
Abstract
Introduction
The American College of Medical Toxicology Case Registry was established in 2010 as a method of identifying cases cared for by medical toxicologists at participating institutions. The Registry allows for the extraction of information from medical records making it the most robust multicenter database on chemical toxicities in existence. The current report is a summary of the data collected in 2010.
Methods
All cases seen by medical toxicologists at participating institutions were entered on a database. Information characterizing patients entered in 2010 was tabulated.
Results
Over the course of 2010, the number of institutions contributing cases grew from 4 to 50. Three thousand nine hundred forty-eight cases were entered. Emergency departments were the most common source of consultations, accounting for approximately 50% of the cases. The most common reason for consultations was for pharmaceutical overdoses, which occurred in 42% of the patients. The most common classes of agents were non-opioid analgesics (14%), sedative/hypnotics/muscle relaxants (10%), ethanol (8%), and opioids (8%). N-acetylcysteine was the most common antidote used, followed by opioid antagonists, sodium bicarbonate, and physostigmine. Anti-crotalidae Fab fragments were administered in 72% of the cases in which an antivenin was used. Signals were detected suggesting the possibility that amlodipine and metoprolol were associated with greater toxicity than had been previously recognized.
Conclusions
The Registry can identify and characterize patients who have sufficient toxicity to require a consultation by a medical toxicologist. Hypotheses for further investigation emerged from the data. The Registry appears to be a potentially powerful tool for toxicovigilance and research.
Similar content being viewed by others

The American College of Medical Toxicology (ACMT) Case Registry was established in early 2010 as a method of recording all cases cared for by medical toxicologists in the USA. This information was deemed important for both toxicosurveillance and research. The Case Registry is unique in that it contains information on patients who have all been evaluated at the bedside in hospitals or in clinics by medical toxicologists. The Registry allows for the identification and subsequent extraction of detailed clinical information from patients’ medical records making it the most robust multicenter clinical toxicology database in existence. Because all cases in the Registry are there by virtue of a medical toxicologist evaluation of the patient, the cases contained therein tend to be those with more serious toxicities.
A full description of the Registry has been published [1]. This is the first annual report and it is based on an analysis of 3,948 patients cared for by participating medical toxicologists at participating institutions during 2010. In 2010, there were 50 hospitals and clinics contributing cases to the Registry.
Methods
All participating centers, by agreement, enter all of their medical toxicology consultation cases into the Case Registry. Case entry is done online using a password-protected database maintained by ACMT. No patient identifiers are provided on the database [1]. Participation in the Case Registry is done pursuant to local institutional review board policies and procedures. A list of centers participating in the Case Registry during 2010 is listed in Table 1.
The information stored on the database is strictly descriptive and statistical. A number of fields are populated for each patient involving check offs or drop-down boxes. There are free text fields for signaling new, unusual, or sentinel cases, as well as for entry of the substances or species involved. More detailed queries require access to specific patient’s charts. This is done only in the context of an approved study or as allowed by statute, such as reporting the details of an adverse drug reaction to the FDA.
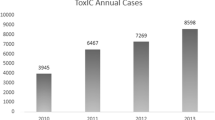
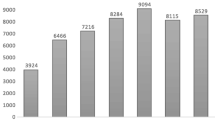
For this report, a search was made of the database assessing the parameters in each field between the dates of 10 January 2010, when the database was initially started with four centers, and 31 December 31 2010, when 50 institutions were contributing data. The patient accrual over time is shown in Table 2. Only data fields with significant numbers of cases are shown.
Hospitalized cases in the Case Registry were either admitted directly to medical toxicology services or cared for by virtue of a consultation request. In this report, all types of patient encounters, as well as outpatient visits, are referred to as consultations.
Over the course of 2010, as more experience was gained, the specific statistical data collected on each patient evolved. This was due to the addition of several data fields. Because of these additions, some of the data reported by us are based on only a partial year collection and thus expressed only as the percentage of use over that period.
Results
Demographic data about patients in the Case Registry are shown in Table 3. Most cases were in the age category 19 to 64 years old, although approximately one quarter of the patients were in the pediatric age group. As shown in Table 4, approximately half of the consultations came from emergency departments. Thirteen percent of the patients were transferred from other hospitals.
Intentional pharmaceutical overdose represents the most common type of patient in the Case Registry, accounting for 42% of the cases (Table 5). The next most common category was drug abuse, accounting for approximately one quarter of the patients. The agents of abuse were evenly divided between prescription and nonprescription drugs. Table 5 also shows the frequency of medical toxicology consultations for other reasons.
Table 6 shows the classes of agents responsible for medical toxicology consultations. The most common were non-opioid analgesics. Specific toxidromes were identified in 25% (997/3948) of the cases. The most common was the sedative-hypnotic, followed by anticholinergic toxidromes.
The agents responsible for the 856 cases involving non-opioid analgesics are shown in Table 7. Acetaminophen was by far the most common, responsible for 70% of all cases in this category and thus 15% of Registry cases in 2010. Non-salicylate nonsteroidal anti-inflammatory agents (NSAIDS) made up, in the aggregate, 13% of the cases, of which ibuprofen was overwhelmingly the most common. Sixteen percent of cases were due to salicylates, 99% of which involved aspirin.
Sedative-hypnotic agents and muscle relaxants accounted for 826 cases in the Registry (Table 8). Of these, approximately two thirds were due to benzodiazepines, with clonazepam being the most common. Muscle relaxants, particularly cyclobenzaprine and carisoprodol, accounted for 18% of cases. Barbiturates were responsible for only 5% of the cases, of which two thirds were due to butalbital.
As shown in Table 9, approximately equal numbers of atypical antidepressants and selective serotonin reuptake inhibitors were recorded. Almost one quarter of the cases were due to tricyclic agents. The most common agents in each class were bupropion, citalopram, and amitriptyline.
Opioids and opiates accounted for 620 cases (Table 10). The most common category was semisynthetic agents, primarily oxycodone. The synthetic agents made up approximately one third of the cases, of which methadone was the most common.
As shown in Table 11, 366 cases were due to anticholinergic/antihistamine toxicity, most commonly diphenhydramine, followed by hydoxyzine. Table 12 shows the antipsychotic agent cases. Eighty-five percent of these cases involved atypical agents, particularly quetiapine and risperidone.
The 240 cases involving cardiovascular agents are shown in Table 13. As can be seen in the table, this category represents a diverse group of medications. The most common categories were beta blockers (36%) and calcium channel blockers (24%). Metoprolol was the most common beta blocker, accounting for 36% of the cases. This was followed by atenolol and propranolol. Amlodipine was responsible for almost half of the cases of calcium channel blocker toxicity. Verapamil accounted for approximately one quarter of the cases.
Table 14 shows the agents involved in sympathomimetic cases. Methamphetamine and cocaine were the most common, each accounting for nearly one third of the cases. Cases classified as involving psychoactive drugs of abuse are shown in Table 15. Fifty-nine percent of these were related to the use of dissociative agents, primarily dextromethorphan. The second most common group of agents in this category was cannabinoids, for which there were 11 cases involving synthetics.
Snakebites made up two thirds of the envenomation cases (Table 16). Most of these involved rattlesnakes. Twenty-eight percent of the cases involved copperhead bites.
Table 17 shows the number of cases involving alcohols and glycols. Ethylene glycol represented almost one half of the non-ethanol-related cases, followed by isopropanol and methanol.
Anti-diabetic medication-related cases are shown in Table 18. The sulfonylureas were the most common agents, accounting for 40% of cases. Metformin accounted for almost one third of cases while insulin was responsible for an additional approximately one quarter of the cases.
As shown in Table 19, basic substances, primarily sodium hypochlorite, made up nearly 50% of the caustic cases. Acids made up 22%, the most common being acetic, hydrochloric, and hydrofluoric. Each of these was responsible for almost one third of the acid cases.
Specific antidotes used are shown in Table 20. Because these data are only from a part of the year they are expressed as percentages of use. The most commonly administered antidotes were N-acetylcysteine, opioid antagonists, sodium bicarbonate, and physostigmine. Ovine crotalidae Fab snake antivenin was the most commonly used antivenin and succimer was the most frequently administered chelator.
Of the cases in which an enhanced elimination technique was utilized, hemodialysis constituted over half (53%). The latter was used much more frequently than continuous renal replacement therapy, which was done in 9% of these cases. Urinary alkalinization was done in 24% and multi-dose activated charcoal was used in 14% of the cases in which an enhanced elimination technique was recorded.
Three 3% of cases in the Registry were listed as adverse drug reactions (ADRs). Detailed categorization of the ADRs is shown in Table 21. Eighty-four different medications were implicated. The most common were acetaminophen occurring in 13% of cases and lithium in 12%.
Discussion
The ACMT Case Registry was developed because there is no other multicenter data collection system that could lead to detailed medical record-validated information on patients experiencing adverse toxicological or pharmacological effects. The data from the patients in the Case Registry are unique in that these are of high quality specifically related to toxicological issues because the patients were directly evaluated and cared for by a medical toxicologist.
The Case Registry collects de-identified patient data on all medical toxicology consultations by participating institutions. This dataset provides an important profile of those patients requiring care by medical toxicologists. Because of this, the Case Registry does not provide incidence data on all poisonings. Patients with minor exposures are less likely than those with serious toxicities to receive care by medical toxicologists. Thus, the Registry provides information biased towards sicker patients and can be used, therefore, to extract information on more serious toxicities.
The Case Registry began in 2010 with only four centers [1]. Over the course of the year, progressively more centers joined the Registry so that by 31 December 2010 there were 50 participating institutions. Therefore, the rate of patient accrual increased as the year progressed. The fact that case accrual was not random over the year, but was weighted towards the latter part of 2010, is unlikely to have a major effect on most of the data points in the Registry. However, for toxicities in which there is a seasonal predominance, such as carbon monoxide poisoning, or geographical predominance, such as crotaline envenomation, the frequencies presented here may not be representative of what would have been collected by all centers over a 12-month period.
A number of interesting trends can be gleaned from the data we present. Serious poisonings appear to be least common in the 7–12 year age group. Children in this age range are beyond the stage where they are vulnerable to the accidental toxicities seen in younger patients and many have not yet begun the patterns of possible drug abuse and attempts at self-harm which become more common in teenagers. The pattern of few exposures in this age group is mirrored in the data collected by poison centers [2].
A truly unique aspect of the Registry is that for the first time we have data on the bedside practice patterns of medical toxicologists, as seen in Tables 4 and 5. Such information may be useful to individual medical toxicologists as they strategize on building a successful practice. The most common type of patients cared for by medical toxicologists are those who have intentionally overdosed on a pharmaceutical agent and for whom the consultation arose from an emergency department. However, there is a broad diversity of reasons that medical toxicologists are consulted (Table 5) and intentional pharmaceutical overdoses account for less than half of all patients. N-acetylcysteine was the most commonly used antidote, a fact consistent with the high frequency of acetaminophen-related consultations.
Of all cases involving non-opioid analgesics, acetaminophen comprised 70% and non-salicylate NSAIDS 13%. Because of the possibility of acetaminophen-induced hepatic injury, patients ingesting this agent are often admitted for antidotal therapy with N-acetylcysteine. The decreased late toxicity of NSAIDS compared to acetaminophen likely results in fewer hospital admissions and medical toxicology consultations for this group of medications.
It is clear that there is a major difference in the frequency with which cases appear on the Case Registry and their market share. This is dramatically demonstrated with the cardiovascular agents where angiotensin-converting enzyme inhibitors accounted for only 1% of the cases and statins only 4%. In contrast, there was an overrepresentation of beta blockers and calcium channel blockers, the two categories of cardiovascular agents associated with the most significant acute toxicity. Although propranolol and verapamil are generally thought of as the most toxic agents in this category, the predominance of metoprolol and amlodipine cases suggest that these agents may have a greater likelihood of causing toxicity than has been previously recognized. However, the difference in submissions to the Registry may reflect a difference in the number of dispensed prescriptions. For example, in 2009, metoprolol ranked number 9 and amlodipine ranked number 15 in number of prescriptions. Conversely, verapamil SR was ranked number 198 and propranolol was not among the top 200 prescribed medications [3]. This is an example of how the Registry can generate important hypothesis-driven studies.
It is interesting to note that ethanol and fomepizole are both used for the same indication—inhibition of alcohol dehydrogenase after the ingestion of a potentially toxic alcohol or glycol. In 100% of the cases in which an alcohol dehydrogenase inhibitor was used, fomepizole was chosen. This suggests that medical toxicologists, or the pharmacies in the institutions in which they practice, appear to have a strong preference for using fomepizole over ethanol.
One hundred and sixteen cases were classified as ADRs, representing 3% of all cases in the Registry. This is important as medical toxicologists are consulted for primarily serious adverse reactions. Simple rashes (non-blistering, non-bullous) make up a very large group of non-serious adverse drug reactions, yet there were only two such ADR cases in the Registry in 2010. Thus, ADRs potentially constitute a major area for toxicosurveillance for the Case Registry.
Interestingly, acetaminophen and lithium were the two medications most implicated in causing ADRs. Although it is possible that the acetaminophen-related ADRs are from liver function test abnormalities with therapeutic use, and the lithium cases involve such known therapeutic side effects as hypothyroidism or nephrogenic diabetes insipidus, these deserve further study.
The Case Registry has certain limitations. It provides real world prospective data on cases seen by medical toxicologists. However, as in the real world, many clinical conclusions are more diagnostic impressions than absolute truths. For example, in many cases, the substances implicated in the patients’ clinical presentation have not been verified by full analytical confirmation.
Categorization of some of the specific substances is subject to debate. In several cases, there was no absolute right answer. For example, should diphenhydramine be classified as an antihistamine or an anticholinergic? In cases of controversy, the substances were categorized by consensus.
Despite the Case Registry collecting nearly 4,000 cases in 2010, the number of cases in individual cells can be small. The Case Registry should be viewed as a constantly growing body of data. For purposes of aggregating cases together for research studies, the 2010 cases will be added to those subsequently collected. Given that the Registry’s current accrual rate is approximately 150 entries per week, the number of individual cases in the various cells should grow considerably over time.
This report is based only on statistical data from patients entered into the Case Registry. Therefore, these data are best viewed as providing information about the agents that cause serious poisonings, the reasons for such poisonings, and commonly used therapies. No attempt was made to correlate specific exposures with specific reasons for poisonings or with any age group. Because the Registry is continuing to collect cases, and at the time of publication of this report 57 institutions are contributing cases, it is expected that these further analyses will be forthcoming.
The strongest data available through the Case Registry are contained in the patients’ medical records. No attempt was made to mine any data from these records for this report. It is expected that as issues of toxicosurveillance or research questions arise, more in-depth analyses using individual patient medical records will be done.
References
Wax PM, Kleinschmidt K, Brent J (2011) The toxicology investigators consortium (ToxIC) registry. J Med Toxicol. doi:10.1007/s13181-011-0177-z
Bronstein AC, Spyker DA, Cantilena LR, Green JL, Rumack BH, Griffin SL (2010) 2009 Annual report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 27th annual report. Clin Toxicol 48(10):979
Pharmacy Times. May 11, 2011 posting. http://www.pharmacytimes.com/publications/issue/2010/May2010/RxFocusTopDrugs-0510. Accessed 28 August 2011
Acknowledgments
Funding for this project comes from the American College of Medical Toxicology.
Conflicts of interest
None
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
About this article
Cite this article
Brent, J., Wax, P.M., Schwartz, T. et al. The Toxicology Investigators Consortium Case Registry—The 2010 Experience. J. Med. Toxicol. 7, 266–276 (2011). https://doi.org/10.1007/s13181-011-0185-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13181-011-0185-z