
Abstract
Background — Aim
Clinical studies over the last ten years have shown that preoperative enteral immunonutrition after major gastrointestinal operations reduces morbidity and improves outcome. Similar results have been reported with the application of Enhanced Recovery After Surgery (ERAS) programmes. The aim of this study was to determine whether the addition of preoperative enteral immunonutrition to an ERAS program further decreases postoperative morbidity and the length of hospital stay in patients undergoing major gastrointestinal surgery.
Patients-Methods
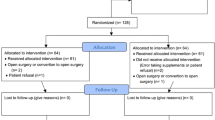
A retrospective study was conducted of 19 patients who, over a six-month period, had undergone a planned elective operation for benign or malignant intra-abdominal illness and were treated according to an ERAS program. Before surgery, 10 patients (group A) received 900 ml/day of an immune-enhancing oral diet for 6 days before surgery, together with normal food, while the remaining 9 patients (group B) just received a normal diet. Statistical analysis was done by the use of Fisher’s exact test and Mann-Whitney test.
Results
All surgical procedures were performed by the same surgical team. The two groups were comparable, in terms of age, gender, ASA grade, nutritional status, type of disease and type of surgery. Complication rates were 20% in group A, and 10% in group B (p=0.5). Furthermore, no significant differences between the two groups were found with regard to mortality and length of hospital stay. However, the comparison of the duration of stay in upper and lower gastrointestinal surgery revealed that patients in Group A who underwent surgery in the lower abdomen had a significantly shorter length of hospital stay compared with their counterparts in Group B (p=0.03).
Conclusion
In patients who undergo major intra-abdominal surgery, treated with an ERAS regimen, the preoperative administration of immune-enhancing diet does not further reduce morbidity and mortality. However, it enables a shorter length of hospital stay, particularly for those undergoing surgery of the lower abdomen.
Similar content being viewed by others


References
Meakins JL. Host defense mechanisms in surgical patients: effects of surgery and trauma. Acta Chir Scand 1989;550(suppl): 43–51.
Chang HR, Bistrian B. The role of cytokines in the catabolic consequences of infection and injury. JPEN 1998;22:156–166.
Sax HC. Immunonutrition and upper gastrointestinal surgery: what really matters? Nutr Clin Pract 2005;20(5):540–543.
Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg 2002;183(6):630–641.
Zarger-Shoshtari K, Hill AG. Optimization of perioperative care for colonic surgery: a review of the evidence. ANZ Journal of Surgery 2008;78(1–2):13–23.
Gianotti L, Braga M, Fortis C et al. A prospective, randomized clinical trial on perioperative feeding with arginine, omega-e fatty acids and RNA-enriched enteral diet: Effect on host response and nutritional status. JPEN 1999;23:314–320.
Braga M, Gianotti L, Vignali A et al. Preoperative oral arginine and n-3 fatty acid supplementation improves the immunometabolic host response and outcome after colorectal resection for cancer. Surgery 2002;132:805–814.
Alvarez W, Mobarhan S. Finding a place for immunonutrition. Nutr Rev 2003;61:214–218.
Lassen K, Soop M, Nygren J et al. Consensus review of optimal perioperative care in colorectal surgery: Enhanced Recovery After Surgery (ERAS) Group recommendations. Arch Surg 2009;144(10):961–969.
Heys SD, Walker LG, Smith I et al. Enteral nutrition supplementation with key nutrients in patients with critical illness and cancer: a meta-analysis of randomized controlled clinical trials. Ann Surg 1999;229:467–477.
Gianotti L, Braga M, Neapoli L et al. A randomized controlled trial on preoperative oral supplementation with a specialized diet in patients with gastrointestinal cancer. Gastroenterology 2002;122:1763–1770.
Braga M, Gianotti L. Preoperative immunonutrition: cost benefit analysis. JPEN 2005;29(suppl):S57–S61.
Walter CJ, Collin L, Dumville JC et al. Enhanced recovery in colorectal resections: a systematic review and meta-analysis. Colorectal Dis 2009;11(4):344–353.
Eskicioglou C, Forbess SS, Aarts MA et al. Enhanced recovery after surgery (ERAS) programs for patients having colorectal surgery: a meta-analysis of randomized trials. J Gastrointest Surg 2009;13(12):2321–2329.
Varadhan KK, Neal KR, Dejong CH et al. The enhanced recovery after surgery (ERAS) pathway for patients undergoing major elective open colorectal surgery: a meta-analysis of randomized controlled trials. Clin Nutr 2010;29(4):434–440.
Lassen K, Kjaeve J, Fetveit T et al. Allowing normal food at will after major upper gastrointestinal surgery does not increase morbidity: a randomized multicenter trial. Ann Surg 2008;247(5):721–729.
Charoenkwan K, Phillipson G, Vutyavanich T. Early versus delayed (traditional) oral fluids and food for reducing complications after major abdominal gynaecologic surgery. Cochrane Database Syst Rev 4 2007;CD004508.
Pruthi RS, Chun J, Richman M. Reducing time to oral diet and hospital discharge in patients undergoing radical cystectomy using a perioperative care plan. Urology 2003;62(4):661–665.
Teeuwen PH, Bleichrodt RP, Strik C et al. Enhanced recovery after surgery (ERAS) versus conventional postoperative care in colorectal surgery. J Gastrointest Surg 2010;14(1):88–95.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Alivizatos, V., Gavala, V., Athanasopoulos, P. et al. The place of preoperative immunonutrition in the era of fast-track surgery. Hellenic J Surg 84, 225–229 (2012). https://doi.org/10.1007/s13126-012-0033-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13126-012-0033-x