
Abstract
Recent literature on the health impacts of CO2 emissions suggests a variety of factors that may establish a more robust link. However, no previous study has explored the role of research and development (R&D) in explaining the nexus between CO2 emissions and health outcomes. Using data for Saudi Arabia over the period 2000–2018, this paper investigates the ability of R&D (expenditures and environmentally related R&D) to reduce the incidence of emissions on population health outcomes, particularly infant mortality and life expectancy. We find (i) negative impacts of CO2 emissions on health outcomes; (ii) R&D expenditures have a weak positive impact on health outcomes; (iii) additionally to their direct effects on health outcomes, R&D expenditures remarkably enhanced health outcomes through reducing per capita CO2 emissions; (iv) R&D expenditures interact with CO2 from electricity and heat production and from electricity and heat production to negatively influence health outcomes. Similarly, environmentally related R&D, measured by patents environmental-related technologies, interacts with per capita CO2 emissions to negatively influence health outcomes. To address these negative impacts, we calculated the corresponding R&D thresholds. Policymakers in Saudi Arabia are therefore called to give more and more incentives for R&D to reduce emissions and then improve population health outcomes.
Similar content being viewed by others


Introduction
Carbon dioxide (CO2) emissions are the principal origin of human-induced global warming and associated climate change, which is widely seen to be one of the most serious worldwide dangers to human health (Costello et al., 2009). In general, it may influence population health in the following manners. First, inhaling high concentrations of emissions directly harms the respiratory system of people, inducing headaches, shortness of breath, and even delirium (Sechzer et al., 1960). Second, emissions may indirectly influence population health through climate change, which will lead to around 250,000 deaths each year over the period 2030–2050, according to the World Health Organization.Footnote 1 On the one hand, increasing CO2 emissions leads to global warming that changes the pattern and amount of precipitation and rising the intensity and frequency of extreme weather. On the other hand, by increasing air pollution and facilitating the propagation of climate-sensitive diseases, global warming will affect population health (Dong et al., 2021). For this reason, Watts et al. (2018) argue that effective solutions to address these issues are the current biggest word’s health opportunity.
However, in many developing economies, the costs of environmental pollution are inevitable as the energy and industrial sectors are vital sectors that generate the fundamental drivers of economic growth and development. So, the problem of linking human health to environmental pollution and economic progress is crucial for developing economies, especially those that have weak environmental policies (Wesseler & Zhao, 2019; Rodriguez-Alvarez, 2021), weak governance infrastructure (Ahmed et al., 2020; Omri & Mabrouk, 2020), unsuitable health infrastructure (Kiross et al., 2020), and weak share of renewable energy in the total energy mix (Martins et al., 2018; Omri & Belaid, 2021). As an oil-producing country, this study focuses on Saudi’s economy which still depends on fossil fuel production and consumption due to the cheapest and availability of energy resources, resulting in higher economic growth that increases carbon emissions causing negative impacts on health outcomes (Ahmed et al., 2020). Within this context, Omri et al. (2019) argue that since Saudi Arabia is the world’s top oil producer and is among the top world’s 10 largest emitters, reducing emissions is becoming an increasingly difficult task in the country, as the economic growth is primarily depending on fossil fuels. To deal with this issue, in its vision 2030, the Saudi government targets low environmental pollution (including air, soil, water, and sound) in the areas of the strategic goals of national industrial development and the national transformation agenda, designed to provide a healthy and satisfying life (Kingdom of Saudi Arabia, 2019). In this direction, this study attempts to investigate the ability of research and development (R&D) to reduce the effects of environmental degradation, specifically carbon emissions, on population health in Saudi Arabia.
Two large shortcomings are broadly shared by previous literature. The first gap concerns the nature of the linkage between CO2 emissions, health outcomes, and R&D. Most of previous studies have focused either on the health impacts of environmental degradation (Cao et al., 2011; Erdoğan et al., 2019; Guo & Luo, 2021; Liu et al., 2018; Majeed & Ozturk, 2020; Seppänen et al., 1999; Shobande, 2020; Sirag et al., 2017; Urhie et al., 2020), health impacts of R&D (Wald et al., 2007; Lucas, 2008; Blaya et al., 2010; Tsai et al., 2018; Majeed & Khan, 2019; Callaghan et al., 2019; Faria et al., 2021), or environmental impacts of R&D (Garrone & Grilli, 2010; Petrovic & Lobanov, 2020; Abid et al., 2022); however, to our knowledge, no empirical study took account the three variables in one framework. The second gap concerns a common failure to consider a policy variable that reduces CO2 emissions, which, in turn, enhance population health outcomes. Therefore, this study uses R&D as a possible channel that improves health outcomes by reducing CO2 emissions. To validate this assumption, R&D has interacted with CO2 emissions, and the net impacts on health outcomes are then processed from conditional and unconditional impacts.
To fill these shortcomings, this study contributes in the following ways. First, instead of looking for the mechanisms or tools that may lessen the incidences of CO2 emissions on population health, most of the previous studies have only focused on the direct relationship between the two phenomena. As already stated, we investigate the effectiveness of R&D in moderating the negative impacts of CO2 emissions on population health outcomes in Saudi Arabia over the period 2000–2018 using the dynamic ordinary least square (DOLS) method, which is suggested to deal with finite sample bias of OLS caused by endogeneity issue when estimating regression models based on cointegrated variables. To our knowledge, no previous study has examined the joint effects of CO2 emissions and R&D on health outcomes, especially in Saudi Arabia. Saudi Arabia is an important context for examining such interaction as it is currently ranked 8th among the world’s top emitter countries and the mitigating of carbon emissions to provide a healthy and satisfying life is a strategic goal of its 2030 vision. Different measures of R&D (R&D expenditures and environmentally related R&D), CO2 emissions (CO2 emissions per capita, CO2 emissions from electricity and heat production, CO2 from liquid fuel consumption, CO2 intensity), and health outcomes (infant mortality and life expectancy) are included in the analysis. Second, empirically, it extends the existing literature by computing and discussing the R&D thresholds under which the overall net negative effects become positive on population health outcomes. Third, in terms of results and policy implications, we find that, in most cases, the level of R&D in Saudi Arabia is not sufficient to moderate the effects of carbon emissions on health outcomes. For this reason, this study call policymakers in Saudi Arabia to give more and more incentives for R&D to reduce emissions and then improve health outcomes. In the same direction, corporates and firms’ decision-makers must integrate environmental sustainability into firms’ decision-making, which opens up new opportunities leading to better environmental and financial performance. Thus, more investments in green R&D can result in a reduction in CO2 emissions and positive financial performance.
After the introduction, the “Literature Review” section reviews the existing studies on the relationships among CO2 emissions, health, and R&D. The “Methodology and Data” section presents the used methodology and data. The “Results and discussions” section discusses the main findings. The “Conclusions and Implications” section concludes and offers some policy and practical recommendations.
Literature Review
Environmental Quality and Health
Over the past few decades, human activities have dramatically augmented carbon emissions and other types of greenhouse gases that affect human health. According to Majeed and Ozturk (2020), environmental degradation may influence human health by augmenting the concentration of outdoor air pollutants, creating negative variations in food production, creating heat stress, causing diseases of origin water, and spreading diseases, such as malaria, dengue fever, and aeroallergens. Additionally, environmental degradation appears to have various adverse health impacts in early human life, such as cardiovascular, respiratory, and perinatal disorders (USGCRP, 2009), leading to chronic diseases in adulthood or infant mortality (Hashim & Boffetta, 2014). Darçın (2017) argues that about 3.3 million people die annually in the world due to environmental degradation, particularly air pollution in the atmosphere. According to OECD forecasts, this later is “responsible for the premature mortality in the world.” There are many types of air pollutants, including CO2, SOx (sulfur oxides), and NOx (nitrogen oxides), which cause many diseases related particularly to respiration and increase health expenditures.
Empirically, a large number of scholars have examined the health impacts of environmental quality (Cao et al., 2011; Erdoğan et al., 2019; Liu et al., 2018; Magazzino et al., 2021a, 2021b; Majeed & Ozturk, 2020; Mele et al., 2021; Seppänen et al., 1999; Shobande, 2020; Sirag et al., 2017; Urhie et al., 2020). For example, Cao et al. (2011) explore the relationship between air pollution and mortality in China, and their findings show a positive effect of air pollution rising on mortality rates. For a sample of 35 African countries from 1995 to 2012, Sirag et al. (2017) apply the FMOLS and DOLS methods to investigate the association between health financing, CO2 emissions, and health outcomes. Their findings show a negative effect of emissions on health outcomes. The authors also highlight the significance of some socioeconomic variables, education, and health, in enhancing health outcomes. In the same direction, Erdoğan et al. (2019) analyze CO2 emissions’ effect on mortality rates and life expectancy in Turkey over the 1971–2016 period, and they find that CO2 emissions have a negative long-run effect on both health outcome indicators. The authors call to invest more and more in renewable energy to reduce CO2 emissions and their negative effect on Turkey’s health outcomes. Using data for 180 countries over the period 1990–2016, Majeed and Ozturk (2020) make a global study focused on carbon dioxide emissions’ effect on mortality and life expectancy as measures of population health outcomes. The empirical results confirm the negative effect of CO2 emissions on health outcomes. It reveals that countries with aloft CO2 emission levels suffer from elevated infant mortality rates and depressed life expectancy. The paper suggests taking some health reforms compatible with reducing CO2 emissions. Based on a sample of twenty-three African economies during 1999–2014, Shobande (2020) checks the energy use impact on infant mortality rate. This study’s findings show that energy use stimulates pollution and increases significantly infant mortality rates. The study also shows that relying on natural energy sources will reduce infant mortality. Based on these results, the researcher recommends rapid intervention by the African countries’ governments to save the region from the repercussions and dangers of the high use of polluted energy. Urhie et al. (2020) also display that economic growth increases air pollution, affecting Nigerians’ health. They show that public health expenditures can moderate this effect, but on the other hand, that does not decrease air pollution. The authors argue that the Nigerian government’s efforts must be focused on the use of environmentally friendly technologies that reduce CO2 emissions and enhance health outcomes, especially life expectancy. More recently, Magazzino et al. (2021a) examine the relationship between economic growth, air pollution, and COVID-19 using deep machine learning, and they find that PM2.5 and NO2 are the most significant pollutant agents responsible for facilitating COVID-19–attributed death rates.
Previous studies have only shown that CO2 emissions burden economies’ budgets because of their negative effect on health outcomes. Among the solutions proposed by some studies is to rely more on R&D to reduce CO2 emissions and develop healthcare services. In the following sub-section, we will highlight the importance of R&D in improving environmental quality and the general state of healthcare.
The Role of R&D
An increasing number of studies have focused on analyzing the nexus among environment, health, and R&D. We can split these studies into two strands of literature. The first strand focuses on reviewing the empirical association between R&D and environmental quality, particularly CO2 emissions (Dinda, 2004; Garrone & Grilli, 2010; Petrovic & Lobanov, 2020; Abid et al., 2022). Endogenous growth theory postulates that progress in technologies resulting from investments in R&D leads to higher efficiency in the consumption of energy and natural resources and in production. As income increases, economies are better able to invest in R&D and are, therefore, better able to adopt and use more effective technologies, which lower the dependence on natural resources as well as decrease emissions (Dinda, 2004). Therefore, more R&D investments are likely to improve environmental quality in circumstances where efficacious environmental management systems are in place to assure appropriate waste management (Arora & Cason, 1996). In the same direction, using data for 30 high-income economies, Garrone and Grilli (2010) investigate the empirical association between energy R&D and CO2 emissions, and they confirm that R&D reduces CO2 emissions. The paper recommends governments allocate a sufficient R&D budget to boost the energy innovation process. Similarly, using data from Japanese firms, Lee and Min (2015) investigate the linkage between green R&D and emissions, and they prove that investments in green R&D reduce CO2 emissions and improve companies’ financial performance. To boost this positive effect on the environment and firm performance, authors suggest firms develop some distinctive capabilities and resources. Using data for 95 countries, Li and Wang (2017) also investigate the impact of R&D on CO2 emissions, and they find that R&D has, on average, a negative effect on CO2 emissions. However, the authors support the idea that investments in R&D boost economic growth, which, in turn, increases emissions. For China, Zhang et al. (2017) use the system GMM method to study the effects of some environmental innovation measures on CO2 emissions. Their findings show that most of these measures, including R&D, reduce CO2 emissions. They recommend the policymakers in China create a favorable environment to reduce CO2 emissions, encourage companies to invest more and more in innovative activities, and build a creative network between them. Fernandez et al. (2018) also confirm the positive effect of R&D in reducing emissions for the United States, China, and the European Union (15). The authors recommend R&D expenditures as an engine of sustainable development because that makes it possible to reconcile between growth and decreasing CO2 emissions. For France, Shahbaz et al. (2018) show that R&D has a strong negative impact on CO2 emissions, and they advise to invest more and more in energy innovation because that improves significantly environmental quality and “will help French to address the environmental challenges and honor its commitments.” For G7 countries, Churchill et al. (2019) use a nonparametric data model to study the relationship between R&D and CO2 emissions. They show a varied relationship between R&D and CO2 emissions over time. By applying long-run regression models on the data of 16 OECD countries for the period 1981–2014, Petrovic and Lobanov (2020) find, on average, that R&D expenditures negatively affect CO2 emissions but cannot confirm this relation to 40% of the sample of countries. In addition, for the short-run level, the results of this study show that the impact of R&D on CO2 emissions can be negative, positive, or insignificant for many years. Based on these results, the authors argue that the association between R&D and CO2 emissions cannot be defined in advance and must be empirically estimated. They recommend following the US and German R&D programs that concentrate on dropping CO2 emissions.
The second strand of studies focuses on the linkage between health and R&D. In general, R&D, particularly in health, has a positive impact on society and addresses many significant health issues (clinical trials, patterns of care, disease trends, healthcare costs, public health interventions, risk factors, etc.). R&D plays a vital role in highlighting best practices, ensuring high-quality healthcare, and being an influent socioeconomic factor across countries. Many existing studies investigate the health R&D and its impact on health outcomes with different manners (Wald et al., 2007; Lucas, 2008; Blaya et al., 2010; Tsai et al., 2018; Majeed & Khan, 2019). For instance, Paruk et al. (2014) examine the adequacy of funds allocated by the Ministry of Health for R&D in South Africa health. This study affirmed that the greater R&D expenditure on health, the better the chance of achieving general goals in the field of health and supporting the improvement of the country’s health outcomes. The paper calls decision-makers to set realistic and transparent health goals where its achievement depends on R&D expenditures on health. The research carried out by Callaghan et al. (2019) indicates that the differences in R&D investments enhance healthcare inequality between countries. This inequality is clearer between developed and developing countries, and this is due to many reasons. The most important of these is the ability of developed countries to provide large financial allocations for R&D compared to developing countries. In addition to that, outcomes of R&D reached by developed countries do not necessarily serve the specific healthcare needs of developing countries. In the paper results, the researchers highlight the need for developing countries to enhance R&D expenditure to improve their health outcome indicators. The study of Faria et al. (2021) shows the importance of R&D in medical schools and its positive effect on R&D in hospitals, thus improving the general healthcare status in the country.
Most of the above-discussed studies have focused either on the health impacts of environmental degradation, the health impacts of R&D, or environmental impacts of R&D; however, to our knowledge, no empirical study took into account the three variables in one framework. They also show that stronger R&D would evidently have better health policies that can protect countries against the unwanted negative impacts of environmental degradation and thus profit the health outcomes of the population. Therefore, this paper argues the feasibility of R&D in mitigating the impacts of CO2 emissions on health outcomes. With this background, the objective of this study is to investigate the impacts of emissions on population health outcomes in the presence of R&D.
Methodology and Data
Model Specifications
Our empirical strategy is based on the health production model proposed by Grossman (1972). This model suggests that health outcomes depend on health inputs, including health constraints, medical facilities, and individual behavior. We start from the following health production function:
where H is the individual’s health outcomes and HI is the required individual’s health inputs. This function only analyses the micro-level health outcomes. Since the objective of this work is to analyze the macro-level health outcomes, we follow the study of Fayissa and Gutema (2005) who structured HI into environmental, social, and economic factors. Then, we have.
where P, S, and E are the vectors of environmental, social, and economic indicators, respectively. Since the main objective of this paper is to assess the relationship between CO2 emissions and health outcomes, the vectors of social and economic indicators are included in the model as control variables. The vector of environmental indicators includes four types of CO2 emissions (CO); the vector of social indicators included urbanization, education, and public health expenditure, and finally, the vector of economic indicators is limited to economic growth. Two broader proxies of health outcomes are used, namely infant mortality and life expectancy. The extended health production function can be specified as follows:
where t (t = 1…n) is the time period (1990–2018), ln denotes the natural logarithm, H is the health outcomes defined by infant mortality and life expectancy, CO indicates the proxies of CO2 emissions, and Z is the vector of control variables, including economic growth, education, and public health expenditures.
To investigate the ability of R&D in modulating the negative incidences of environmental degradation, particularly CO2 emissions, on health outcomes we rewrite Eq. (3) as follows:
where R&D is the research and development, which is measured by two proxies, namely R&D expenditures and environmentally related R&D—patents environmental-related technologies. CO * R&D is the interplay among the proxies of CO2 emissions and the two proxies of R&D. Therefore, we expect that the indicators of R&D would positively affect health outcomes (Paruk et al., 2014; Callaghan et al., 2019; Faria et al., 2021); however, the indicators of CO2 emissions have a negative effect (Farooq et al., 2019; Shobande, 2020; Urhie et al., 2020). Regarding the interaction between CO2 emissions and R&D, we expect that this later modulates the negative impacts of CO2 emissions on health outcomes.
Before estimating Eq. (4), we need first to verify the stationarity of the following variables. We then run the long-run equilibrium links among our series of variables. Finally, we use the DOLS estimator to estimate our model. This estimator takes lags and leads of the first-difference regressors to deal with the possible endogeneity bias (Omri et al., 2019).
Data
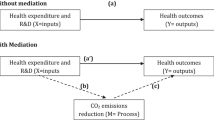
Using a time-series data for Saudi Arabia over the 2000–2018 period, this study examines the joint effects of R&D and CO2 emissions on health outcomes (Fig. 1). The study’s period has been chosen based on the accessibility of data on the two indicators of R&D. The definition and sources of the used variables are given as follows.

Conceptual model of the study
Dependent Variable
Two broad measures of the health outcomes’ dependent variable are used, namely infant mortality (Imo) and life expectancy (LE). Imo is expressed as infant mortality rates in per thousand live births. LE is defined as total life expectancy at birth in years. The data on Imo and LE are collected from the World Bank (WDI) online database.
Key Explanatory Variables
As stressed previously, the objective of this study is to examine the complementarity between R&D and CO2 emissions on health outcomes. Therefore, the core independent variables are:
-
Environmental Quality (P)
This study uses CO2 emissions as a measure of environmental degradation. Previous studies, such as Sileem (2016), Magazzino (2017a, b, 2019), Omri et al. (2021) and Omri and Saidi, (2022), among others, argue that CO2 emissions are the more reliable and valid indicator to measure environmental degradation. As mentioned in the first section, four proxies of CO2 emissions are included in the analysis to show which types of emissions influence health outcomes. Their relative data are collected from the World Bank (WDI) database. We expect that these indicators have positive and negative impacts on infant mortality rate and life expectancy, respectively.
-
Research and Development (R&D)
The R&D variable is included in the model as a policy instrument that may moderate the incidences of CO2 emissions on health outcomes. Two indicators of R&D are considered in the analysis, namely, research and development expenditures (RDexp) in the percentage of GDP and the number of patents environmental-related technologies (PET)—environmentally related R&D. The data on R&D expenditures is sourced from the World Bank (WDI) online database, while the data on PET is sourced from the OECD Statistics online database. The two indicators are expected to reduce CO2 emissions, which, in turn, reduce the rate of infant mortality and increase life expectancy.
Control Variables
In addition to these explanatory variables and following the study of Fayissa and Gutema (2005), other social and economic factors are included as inputs in the health outcomes function, namely public health expenditures, education, urbanization, and economic growth.
-
Public Health Expenditures (PHE)
The harmful impacts of environmental degradation on population health have increased the amount of public healthcare expenditure (Nasreen, 2021). A significant number of studies investigate the link between this latter and health outcomes and show that an increase in public health expenditure enhances health outcomes through improving health awareness and health facilities (see, e.g., Gupta et al., 2002; Arthur & Oaikhenan, 2017). The indicator of public health expenditure is expressed as domestic general government health expenditure in the percentage of GDP. The data on public health expenditure is collected from the World Bank (WDI) online database. Public health expenditures are expected to increase life expectancy and reduce infant mortality.
-
Education (Edu)
Health and education are two important characteristics of human capital. There is an abundance of empirical studies, mainly from social science scholars, on the link between education level and population health. A large part of these studies shows that education improves health outcomes, regardless of whether the focus is on individuals or country levels (Grossman, 2006; Dursun et al., 2018). Furthermore, some other scholars, such as Ross and Wu (1995) and Grossman (2006), argue that a high educational level improves health outcomes, directly or indirectly, through economic conditions, work, sociopsychological resources, and a healthy lifestyle. This study uses the gross enrollment rate in tertiary education as a measure of education. The data on this indicator is obtained from the World Bank (WDI) online database. It is expected that the impacts of investment in higher education on life expectancy and infant mortality are positive and negative, respectively.
-
Economic Growth (Y)
Historically, enhancing health outcomes has been linked to economic growth via three main mechanisms: improvements in public health infrastructure, better nutrition, and more efficient medical technologies, such as vaccines and antibiotics. The results of many studies, such as Majeed and Gilani (2017) and Majeed and Ozturk (2020), confirm that an increase in economic growth increases an individual’s income, which allows them a better diet, education, housing, and health facilities that conduct to enhance health outcomes. This study uses GDP per capita in constant 2010 US$ as a measure of economic growth. The data on GDP per capita is obtained from. The data on this indicator is sourced from the World Bank (WDI) online database. We expect that economic growth has negative and positive impacts on infant mortality and life expectancy.
Descriptive Statistics
Table 1 reports the descriptive statistics and the pairwise correlations among the different variables.
From the information reported in this table, we can see that, over the sample time, the variation of the infant mortality rate is between 6 and 18.7 deaths per 1000 live births; per capita GDP varies between 72.561 and 74.998 years; the indicators of CO2 emissions are between 11.724 and 17.691 metric tons per capita for COpc, between 47.139 and 50.486 percent of total fuel consumption for COehp, between 57.924 and 89.531 percent of total emissions for COlfc, and between 2.367 and 2.598 kg of oil equivalent energy use for COint; the R&D indicators range from 0.042 to 0.897% for the RDexp and from 0 to 233 patents for PET. Furthermore, pairwise correlations show, that, on the one hand, the infant mortality rate is positively connected to the four indicators of CO2 emissions and negatively to life expectancy, the two indicators of R&D, public health expenditure, education, and per capita GDP. On the other hand, life expectancy is negatively connected to the four indicators of CO2 emissions and positively connected to the two indicators of R&D, public health expenditure, education, and per capita GDP. Table 1 also shows that the correlation among the indicators of CO2 emissions as well as between the two proxies of R&D is positive and high. For this reason and to avoid the multicollinearity problem, the indicators of emissions and R&D are included separately in the estimated model.
Estimation Method
Before estimating our empirical model, we need first to verify the stationary properties of our variables using several unit root tests: Philippe and Perron (Philips & Perron, 1988; PP), Augmented Dickey-Fuller (Dickey & Fuller, 1981; ADF), Elliott et al., (1996; ERS), and Kwiatkowski et al., (1992; KPSS).
The results of these tests in level and first difference are reported in Table 2, which clearly shows that all of the variables, except CO2 intensity, are nonstationary at their level forms; however, they become stationary at the first difference. This means that our considered variables are integrated of order one, i.e., I(1), allowing us, therefore, to check the long-run equilibrium links between variables using the cointegration test of Johansen (1988). Table 3 reports the results of this test and shows that the trace statistics are higher than critical values at rank = 0, indicating that all models do not reject the hypothesis of cointegration. After confirming the cointegration between variables, we can run the long-term parameters in the next step using the DOLS method. The benefit of applying this method is that the endogeneity problems in serial correlations in error and regressors are often removed in a very successful manner (Omri et al., 2021). The specification for the DOLS method is identified as such:
where \({Y}_{t},X,\overrightarrow{\beta }, p, q\) are the dependent variable, the vector of explanatory variables, the cointegrating vector (the long-term impact of a fluctuation in X on Y), lag length, and lead length, respectively. The lag and lead terms used in the DOLS method are structured to distinguish its stochastic error term from all previous innovations in stochastic regressors. Tables 4 and 5 report the results of this method.
Results and Discussions
The long-run estimates among the CO2 emissions, R&D, and health outcomes are reported in Tables 4 and 5. Table 4 provides the findings on the impacts of the proxies of CO2 emissions and R&D on the rate of infant mortality.
The following are the main results obtained from this table. First, regarding the impacts of the indicators of R&D on infant mortality rate, only model 1, pertaining to CO2 emissions per capita, shows that R&D expenditures have a negative and significant impact on infant mortality. This impact is significant at the 5% level. However, models 5 to 8 show an insignificant negative impact of patents environmental-related technologies on infant mortality. The magnitude of − 0.098 indicates that a 1%-point rise in R&D expenditures lessens the infant mortality rate by 0.098%. This is because R&D has invariably enabled the development of disease control protocols, sophisticated health equipment, and elimination, treatment methods that have synergistically decreased the rates of infant mortality (Tang, 2019). The author recommends that the increase in R&D activities help stimulate innovations in care and treatment as well as the progress of advanced medical equipment and tools that will improve the supervising of the present therapeutic procedures and intervention measures. Second, it is clear from all the estimated models that, as expected, CO2 emissions have a positive impact on the infant mortality rates, ranging from 0.112 to 0.180% for the models pertaining to the R&D expenditures and from 0.183 to 0.299% for the models pertaining to patents environmental-related technologies. These results indicate that environmental degradation increases the rates of infant mortality. In this context, Bressler (2021) argues that adding 4434 metric tons of carbon dioxide in 2020 causes one more death worldwide in expectations between 2020 and 2100. Indeed, the negative influence of CO2 emissions on the mortality rates confirms the findings of Ahmed et al. (2020) who find that air pollution increases the mortality rates for 72 developing countries and the governments of these countries can moderate this positive impact by improving governance infrastructure. In the same vein, Majeed and Ozturk (2020) investigate the relationship between CO2 emissions and infant mortality for 180 countries, and they argue that countries with high levels of emissions experience high rates of infant mortality. They suggest that health-related reforms should be aligned with policies that guarantee fewer emissions and these health policies should be designed in a way that moderates the negative impacts of environmental degradation on population health. For this reason, this study seeks to examine the ability of R&D to moderate these negative impacts.
Third, we emphasize one of the central contributions of this work, i.e., examining the moderating role of R&D on the linkage between the indicators of CO2 emissions and infant mortality rates. Following the studies of Tchamyou et al. (2019), Omri (2020), and Omri et al. (2021), among others, net impacts are calculated to analyze the overall impact of the interaction between CO2 emissions and infant mortality. For each estimated model, a negative net impact means that the complementarity between CO2 emissions and R&D reduces the rates of infant mortality; however, a positive net impact implies that R&D cannot reduce the incidence of emissions on infant mortality. Among all the estimated models, it is only in model 1(COpc) pertaining to the R&D expenditures that the net impact on infant mortality from the complementarity between R&D expenditures and per capita CO2 emissions is negative, i.e., − 0.017 [(− 0.390 × 0.349) + 0.117]. In this formula, 0.349 is the mean value of R&D expenditures, − 0.390 is the marginal impact from increasing R&D expenditures, and 0.117 is the unconditional impact of per capita CO2 emissions. It is clear that when adding R&D expenditures in the estimated model, the overall impact becomes negative in affecting infant mortality. This suggests that when promoting the R&D initiatives, the positive impact of per capita CO2 emissions can be moderated. Accordingly, we can say that the expenditures on R&D influence population health outcomes more effectively when it is directly targeted towards environmental degradation. On the other hand, we can see that models 2 and 3 pertaining to R&D expenditures show that the net impacts on the rates of infant mortality are positive from the interactions between R&D expenditures and (i) CO2 emissions from electricity and heat production (0.071) and (ii) CO2 from liquid fuel consumption (0.044). Fourth, for these net positive impacts, the corresponding marginal effects are negative and significant, meaning that at a given threshold of R&D expenditures, the net positive impacts on infant mortality can be transformed from positive to negative. The corresponding threshold of R&D expenditures that reduce infant mortality rate is 0.58% of GDP for both CO2 emissions from electricity and heat production (0.180/0.310) and CO2 from liquid fuel consumption (0.112/0.193). Since R&D expenditures range from 0.042 to 0.897%, the computed thresholds of R&D expenditures make economic sense and have policy significance (Omri & Belaid, 2021). Thus, increasing R&D expenditures to above 0.58% would reduce CO2 emissions from electricity and heat production and CO2 from liquid fuel consumption and then reduce the rates of infant mortality.
We then re-estimated the models in Table 4 by replacing the health outcome indicator with life expectancy. Table 5 reports the main findings of these re-estimations. First, regarding the impact of the two indicators of R&D on life expectancy at birth, all the estimated models show that this impact is positive but insignificant, meaning that, at present, the level of R&D in Saudi Arabia does not have a significant impact on increasing life expectancy at birth. Second, as expected, all the estimated models show that CO2 emissions reduce life expectancy, ranging from − 0.104 to − 0.290% for the models pertaining to the R&D expenditures and from − 0.145 to − 0.598% for the models pertaining to patents environmental-related technologies. The same result was found by Rodriguez-Alvarez (2021) who examines the contribution of air pollution, including CO2 emissions, for 29 European countries, and he confirms that CO2 emissions reduce life expectancy at birth. The author calls these countries to more investments in renewable energy to reduce the incidence of air pollution on life expectancy. Similarly, de Keijzer et al. (2017) conducted a global study focused on CO2 emission impacts on life expectancy, and they confirm the negative impact of CO2 emissions on life expectancy. They conclude that a country with a high level of emissions suffers from depressed life expectancy, suggesting that health reforms compatible with a reduction of CO2 emissions should be a priority for public health. However, this result is in contradiction with Bayati et al. (2013) who investigate the determinants of life expectancy for 21 Eastern Mediterranean countries, and they show that the impact of per capita CO2 emissions was insignificant on life expectancy. Third, we emphasize another contribution to previous literature, i.e., examining the role of R&D in modulating the link between the indicators of CO2 emissions and life expectancy. Net impacts are calculated to demonstrate the global impact of the interplay between CO2 emissions and life expectancy. For each estimated model, a positive net impact means that R&D modulates the negative effect of CO2 emissions on life expectancy; however, a negative net impact means that R&D cannot lessen the negative effect of emissions on life expectancy. Among all the estimated models, it is only in model 1(COpc) pertaining to the R&D expenditures that the net impact on life expectancy from the interaction between R&D expenditures and per capita CO2 emissions is positive, i.e., 0.010 [(0.410 × 0.349) + (− 0.133)]. In this formula, 0.349 is the mean value of R&D expenditures, 0.410 is the marginal effect from increasing R&D expenditures, and − 0.133 is the unconditional impact of per capita CO2 emissions. It is clear that when adding R&D expenditures in the estimated model, the overall impact becomes positive in influencing life expectancy, indicating when the R&D initiatives were increased, the negative impact of per capita CO2 emissions on life expectancy can be modulated. Therefore, we can say that R&D increases population health outcomes more effectively when it is directly targeted towards reducing environmental pollution. On the other hand, we can see that models 2 and 3 pertaining to R&D expenditures and model 5 pertaining to patents environmental-related technologies show that the net impacts on life expectancy are positive from the interplays between R&D expenditures and (i) CO2 emissions from electricity and heat production (− 0.072) and (ii) CO2 from liquid fuel consumption (− 0.043) and between patents environmental-related technologies and per capita CO2 emissions. Fourth, for these net negative impacts, the corresponding marginal impacts are positive and significant, indicating that (i) at a given threshold of R&D expenditures, the net negative impacts on life expectancy can be transformed from negative to positive. The corresponding threshold of R&D expenditures that increase life expectancy is 0.60% of GDP for both CO2 emissions from electricity and heat production (0.196/0.326) and CO2 from liquid fuel consumption (0.104/0.174). Since R&D expenditures range from 0.042 to 0.897%, the calculated thresholds of R&D expenditures have policy significance and make economic sense (Omri & Belaid, 2021). Thus, increasing R&D expenditures to above than 0.6% of GDP would reduce CO2 emissions from electricity and heat production and CO2 from liquid fuel consumption and then increase life expectancy; (ii) at a certain threshold level of environmentally related R&D, the net negative impact on life expectancy can be changed from negative to positive. The corresponding threshold of patents environmental-related technologies that increase life expectancy is 100 patents for the model pertaining to per capita CO2 emissions (0.598/0.006). Since the number of patents environmental-related technologies ranges from 0 and 233, the calculated threshold of this later makes economic sense and has policy significance.
In summary, to modulate the negative impacts of CO2 emissions on health outcomes, the findings found in Tables 4 and 5 show that the spending on R&D must be more than 0.6% of GDP and the number of patents environmental-related technologies must be more than 100. These tables also show that, as expected, (i) public health expenditures promote health outcomes, i.e., reducing infant mortality and increasing life expectancy. This result is in line with those of Gupta et al. (2002) and Majeed and Ozturk (2020); (ii) education level, particularly tertiary education, improves population health as educated people can avoid unhealthy habits and diets (Khan & Majeed, 2019); (iii) economic growth also contributes positively to population health, meaning that when the average level of income is high in a given country, the government of that country has more resources to spend on improving the health of their residents, and these later, through increasing income, will have more resources to afford better shelter, food, and healthcare facilities (Majeed & Ozturk, 2020).
For robustness purposes, we also estimate Eq. 4 using a fully modified ordinary least squares (FMOLS) method to confirm the results of the DOLS method. The results of the FMOLS method are reported in Tables 6 and 7. The followings are the main findings found from the FMOLS estimates: First, as shown in the DOLS estimates, both indicators of R&D have positive (negative) and an insignificant impact on life expectancy (infant mortality), indicating that, at present, the level of R&D in Saudi Arabia does not have a significant impact on increasing life expectancy at birth and reducing infant mortality. Second, all the estimated models confirm that CO2 emissions decrease life expectancy and increase infant mortality. Third, R&D expenditures enhance health outcomes by reducing per capita CO2 emissions; i.e., R&D expenditures could modulate the negative impacts of CO2 emissions on human health. Fourth, R&D expenditures interact with CO2ehp and CO2lfc to negatively influence life expectancy and to positively influence infant mortality. To modulate these negative impacts on health outcomes, the corresponding R&D threshold was calculated and discussed. The calculated thresholds also show that increasing R&D expenditures to above 0.6% of GDP would reduce CO2 emissions from electricity and heat production and CO2 from liquid fuel consumption and then increase life expectancy and reduce infant mortality. These results confirm those obtained from the DOLS method.
Conclusions and Implications
This study extends the ongoing health economics literature by investigating the joint effects of R&D (expenditures and environmentally related R&D) and CO2 emissions on population health outcomes (infant mortality and life expectancy). As discussed above, the theoretical health production function of Grossman (1972) was extended by including CO2 emissions, R&D, their interaction terms, and other socioeconomic indicators as inputs. In this study, R&D has been included as a policy variable that modulates the negative incidences of CO2 emissions on population health outcomes for Saudi Arabia for the 2000–2018 period. Different indicators of CO2 emissions are included in the analysis. Required pre-estimations tests, such as unit root and Johansen’s (1988) cointegration test, and the DOLS technique to run the long-run estimates are used. Our empirical analysis shows that (i) there are negative unconditional effects of CO2 emissions on health outcomes in all the estimated models; (ii) R&D expenditures have a weak direct impact on health outcomes; (iii) in addition to their direct effects on health outcomes, R&D expenditures remarkably enhanced health outcomes through reducing per capita CO2 emissions; and (iv) R&D expenditures interact with CO2ehp and CO2lfc to negatively influence health outcomes. Similarly, environmentally related R&D, measured by patents environmental-related technologies, interacts with per capita CO2 emissions to negatively influence health outcomes. To modulate these negative impacts, the corresponding R&D threshold was calculated and discussed.
There are also important policy and practical implications to be drawn from this work. From a policy viewpoint, policymakers in Saudi Arabia should give more and more incentives for R&D to reduce emissions and then improve health outcomes. As the healthcare sector is leading the way in Saudi Arabia in terms of innovation, investments in R&D should be designed in a way that boosts relevant scientific research related to health and the environment. It is substantial to note that the design of R&D should be connected to national and international policies, particularly policies related to environmental and health research, health manufacturing, and health information and communication technologies. We also support the incentive for R&D through tax exemptions, grants, subsidies, and other similar financial measures that will boost R&D in healthcare, which, in turn, will produce procedures and products that will improve population health outcomes. Since Saudi Arabia is among the ten top emitters in the world, government efforts must be strictly focused on supporting and promoting R&D programs directly linked to CO2 emissions and increasing their use. These programs should be oriented to attach green R&D policies with sustainable development goals and conduct a comprehensive shift from fossil to renewable resources (Magazzino et al., 2021b). Policymakers should consider the characteristics of the effect of different green R&D initiatives on CO2 emissions when preparing relevant policies. From a practical viewpoint, corporates and firms’ decision-makers must integrate environmental sustainability into firms’ decision-making, which opens up new opportunities leading to better environmental and financial performance. Thus, more investments in green R&D can result in a reduction in CO2 emissions and positive financial performance (Lee et al., 2015). Moreover, we suggest the centralization of R&D in dedicated childcare institutions in which private and governmental establishment can pool their expertise and financial resources to yield practical solutions aimed at reducing the rates of infant mortality. Finally, effective R&D operations demand significant collaboration between researchers from several domains. For example, to be maximally productive, investment in healthcare R&D fields requires to include investment in numerous other relevant domains, such as biology, physical sciences, chemistry, economics, and ICT. Furthermore, in light of the global objective of supporting investment in healthcare R&D, as reported in the national development plan, diverse related academic domains need also to take further support.
Despite these interesting findings, policy, and practical implications, we are cautious to indicate that our study suffers from some limits that should be pointed out: First, this study has certain limitations. First, environmental quality is only measured using four indicators of CO2 emissions; however, some other indicators, such as PM2.5 and NO2, among others, could be included in future studies. Second, CO2 emissions also affect mental health, whereas this article only focuses only on physical health. Because of the data limitations, this study uses two broader measures of health outcomes. Future studies can focus on other measures of health outcomes.
Data availability
The data are available upon demand by request to the corresponding author.
References
Abid, A., Mehmood, U., Tariq, S., & Haq, Z. U. (2022). The effect of technological innovation, FDI, and financial development on CO2 emission: Evidence from the G8 countries. Environmental Science and Pollution Research, 29(8), 11654–11662.
Ahmed, Z., Ali, S., Saud, S., & Shahzad, S. J. H. (2020). Transport CO2 emissions, drivers, and mitigation: an empirical investigation in India. Air Quality, Atmosphere & Health, 13(11), 1367–1374.
Arora, S., & Cason, T. N. (1996). Why do firms volunteer to exceed environmental regulations? Understanding participation in EPA’s 33/50 Program. Land Economics, 72(4), 413–432. https://doi.org/10.2307/3146906
Arthur, E., & Oaikhenan, H. E. (2017). The effects of health expenditure on health outcomes in Sub‐Saharan Africa (SSA). African Development Review, 29(3), 524–536.
Bayati, M., Akbarian, R., & Kavosi, Z. (2013). Determinants of life expectancy in eastern Mediterranean region: A health production function. International Journal of Health Policy and Management, 1(1), 57.
Blaya, J. A., Fraser, H. S., & Holt, B. (2010). E-health technologies show promise in developing countries. Health Affairs, 29(2), 244–251.
Bressler, R. D. (2021). The mortality cost of carbon. Nature Communications, 12(1), 1–12.
Callaghan, C. W., Callaghan, N. C., & Jogee, R. (2019). Inequality in healthcare R&D outcomes: A model of process disruption. Development Southern Africa, 36(6), 874–888.
Cao, J., Yang, C., Li, J., Chen, R., Chen, B., Gu, D., & Kan, H. (2011). Association between long-term exposure to outdoor air pollution and mortality in China: A cohort study. Journal of Hazardous Materials, 186(2–3), 1594–1600.
Churchill, S. A., Inekwe, J., Smyth, R., & Zhang, X. (2019). R&D intensity and carbon emissions in the G7: 1870–2014. Energy Economics, 80, 30–37.
Costello, A., Abbas, M., Allen, A., Ball, S., Bell, S., Bellamy, R., ... & Patterson, C. (2009). Managing the health effects of climate change: Lancet and University College London Institute for Global Health Commission. The Lancet, 373(9676), 1693–1733.
Darçın, M. (2017). How air pollution affects subjective well-being. Well-being and Quality of Life: Medical Perspective, 211.
de Keijzer, C., Agis, D., Ambrós, A., Arévalo, G., Baldasano, J. M., Bande, S., … & MED-HISS Study group. (2017). The association of air pollution and greenness with mortality and life expectancy in Spain: A small-area study. Environment International, 99, 170–176.
Dickey, D. A., & Fuller, W. A. (1981). Likelihood ratio statistics for autoregressive time series with a unit root. Econometrica: Journal of the Econometric Society, 1057–1072.
Dinda, S. (2004). Environmental Kuznets curve hypothesis: A survey. Ecological Economics, 49, 431–455.
Dong, H., Xue, M., Xiao, Y., & Liu, Y. (2021). Do carbon emissions impact the health of residents? Considering China’s industrialization and urbanization. Science of the Total Environment, 758, 143688.
Dursun, B., Cesur, R., & Mocan, N. (2018). The impact of education on health outcomes and behaviors in a middle-income, low-education country. Economics & Human Biology, 31, 94–114.
Elliott, G., Rothenberg, T. J., & Stock, J. H. (1996). Efficient tests for an autoregressive unit root. Econometrica, 64, 813–836
Erdoğan, S., Yıldırım, D. Ç., & Gedikli, A. (2019). The relationship between CO2 emissions and health indicators: The case of Turkey. Economic Letters, 6(1), 28–39.
Faria, J. R., Caudill, S. B., Mixon, F. G., Jr., & Upadhyaya, K. P. (2021). Cooperation and spillovers in healthcare R&D: Theory and evidence. Economic Modelling, 95, 68–75.
Farooq, M. U., Shahzad, U., Sarwar, S., & ZaiJun, L. (2019). The impact of carbon emission and forest activities on health outcomes: Empirical evidence from China. Environmental Science and Pollution Research, 26(13), 12894–12906.
Fayissa*, B., & Gutema, P. (2005). Estimating a health production function for Sub-Saharan Africa (SSA). Applied Economics, 37(2), 155–164.
Fernández, Y. F., López, M. F., & Blanco, B. O. (2018). Innovation for sustainability: The impact of R&D spending on CO2 emissions. Journal of Cleaner Production, 172, 3459–3467.
Garrone, P., & Grilli, L. (2010). Is there a relationship between public expenditures in energy R&D and carbon emissions per GDP? An Empirical Investigation. Energy Policy, 38(10), 5600–5613.
Grossman, L. (1972). Condensation in the primitive solar nebula. Geochimica et Cosmochimica Acta, 36(5), 597–619.
Grossman, M. (2006). Education and nonmarket outcomes. Handbook of the Economics of Education, 1, 577–633.
Gupta, S., Verhoeven, M., & Tiongson, E. R. (2002). The effectiveness of government spending on education and health care in developing and transition economies. European Journal of Political Economy, 18(4), 717–737.
Guo, Q., & Luo, K. (2021). The spatial convergence and drivers of environmental efficiency under haze constraints-Evidence from China. Environmental Impact Assessment Review, 86, 106513.
Hashim, D., & Boffetta, P. (2014). Occupational and environmental exposures and cancers in developing countries. Annals of Global Health, 80(5), 393–411.
Johansen, S. (1988). Statistical analysis of cointegration vectors. Journal of Economic Dynamics and Control, 12(2–3), 231–254.
Kingdom of Saudi Arabia. (2019). KSA Vision 2030: Strategic objectives and vision realization programs. https://vision2030.gov.sa/sites/default/files/report/Vision%20Realization%20Programs%20Overview.pdf
Kiross, G. T., Chojenta, C., Barker, D., & Loxton, D. (2020). The effects of health expenditure on infant mortality in sub-Saharan Africa: Evidence from panel data analysis. Health Economics Review, 10(1), 1–9.
Kwiatkowski, D., Phillips, P. C ., Schmidt, C., & Shin, Y. (1992). Testing the null hypothesis of stationarity against the alternative of a unit root: How sure are we that economic time series have a unit root? Journal of Econometrics, 54, 159–178.
Lee, K. H., & Min, B. (2015). Green R&D for eco-innovation and its impact on carbon emissions and firm performance. Journal of Cleaner Production, 108, 534–542.
Li, M., & Wang, Q. (2017). Will technology advances alleviate climate change? Dual effects of technology change on aggregate carbon dioxide emissions. Energy for Sustainable Development, 41, 61–68.
Liu, L., Wang, K., Wang, S., Zhang, R., & Tang, X. (2018). Assessing energy consumption, CO2 and pollutant emissions and health benefits from China’s transport sector through 2050. Energy Policy, 116, 382–396.
Lucas, H. (2008). Information and communications technology for future health systems in developing countries. Social Science & Medicine, 66(10), 2122–2132.
Magazzino, C. (2017a). The relationship among economic growth, CO2 emissions, and energy use in the APEC countries: A panel VAR approach. Environment Systems and Decisions, 37(3), 353–366.
Magazzino, C. (2017b). Economic growth, CO2 emissions and energy use in the South Caucasus and Turkey: A PVAR analyses. International Energy Journal, 16(4), 153–162.
Magazzino, C. (2019). Testing the stationarity and convergence of CO2 emissions series in MENA countries. International Journal of Energy Sector Management, 13, 977–990.
Magazzino, C., Mele, M., & Sarkodie, S. A. (2021a). The nexus between COVID-19 deaths, air pollution and economic growth in New York state: Evidence from deep machine learning. Journal of Environmental Management, 286, 112241.
Magazzino, C., Mele, M., & Schneider, N. (2021b). A machine learning approach on the relationship among solar and wind energy production, coal consumption, GDP, and CO2 emissions. Renewable Energy, 167, 99–115.
Majeed, M. T., & Gillani, S. (2017). State capacity and health outcomes: An empirical Analysis. Pakistan Journal of Commerce and Social Sciences (PJCSS), 11(2), 671–697
Majeed, M. T., & Khan, F. N. (2019). Do information and communication technologies (ICTs) contribute to health outcomes? An Empirical Analysis. Quality & Quantity, 53(1), 183–206.
Majeed, M. T., & Ozturk, I. (2020). Environmental degradation and population health outcomes: A global panel data analysis. Environmental Science and Pollution Research, 27(13), 15901–15911.
Martins, F., Felgueiras, C., & Smitková, M. (2018). Fossil fuel energy consumption in European countries. Energy Procedia, 153, 107–111.
Mele, M., Magazzino, C., Schneider, N., & Strezov, V. (2021). NO2 levels as a contributing factor to COVID19 deaths: The first empirical estimate of threshold values. Environmental research, 194, 110663.
Nasreen, S. (2021). Association between health expenditures, economic growth and environmental pollution: Long‐run and causality analysis from Asian economies. The International Journal of Health Planning and Management, 36(3), 925–944.
Omri, A. (2020). Formal versus informal entrepreneurship in emerging economies: The roles of governance and the financial sector. Journal of Business Research, 108, 277–290.
Omri, A., & Belaïd, F. (2021). Does renewable energy modulate the negative effect of environmental issues on the socio-economic welfare?. Journal of Environmental Management, 278, 111483.
Omri, A., & Mabrouk, N. B. (2020). Good governance for sustainable development goals: Getting ahead of the pack or falling behind?. Environmental Impact Assessment Review, 83, 106388.
Omri, A., & Saidi, K. (2022). Factors influencing CO2 emissions in the MENA countries: the roles of renewable and non-renewable energy. Environmental Science and Pollution Research, 1–12.
Omri, A., Euchi, J., Hasaballah, A. H., & Al-Tit, A. (2019). Determinants of environmental sustainability: evidence from Saudi Arabia. Science of the Total Environment, 657, 1592–1601.
Omri, A., Kahia, M., & Kahouli, B. (2021). Does good governance moderate the financial development-CO2 emissions relationship?. Environmental Science and Pollution Research, 28(34), 47503–47516.
Paruk, F., Blackburn, J. M., Friedman, I. B., & Mayosi, B. M. (2014). National expenditure on health research in South Africa: What is the benchmark? South African Medical Journal, 104(7), 468–474.
Petrović, P., & Lobanov, M. M. (2020). The impact of R&D expenditures on CO2 emissions: Evidence from sixteen OECD countries. Journal of Cleaner Production, 248, 119187.
Phillips, P. & Perron, P. (1988). Testing for a unit root in time series regression. Biometrika, 75, 335–346.
Rodriguez-Alvarez, A. (2021). Air pollution and life expectancy in Europe: Does investment in renewable energy matter. The Science of the Total Environment, 792, 148480.
Ross, C. E., & Wu, C. L. (1995). The links between education and health. American Sociological Review, 719–745.
Sechzer, P. H., Egbert, L. D., Linde, H. W., Cooper, D. Y., Dripps, R. D., & Price, H. L. (1960). Effect of CO2 inhalation on arterial pressure, ECG and plasma catecholamines and 17-OH corticosteroids in normal man. Journal of Applied Physiology, 15(3), 454–458.
Seppänen, O. A., Fisk, W. J., & Mendell, M. J. (1999). Association of ventilation rates and CO2 concentrations with health and other responses in commercial and institutional buildings. Indoor Air, 9(4), 226–252.
Shahbaz, M., Nasir, M. A., & Roubaud, D. (2018). Environmental degradation in France: The effects of FDI, financial development, and energy innovations. Energy Economics, 74, 843–857.
Shobande, O. A. (2020). The effects of energy use on infant mortality rates in Africa. Environmental and Sustainability Indicators, 5, 100015.
Sileem, H. H. M. (2016). Health expenditure, climate changes and corruption in the MENA region: a granger causality approach. Journal of African Development, 18(2), 61–72.
Sirag, A., Mohamed Nor, N., Law, S. H., Abdullah, N. M. R., & Lacheheb, M. (2017). The impact of health financing and CO2 emission on health outcomes in Sub-Saharan Africa: A cross-country analysis. GeoJournal, 82(6), 1247–1261.
Tang, C. F. (2019). Determinants of infant mortality rate in Malaysia: Evidence from dynamic panel data study. Journal of Health Management, 21(4), 443–450.
Tchamyou, V. S., Asongu, S. A., & Odhiambo, N. M. (2019). The role of ICT in modulating the effect of education and lifelong learning on income inequality and economic growth in Africa. African Development Review, 31(3), 261–274.
Tsai, Y. Y., Chao, C. M., Lin, H. M., & Cheng, B. W. (2018). Nursing staff intentions to continuously use a blended e-learning system from an integrative perspective. Quality & Quantity, 52(6), 2495–2513.
Urhie, E., Afolabi, A., Afolabi, A., Matthew, O., Osabohien, R., & Ewetan, O. (2020). Economic growth, air pollution and health outcomes in Nigeria: A moderated mediation model. Cogent Social Sciences, 6(1), 1719570.
USGCRP. (2009). Global climate change impacts in the United States. In: Karl TR, Melillo JM, Peterson TC, editors. Climate Change Impacts by Sectors: Ecosystems. New York, NY: United States Global Change Research Program. Cambridge University Press.
Wald, H. S., Dube, C. E., & Anthony, D. C. (2007) .Untangling the Web—The impact of Internet use on health care and the physician–patient relationship. Patient Education and Counseling, 68(3), 218–224.
Watts, N., Amann, M., Arnell, N., Ayeb-Karlsson, S., Belesova, K., Berry, H., ... & Costello, A. (2018). The 2018 report of the Lancet Countdown on health and climate change: Shaping the health of nations for centuries to come. The Lancet, 392(10163), 2479–2514.
Wesseler, J., & Zhao, J. (2019). Real options and environmental policies: The good, the bad, and the ugly. Annual Review of Resource Economics, 11, 43–58.
Zhang, Y.-J., Peng, Y.-L., Ma, C.-Q., & Shen, B. (2017). Can environmental innovation facilitate carbon emissions reduction? Evidence from China. Energy Policy, 100, 18–28.
Acknowledgements
The authors gratefully acknowledge Qassim University, represented by the Deanship of Scientific Research, on the financial support for this research under the number 10351-cbe-2020-1-3-I during the academic year 1442AH/2020 AD.
Funding
This research was funded by Qassim University in Saudi Arabia under grant number 10351-cbe-2020–1-3-I.
Author information
Authors and Affiliations
Contributions
Anis Omri: Conceptualization, methodology, and project administration. Bassem Kahouli: Formal analysis and software. Hatem Afi: Investigation and data collection. Montassar Kahia: Formal analysis and software.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Omri, A., Kahouli, B., Afi, H. et al. Impact of Environmental Quality on Health Outcomes in Saudi Arabia: Does Research and Development Matter?. J Knowl Econ 14, 4119–4144 (2023). https://doi.org/10.1007/s13132-022-01024-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13132-022-01024-8