
Abstract
Purpose
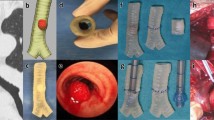
Anatomically correct patient-specific models made from medical imaging can be printed on a three-dimensional (3D) printer or turned into a virtual reality (VR) program. Until recently, use in anesthesia has been limited. In 2019, the anesthesia department at Tel Aviv Medical Center launched a 3D program with the aim of using 3D modelling to assist in preoperative anesthesia planning.
Methods
A retrospective review of all relevant patients between July 2019 and June 2021 referred for preoperative airway planning with 3D modelling. Patient files were reviewed for correlation between the model-based airway plan and the actual airway plan, the type of model used, and any anesthetic complications related to airway management.
Results
Twenty patients were referred for 3D modelling. Of these, 15 models were printed, including 12 children requiring one lung ventilation. Five patients had VR reconstructions, including three with mediastinal masses. One patient had both a 3D-printed model and a VR reconstruction. There were two cases (10%) where the model plan did not correlate with the final airway plan and one case where a model could not be created because of poor underlying imaging. For the remaining 17 cases, the plan devised on the model matched the final airway plan. There were no anesthetic complications.
Conclusions
Three-dimensional modelling and subsequent printing or VR reconstruction are feasible in clinical anesthesia. Its routine use for patients with challenging airway anatomy correlated well with the final clinical outcome in most cases. High-quality imaging is essential.
Résumé
Objectif
Des modèles anatomiquement corrects spécifiques à un·e patient·e réalisés à partir de l’imagerie médicale peuvent être imprimés sur une imprimante tridimensionnelle (3D) ou transformés en programme de réalité virtuelle (RV). Jusqu’à récemment, l’utilisation de cette modalité était limitée en anesthésie. En 2019, le service d’anesthésie du centre médical de Tel Aviv a lancé un programme 3D dans le but d’utiliser la modélisation 3D pour faciliter la planification préopératoire de l’anesthésie.
Méthode
Nous avons réalisé un examen rétrospectif de toute la patientèle concernée référée pour une planification préopératoire des voies aériennes avec modélisation 3D entre juillet 2019 et juin 2021. Les dossiers des patient·es ont été examinés pour déterminer la corrélation entre le plan de prise en charge des voies aériennes fondé sur le modèle et le plan fondé sur les voies aériennes réelles, le type de modèle utilisé et toute complication anesthésique liée à la prise en charge des voies aériennes.
Résultats
Vingt patient·es ont été référé·es pour la modélisation 3D. À partir de cette cohorte, 15 modèles ont été imprimés, dont 12 pour des enfants nécessitant une ventilation pulmonaire. Cinq patient·es ont bénéficié de reconstructions en RV, dont trois avec des masses médiastinales. Un modèle imprimé en 3D et une reconstruction en RV ont été créés pour une personne. Il y a eu deux cas (10 %) où le plan modèle n’était pas corrélé avec le plan des voies aériennes final et un cas où il n’a pas été possible de créer un modèle en raison d’une mauvaise imagerie sous-jacente. Pour les 17 cas restants, le plan conçu sur le modèle correspondait au plan final de prise en charge des voies aériennes. Il n’y a pas eu de complications anesthésiques.
Conclusion
La modélisation tridimensionnelle et l’impression ultérieure ou la reconstruction en RV sont réalisables en anesthésie clinique. Leur utilisation systématique pour les patient·es présentant une anatomie difficile au niveau des voies aériennes était bien corrélée avec le résultat clinique final dans la plupart des cas. Une imagerie de haute qualité est essentielle.


Similar content being viewed by others


References
Martinez-Marquez D, Mirnajafizadeh A, Carty CP, Stewart RA. Application of quality by design for 3D printed bone prostheses and scaffolds. PLoS One 2018; 13: e0195291. https://doi.org/10.1371/journal.pone.0195291
Jandali D, Barrera JE. Recent advances in orthognathic surgery. Curr Opin Otolaryngol Head Neck Surg 2020; 28: 246–50. https://doi.org/10.1097/MOO.000000000000063
Park S, Ahn J, Yoon SU, et al. Prediction of endotracheal tube size using a printed three-dimensional airway model in pediatric patients with congenital heart disease: a prospective, single-center, single-group study. Korean J Anesthesiol 2021; 74: 333–41. https://doi.org/10.4097/KJA.21114
Shaylor R, Verenkin V, Golden E, Matot I. The use of three-dimensional printing and virtual reality to develop a personalised airway plan in a 7.5-year-old child: a case report. Eur J Anaesthesiol 2020; 37: 512–5. https://doi.org/10.1097/EJA.0000000000001184
Chepelev L, Wake N, Ryan J, et al. Radiological Society of North America (RSNA) 3D printing Special Interest Group (SIG): guidelines for medical 3D printing and appropriateness for clinical scenarios. 3D Print Med 2018; 4: 11. https://doi.org/10.1186/s41205-018-0030-y
Author contributions
Ruth Shaylor, Eran Golden, Vladimir Verenkin, Idit Matot, and Barak Cohen contributed to all aspects of this manuscript, including study conception and design; acquisition, analysis, and interpretation of data; and drafting the article. Solomon Dadia, Michael Peer, and Marina Kolodii contributed to the acquisition of data.
Acknowledgments
With thanks to Ronny Gabbi and Tal Katsir for segmenting some of the 3D models.
Disclosures
The authors have no conflict of interest to report.
Funding statement
This study did not receive any external funding.
Prior conference presentations
Parts of this work was presented at Euroanaesthesia 2021 (virtual congress; 17–19 December 2021).
Editorial responsibility
This submission was handled by Dr. Philip M. Jones, Deputy Editor-in-Chief, Canadian Journal of Anesthesia/Journal canadien d’anesthésie.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 eVideo 1 An example of using a 3D-printed model to select airway equipment (MP4 6780 KB)
Supplementary file2 eVideo 2 An example of a virtual reality reconstruction in a case of a large anterior mediastinal mass (MP4 193841 KB)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Shaylor, R., Golden, E., Verenkin, V. et al. Virtual reality and 3D printing in clinical anesthesia: a case series of two years’ experience in a single tertiary medical centre. Can J Anesth/J Can Anesth 70, 1433–1440 (2023). https://doi.org/10.1007/s12630-023-02530-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-023-02530-2