
Abstract
Background
Endoscopic ultrasound (EUS)-guided drainage is the standard of care for drainage of pancreatic necrosis. Though initially it was mainly used for drainage of only walled-off necrosis, recently, a few studies have also shown its safety in the management of acute necrotic collections. We did a retrospective study to evaluate the safety and efficacy of EUS-guided drainage in the early phase of pancreatitis as compared to interventions in the late phase.
Methods
We retrieved baseline disease-related, procedure-related and outcome-related details of patients who underwent EUS-guided drainage of pancreatic necrosis. Patients were divided into early (≤ 28 days from onset of pancreatitis) or delayed (> 28 days) drainage groups. Both groups were compared for disease-related characteristics and outcomes.
Results
Total 101 patients were included in the study. The mean age of included patients was 35.54 ± 13.58 years and 75 were male. Thirty-five patients (34.7%) underwent early drainage. In the early group, a majority of patients underwent intervention due to infected collection (88.6% vs. 18.2%; p < 0.001). More patients in the early group had < 30% wall formation (28.6% vs. 0%; p < 0.001) and > 30% solid debris within the collection (42.9% vs. 15.2%; p = 0.005). Patients in the early group were also more likely to require endoscopic necrosectomy (57.1% vs. 27.3%; p = 0.003) and additional percutaneous drainage (31.4% vs. 12.1%; p = 0.018). Overall, three patients in the early group and one patient in the delayed group had procedure-related complications. Four patients in the early group and one patient in the delayed group succumbed to illness (p = 0.029).
Conclusion
Though delayed interventions remain standard of care in the management of acute pancreatitis, some patients may require early intervention due to infected collection with deteriorating clinical status. Early EUS-guided interventions in such carefully selected patients have in similar clinical outcomes and complication rates compared to delayed intervention. However, such patients are more likely to require additional endoscopic or percutaneous interventions.
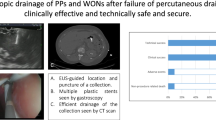
Graphical abstract



Similar content being viewed by others


Data availability
De-identified data will be available on a reasonable request from the corresponding author.
References
Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis–2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62:102–11.
van Santvoort HC, Besselink MG, Bakker OJ, et al. A step-up approach or open necrosectomy for necrotizing pancreatitis. N Engl J Med. 2010;362:1491–502.
Tenner S, Baillie J, DeWitt J, Vege SS, American College of Gastroenterology. American College of Gastroenterology guideline: management of acute pancreatitis. Am J Gastroenterol. 2013;108:1400–15; 1416.
Lakhtakia S, Basha J, Talukdar R, et al. Endoscopic “step-up approach” using a dedicated biflanged metal stent reduces the need for direct necrosectomy in walled-off necrosis (with videos). Gastrointest Endosc. 2017;85:1243–52.
van Brunschot S, van Grinsven J, van Santvoort HC, et al. Endoscopic or surgical step-up approach for infected necrotising pancreatitis: a multicentre randomised trial. Lancet. 2018;391:51–8.
Isayama H, Nakai Y, Rerknimitr R, et al. Asian consensus statements on endoscopic management of walled-off necrosis Part 1: epidemiology, diagnosis, and treatment. J Gastroenterol Hepatol. 2016;31:1546–54.
Baron TH, DiMaio CJ, Wang AY, Morgan KA. American Gastroenterological Association Clinical Practice Update: management of pancreatic necrosis. Gastroenterology. 2020;158:67-75.e1.
Besselink MGH, Verwer TJ, Schoenmaeckers EJP, et al. Timing of surgical intervention in necrotizing pancreatitis. Arch Surg Chic Ill. 1960;2007:1194–201.
Fernández-del Castillo C, Rattner DW, Makary MA, Mostafavi A, McGrath D, Warshaw AL. Débridement and closed packing for the treatment of necrotizing pancreatitis. Ann Surg. 1998;228:676–84.
Singh AK, Samanta J, Gulati A, et al. Outcome of percutaneous drainage in patients with pancreatic necrosis having organ failure. HPB (Oxford). 2021;23:1030–8.
Trikudanathan G, Tawfik P, Amateau SK, et al. Early (<4 weeks) versus standard (≥ 4 weeks) endoscopically centered step-up interventions for necrotizing pancreatitis. Am J Gastroenterol. 2018;113:1550–8.
Oblizajek N, Takahashi N, Agayeva S, et al. Outcomes of early endoscopic intervention for pancreatic necrotic collections: a matched case-control study. Gastrointest Endosc. 2020;91:1303–9.
Rana SS, Verma S, Kang M, Gorsi U, Sharma R, Gupta R. Comparison of endoscopic versus percutaneous drainage of symptomatic pancreatic necrosis in the early (< 4 weeks) phase of illness. Endosc Ultrasound. 2020;9:402–9.
Chantarojanasiri T, Yamamoto N, Nakai Y, et al. Comparison of early and delayed EUS-guided drainage of pancreatic fluid collection. Endosc Int Open. 2018;6:E1398-405.
Boxhoorn L, van Dijk SM, van Grinsven J, et al. Immediate versus postponed intervention for infected necrotizing pancreatitis. N Engl J Med. 2021;385:1372–81.
Bang JY, Navaneethan U, Hasan MK, Sutton B, Hawes R, Varadarajulu S. Non-superiority of lumen-apposing metal stents over plastic stents for drainage of walled-off necrosis in a randomised trial. Gut. 2019;68:1200-9.
Gupta P, Bansal A, Samanta J, et al. Larger bore percutaneous catheter in necrotic pancreatic fluid collection is associated with better outcomes. Eur Radiol. 2021;31:3439–46.
Cotton PB, Eisen GM, Aabakken L, et al. A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc. 2010;71:446–54.
Mier J, León EL, Castillo A, Robledo F, Blanco R. Early versus late necrosectomy in severe necrotizing pancreatitis. Am J Surg. 1997;173:71–5.
Hungness ES, Robb BW, Seeskin C, Hasselgren P-O, Luchette FA. Early debridement for necrotizing pancreatitis: is it worthwhile? J Am Coll Surg. 2002;194:740–4 (discussion 744-5).
Rana SS, Sharma R, Kishore K, Dhalaria L, Gupta R. Safety and efficacy of early (<4 weeks of illness) endoscopic transmural drainage of post-acute pancreatic necrosis predominantly located in the body of the pancreas. J Gastrointest Surg. 2021;25:2328–35.
Rana SS, Bhasin DK, Reddy YR, et al. Morphological features of fluid collections on endoscopic ultrasound in acute necrotizing pancreatitis: do they change over time? Ann Gastroenterol. 2014;27:258–61.
Rana SS, Bhasin DK, Sharma RK, Kathiresan J, Gupta R. Do the morphological features of walled off pancreatic necrosis on endoscopic ultrasound determine the outcome of endoscopic transmural drainage? Endosc Ultrasound. 2014;3:118–22.
Seicean A, Pojoga C, Mostean O, et al. What is the impact of the proportion of solid necrotic content on the number of necrosectomies during EUS-guided drainage using lumen-apposing metallic stents of pancreatic walled-off necrosis ? J Gastrointest Liver Dis. 2020;29:623–8.
Ramai D, Enofe I, Deliwala SS, et al. Early (<4 weeks) versus standard (≥4 weeks) endoscopic drainage of pancreatic walled-off fluid collections: a systematic review and meta-analysis. Gastrointest Endosc. 2023;97:415-21.e5.
Baroud S, Chandrasekhara V, Storm AC, et al. Novel classification system for walled-off necrosis: a step toward standardized nomenclature and risk-stratification framework. Gastrointest Endosc. 2023;97:300–8.
Author information
Authors and Affiliations
Contributions
JS: concept of study, data acquisition, drafting manuscript, critically revising the manuscript. AKS, VJ, AJ: interpretation of data, drafting the manuscript, critically revising the manuscript. TSD: data acquisition, interpretation of data, critically revising the manuscript. YRS, PG, HS: data acquisition, critically revising the manuscript. VS, UD: interpretation of data, critically revising the manuscript. Final approval of manuscript: all authors.
Corresponding author
Ethics declarations
Conflict of interest
JS, AKS, VJ, AJ, TSD, YRS, PG, HS, VS and UD declare no competing interests.
Ethical approval
Taken from Institute Ethics Committee. Helsinki guidelines and Indian Council for Medical Research (ICMR) guidelines were followed.
Consent to participate
Not applicable.
Disclaimer
The authors are solely responsible for the data and the contents of the paper. In no way, the Honorary Editor-in-Chief, Editorial Board Members, the Indian Society of Gastroenterology or the printer/publishers are responsible for the results/findings and content of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Shah, J., Singh, A.K., Jearth, V. et al. Endoscopic ultrasound–guided drainage of early pancreatic necrotic collection: Single-center retrospective study. Indian J Gastroenterol (2023). https://doi.org/10.1007/s12664-023-01478-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12664-023-01478-x