
Abstract
Objective
Aim of this audit is to analyse indication and proportion of babies delivered by elective caesarean section at less than 39+0 weeks of gestation exposed to antenatal corticosteroids performed in a Premier Hospital, Hywel Dda Health University. The second aim was to learn how an audit can be done and used for improving clinical practice.
Methods
Present study involved all patients who underwent elective caesarean delivery before 39 weeks completed period of gestation in August and September 2014. Data collected from medical record tracking using ICD-9 codes and analysed by clinical audit department.
Exclusion
Patients who underwent elective caesarean section after 39 weeks completed period of gestation.
Discussion
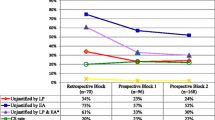
The audit showed 66.6 % of patients were given antenatal corticosteroids. The observation was discussed in consultant meetings, labour forum, and was send as e-mail to every one working in Department of Obstetrics and Gynaecology. The goal was 100 %. Reaudit is to be performed in year time to know the effect of change in practice. All successful audits are structured programmes with realistic aims and objectives, leadership and attitude of senior management, nondirective, hands-on approach, support of staff, strategy groups and regular discussions, emphasis on team working and support, environment conducive to conducting audit.

Similar content being viewed by others


References
Parliamentary Office of Science and Technology. Caesarean sections. Postnote. 2002;184:1–4.
Menacker F. Trends in cesarean rates for first births and repeat cesarean rates for low-risk women: United States, 1990–2003. Natl Vital Stat Rep. 2005;54:1–8.
Liu S, Rusen ID, Joseph KS, et al. Recent trends in caesarean delivery rates and indications for caesarean delivery in Canada. J Obstet Gynecol Can. 2004;26:735–42.
Black C, Kaye JA, Jick H. Cesarean delivery in the United Kingdom: time trends in the general practice research database. Obstet Gynecol. 2005;106:151–5.
Yeh J, Wactawski-Wende J, Shelton JA, et al. Temporal trends in the rates of trial of labor in low-risk pregnancies and their impact on the rates and success of vaginal birth after cesarean delivery. Am J Obstet Gynecol. 2006;194:144.
Landon MB, Hauth JC, Leveno KJ, et al. Maternal and perinatal outcomes associated with a trial of labor after prior cesarean delivery. N Engl J Med. 2004;351:2581–9.
Smith GC, Pell JP, Cameron AD, et al. Risk of perinatal death associated with labor after previous cesarean delivery in uncomplicated term pregnancies. JAMA. 2002;287:2684–90.
Tita AT, Landon MB, Spong CY, et al. Eunice Kennedy Shriver NICHD maternal-fetal medicine units network. Timing of elective repeat cesarean delivery at term and neonatal outcomes. N Engl J Med. 2009;360:111–20.
Yee W, Amin H, Wood S. Elective cesarean delivery, neonatal intensive care unit admission, and neonatal respiratory distress. Obstet Gynecol. 2008;111:823–8.
Hansen AK, Wisborg K, Uldbjerg N, et al. Risk of respiratory morbidity in term infants delivered by elective caesarean section: Cohort study. BMJ. 2008;336:85–7.
Morrison JJ, Rennie JM, Milton PJ. Neonatal respiratory morbidity and mode of delivery at term: influence of timing of elective caesarean section. Br J Obstet Gynecol. 1995;102:101–6.
Stutchfield P, Whitaker R. Russell I; Antenatal Steroids for Term Elective Caesarean Section (ASTECS) Research Team. Antenatal betamethasone and incidence of neonatal respiratory distress after elective caesarean section: pragmatic randomised trial. BMJ. 2005;331:662.
Smith R. Audit and research. BMJ. 1992;305:905–6 (see comments).
NHS, National Institute for Clinical Excellence, Commission for Health Improvement, Royal College of Nursing, University of Leicester. Principles for best practice in clinical audit. Oxford: Radcliffe Medical Press; 2002.
Royal College of Obstetricians and Gynaecologists. Clinical effectiveness support unit team matters. Br J Cancer. 1994;70:363–70.
McKenzie-McHarg K, Ayres S. Data management. In: O’Brien PMS, Broughton Pipkin F, editors. Introduction to research methodology for specialists and trainees. London: RCOG Press; 1999. p. 140–6.
Brocklehurst P, Gates S. Statistics. In: O’Brien PMS, Broughton Pipkin F, editors. Introduction to research methodology for specialists and trainees. London: RCOG Press; 1999. p. 147–60.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author declares that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants performed by author.
Additional information
Dr. Georgy Joy Eralil, MBBS, MS, DGO, MRCOG, is the Associate Professor in Department of Obstetrics and Gynaecology at Sreenarayana Institute of Medical Sciences.
Appendix
Appendix

Rights and permissions
About this article

Cite this article
Eralil, G.J. Understanding Audit in Obstetrics. J Obstet Gynecol India 66 (Suppl 1), 223–228 (2016). https://doi.org/10.1007/s13224-016-0840-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13224-016-0840-z