Pattern of recurrence after surgery in adenocarcinoma of the gastro-oesophageal junction. Eur J Surg Oncol 29(6):506–510
Nakahashi C, Kinoshita T, Konishi M, Nakagohri T, Inoue K, Oda T, Joshida J, Hasebe T, Ochiai A (2004) Long-term survival achieved by repeated resections of metachronous pulmonary and adrenal metastases of alpha-fetoprotein-producing gastric cancer: report of a case. Surg Today 34:784–787
Mokuno Y, Katayama M, Ogura Y, Kimura K, Koh K (2006) Long-term survival after resection of metachronous bilateral adrenal metastases of mucinous gastric carcinoma: report of a case. Surg Today 36:554–558
Do YR, Song HS, Kim IH (2007) Adrenalectomy for metastatic disease to the adrenal gland from gastric cancer: report of a case. Korean J Intern Med 22:18–20
Cho MM, Kobayashi K, Aoki T, Nishioka K, Yoshida K, Hatano N, Hirose H, Moon JH, Matsumoto T, Uemura Y, Kaneko T, Okagawa K (2006) Surgical resection of solitary adrenal metastasis from esophageal carcinoma following esophagectomy. Dis Esophagus 20:79–81
Kosaka T, Ueshige N, Ji Sugaya, Nakano Y, Tomita F, Saito H, Kita I, Takashima S (1999) A long surviving case of resected gastric cancer presenting with synchronous adrenal metastasis. Gastric Cancer 2:142–144
Böhner H, Zimmer T, Hopfenmüller W, Berger G, Buhr HJ (2000) Detection and prognosis of recurrent gastric cancer—is routine follow-up after gastrectomy worthwhile? Hepatogastroenterology 47:1489–1494
Fumagalli U, Panel of Experts (1996) Resective surgery for cancer of the thoracic esophagus. Dis Esophagus 9:30–38
Takeyoshi I, Ohwada S, Ogawa T, Kawashima Y, Ohya T, Kawate S, Nakasone Y, Arai K, Ikeya T, Morishita Y (2000) The resection of non-hepatic intraabdominal recurrence of gastric cancer. Hepatogastroenterology 47:1479–1481
Lehnert T, Rudek B, Buhl K, Golling M (2002) Surgical therapy for loco-regional recurrence and distant metastasis of gastric cancer. Eur J Surg Oncol 28(4):455–461
Toniato A, Boschin I, Bernante P, Foletto M, Guolo AM, Pelizzo MR, Opocher G, Ballotta E, Mantero F (2009) Factors influencing the rising rates of adrenal surgery: analysis of a 25-year experience. Surg Endosc 23:503–507
Lee J, El-Tamer M, Schifftner T, Turrentine FE, Henderson WG, Khuri S, Hanks JB, Inabnet WB (2008) Open and laparoscopic adrenalectomy: analysis of the National Surgical Quality Improvement Program. J Am Coll Surg 206:953–959 (discussion 959–961)
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fumagalli, U., de Carli, S., de Pascale, S. et al. Adrenal metastases from adenocarcinoma of the esophagogastric junction: adrenalectomy and long-term survival. Updates Surg 62, 63–67 (2010). https://doi.org/10.1007/s13304-010-0012-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13304-010-0012-0