
Abstract
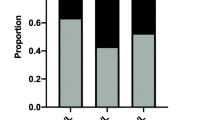
This study demonstrates a strong association of high urinary iodine with thyroid nodules and papillary thyroid cancer as well as aggressive cancer features, suggesting that high urinary iodine is a risk factor for thyroid cancer. The risk of high iodine intake for thyroid cancer has been suggested but not established. The objective of the study was to evaluate the relationship between urine iodine levels and thyroid nodule and thyroid cancer. We preoperatively tested fasting urine iodine in 154 thyroid nodule patients and correlated the results with pathological diagnoses and compared with 306 subjects as normal control. The median urine iodine (MUI) was 331.33 μg/L in patients with benign thyroid nodules versus 466.23 μg/L in patients with papillary thyroid cancer (PTC) (P = 0.003), both of which were in the excessive iodine state and higher than the MUI of 174.30 μg/L in the control group (P < 0.001), which was in the sufficient iodine state. Excessive iodine state (MUI > 300 μg/L) was seen in 62.75 % of patients with benign thyroid nodules and 66.99 % of patients with PTC, both of which were significantly higher than the iodine excessive rate of 19.93 % in the control group (P < 0.001). Moreover, MUI in patients with PTC with lymph node metastasis was significantly higher than that of PTC patients without lymph node metastasis (P < 0.001). Urine iodine of thyroid cancer patients with stage III and IV disease was significantly higher than that of patients with stage I and II diseases (P < 0.001). Multivariable analyses showed that, like sand calcification of thyroid nodule and TSH, urine iodine was an independent risk factor for PTC. These data demonstrate a significant association between high urinary iodine and benign and malignant thyroid nodules and PTC aggressiveness, supporting high urinary iodine as a risk factor for thyroid malignancy. Further studies are warranted to confirm these findings.
Similar content being viewed by others


References
Cibas ES. Fine-needle aspiration in the work-up of thyroid nodules [J]. Otolaryngol Clin North Am. 2010;43(2):257–71.
Mazzaferri EL. Management of a solitary thyroid nodule. N Engl J Med. 1993;328:553–9.
Guth S, Theune U, Aberle J, et al. Very high prevalence of thyroid nodules detected by high frequency (13 MHz) ultrasound examination. Eur J Clin Invest. 2009;39:699–706.
Hundahl SA, Fleming ID, Fremgen AM, et al. A National Cancer Data Base report on 53,856 cases of thyroid carcinoma treated in the U.S., 1985–1995. Cancer. 1998;83:2638–48.
Leenhardt L, Grosclaude P, Cherie-Challine L Increased incidence of thyroid carcinoma in France: a true epidemic or thyroid nodule management effects? Report from the French Thyroid Cancer Committee Thyroid 2004; 14, 1056–1060
Howlader N, Noone AM, Krapcho M et al. SEER Cancer Statistics review, 1975–2009 (Vintage 2009 populations), National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2009_pops09/, based on November 2011 SEER data submission, posted to the SEER web site, April 2012. 2012.
Lind P, Langsteger W, Molnar M, et al. Epidemiology of thyroid diseases in iodine sufficiency. Thyroid. 1998;8(12):1179–83.
Gomez Segovia I, Gallowitsch HJ, Kresnik E, et al. Descriptive epidemiology of thyroid carcinoma in Carinthia, Austria: 1984–2001. Histopathologic features and tumor classification of 734 cases under elevated general iodination of table salt since 1990: population-based age-stratified analysis on thyroid carcinoma incidence. Thyroid. 2004;14(4):277–86.
MOH, Ministry of Health, P.R. China. WS /T 107–2006 Method for determination of urinary iodine by As-Ce catalytic spectrophotometry[S]. People’s Medical Publishing House, 2006.
WHO/UNICEF/ICCIDD. Assessment of the iodine deficiency disorders and monitoring their elimination [S].Geneva: WHO, 2001
Laurberg P, Bulow Pedersen I, Knudsen N, et al. Environmental iodine intake affects the type of nonmalignant thyroid disease [J]. Thyroid. 2001;11(5):457–69.
Zhao SH, Wang L, Wang YG, et al. Influence of iodine nutrition status and susceptible HLA alleles on the pathogenesis of Graves’ disease and Hashimoto’s thyroiditis in Shandong coastal area [J]. Chin J Endocrinol and Metab. 2002;18(6):462–3.
Zhao SH, Wang YG, Yan SL, et al. The effect of iodine nutrition status on anti-thyroid medicine for Graves’ disease [J]. Acta Acadmiae Medicinae Qingdao Universitatis. 2004;40(3):195–6.
Chen JE, Song LJ. New epidemic characteristics of thyroid cancer [J]. Chin J Clin Med. 2009;16(5):812–3.
Dal Maso L, Bosetti C, La Vecchia C, et al. Risk factors for thyroid cancer: an epidemiological review focused on nutritional factors [J]. Cancer Causes Control. 2009;20(1):75–86.
Knobel M, Medeiros-Neto G. Relevance of iodine intake as a reputed predisposing factor for thyroid cancer [J]. Arq Bras Endocrinol Metabol. 2007;51(5):701–12.
Bacher-stier C, Riccabona G, Totsch M, et al. Incidence and clinical characteristics of thyroid carcinoma after iodine prophylaxis an endemic goiter country [J]. Thyroid. 1997;7:733–41.
Hx G, Li CY, Teng WP, et al. High iodine intake is a risk factor of post-partum thyroiditis: result of a survey from Shenyang, China [J]. J Endocrinol Invest. 2005;28(10):876–81.
Eng PH, Cardona GR, Previti MC. Regulation of the thyroid iodide symporter by iodide in FRTL-5 cells [J]. Eur J Endocrinol. 2001;144(2):139–44.
Wu L, Yu JC, Kang WM, et al. Iodine nutritional status and thyroid diseases.[J]. Acta Acad Med Sin. 2013;35(4):363–8.
Conflict of interest
None
Funding
Shandong medical and health research projects, China.
Author information
Authors and Affiliations
Corresponding author
Additional information
Fang Wang and Yangang Wang contributed equally to this work.
Rights and permissions
About this article

Cite this article
Wang, F., Wang, Y., Wang, L. et al. Strong association of high urinary iodine with thyroid nodule and papillary thyroid cancer. Tumor Biol. 35, 11375–11379 (2014). https://doi.org/10.1007/s13277-014-2397-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-014-2397-8