
Abstract
Purpose
A stylet is usually necessary when using the GlideScope® videolaryngoscope for orotracheal intubation. A special stylet, the GlideRite® Rigid Stylet (GRS), was designed for this purpose. A previous trial involving experienced operators showed that the GRS offered no performance improvement vs a standard malleable stylet (SMS). In our trial, we compared the performance of the GRS with that of the SMS in terms of time to intubation and ease of intubation when used by novice GlideScope® operators.
Methods
Sixty patients with normal-appearing airways requiring orotracheal intubation for elective surgery were randomly allocated to be intubated by novice operators with the GlideScope®, using either the GRS or the SMS. Time to intubation was assessed by a blinded observer, and the operators were blinded until just prior to tracheal intubation. Ease of intubation was assessed by a five-point ordinal scale (from 1- easy to 5 -difficult). Intubation attempts/failures, glottic grades, and usage of external laryngeal manipulation were recorded.
Results
There were no significant differences between the GRS and the SMS in terms of the median time to intubation (60 sec, interquartile range [IQR] 48-75 vs 61 sec, IQR 49-75, respectively; P = 0.94) and the ease of intubation (GRS median score: 1.5, IQR 1-2 vs SMS median score: 1, IQR 1-2; P = 0.94). There were no other significant differences between groups.
Conclusion
The GRS and the SMS have similar performance characteristics when used by novice operators for GlideScope®-assisted orotracheal intubation. (Registered at ClinicalTrials.gov: NCT00884754).
Résumé
Objectif
Un mandrin est en général nécessaire lorsqu’on utilise le vidéolaryngoscope GlideScope® pour réaliser une intubation orotrachéale. À cette fin, un mandrin spécial a été conçu, le mandrin rigide GlideRite® (GRS). Une étude précédente portant sur des opérateurs d’expérience a démontré que le GRS n’améliorait pas la performance par rapport à un mandrin flexible standard (MFS). Dans notre étude, nous avons comparé la performance du GRS à celle du MFS en termes de temps d’intubation et de facilité d’intubation lorsqu’ils étaient utilisés par des personnes n’ayant jamais utilisé le GlideScope®.
Méthode
Soixante patients présentant des voies aériennes d’apparence normale et devant subir une intubation orotrachéale pour une chirurgie non urgente ont été recrutés. Des opérateurs sans expérience ont aléatoirement répartis les patients afin qu’ils soient intubés avec le GlideScope® à l’aide du GRS ou d’un MFS. Le temps d’intubation a été évalué par un observateur en aveugle, et les opérateurs ne savaient pas quelle méthode allait être utilisée jusqu’au moment de l’intubation trachéale. La facilité d’intubation a été évaluée à l’aide d’une échelle ordinale à cinq points (de 1 – facile à 5 – difficile). Les tentatives/échecs d’intubation, les grades d’intubation et le recours à une manipulation laryngée externe ont été notés.
Résultats
Aucune différence significative n’a été observée entre le GRS et le MFS en termes de temps médian d’intubation (60 sec, écart interquartile [EIQ] 48-75 vs. 61 sec, EIQ 49-75, respectivement; P = 0,94) et de facilité d’intubation (score médian pour le GRS : 1,5, EIQ 1-2 vs. score médian pour le MFS : 1, EIQ 1-2; P = 0,94). Aucune autre différence significative n’a été observée entre les groupes.
Conclusion
Les caractéristiques de performance du GRS et du MFS sont semblables lorsqu’ils sont utilisés par des opérateurs novices pour réaliser une intubation orotrachéale assistée avec GlideScope®. (Enregistré à ClinicalTrials.gov : NCT00884754).
Similar content being viewed by others


The GlideScope® videolaryngoscope (GVL) (Verathon® Medical Inc., Bothell, WA, USA) has an established role in routine orotracheal and nasotracheal intubation1-3 Although it frequently provides a good glottic view,1,4 advancing the endotracheal tube (ETT) through the vocal cords can sometimes be difficult5 and trauma is possible.6,7 Due to the curvature of the GVL blade, a stylet is usually used to position the ETT tip at the glottic opening,5 although a stylet is not required in all cases.8 In order to place it optimally into the trachea, various authors have recommended different curvatures of the ETT/stylet, including matching the blade’s 60° angle,1 Footnote 1 configuring the ETT with a 90° bend,4,5 or using a J-shaped ETT.9
The GlideScope® manufacturer has designed a reusable stylet specifically for use with the GVL. This GlideRite® Rigid Stylet (GRS) is substantially more rigid than a standard malleable stylet (SMS). Its curvature approaches 90° with a radius of curvature of approximately 6 cm (Fig. 1).A

GlideRite® Rigid Stylet, shown individually and inside an endotracheal tube
A randomized clinical trial investigating the efficacy of the GRS demonstrated that the GRS offered no significant advantage over the standard malleable stylet for orotracheal intubation by experienced operators.10 However, any potential intubation advantage of the GRS due to its unique geometry and stiffness may have been all or partially negated by the experienced operators’ increased knowledge and skill in using the SMS or by their ability to compensate for a disadvantage associated with the SMS. In this case, the best way to expose the putative advantage of using the GRS for intubation with the GlideScope® would be for novice operators to use the GRS. Novice operators would have similar inexperience with both devices and a limited ability to compensate for any potential disadvantages associated with using a malleable stylet. Therefore, in the context of GlideScope®-assisted orotracheal intubation by novice operators, a randomized clinical trial was devised to test whether there was any significant advantage to using the GRS over using the SMS. The null hypothesis was that there would be no difference between the stylets in terms of time to intubation.
Methods
This single centre balanced parallel-group randomized clinical trial took place at University Hospital in London, Ontario, Canada from March to November 2009, and it involved patients having surgery in most surgical disciplines. The trial was registered at ClinicalTrials.gov (NCT00884754) before enrolment of the first patient in the trial. After obtaining local research ethics board approval, patients aged 18 yr and older and scheduled for elective surgery requiring orotracheal intubation were invited to participate. Exclusion criteria included a known or suspected difficult airway (determined by the attending anesthesiologist on physical examination), requirement for rapid sequence induction, or a contraindication to GVL use (determined by the attending anesthesiologist). Anesthesiology trainees were eligible as operators if they had performed ten or fewer GVL-assisted intubations. Written informed consent was obtained from all patients and operators.
The null hypothesis was that there would be no difference between the stylets in terms of time to intubation. The GRS was used according to the manufacturer’s instructions (Fig. 1), and tracheal intubation for the control group was performed according to the standard local practice. First, an ETT was loaded with forward camber4 onto a malleable stylet, 14 French Rusch Flexi-Slip™ (Teleflex Medical, Bannockburn, IL, USA), and a 90° angle was formed 8 cm from the distal end of the ETT; there was no other ETT angulation (Fig. 2).

Malleable Rusch 14 French stylet inserted into an endotracheal tube. The 90º bend was formed 8 cm from the tip
Patient demographics and airway assessment11 were recorded preoperatively, and the ETT size was chosen prior to patient randomization. As each patient entered the operating room, group allocation was carried out by opening a sealed opaque envelope containing a computer-generated random code specifying the group assignment (the randomization sequence was generated using the ralloc program in Stata 11.0 for Mac OS X [StataCorp LP, College Station, TX, USA] with two blocks of 30 patients each created to ensure an equal number of patients randomly assigned to each group). One of the study investigators prepared an ETT with each of the stylets according to the study protocol. This investigator concealed the assigned ETT with a towel and concealed the remaining ETT in another towel to be used if the operator was unsuccessful with the allocated stylet. This investigator then had no further involvement with that patient’s clinical care or outcome assessment. To avoid any potential bias during induction, GVL laryngoscopy, or glottic view scoring, each ETT was concealed so that the GVL operator remained blinded until after the GVL laryngoscopy had been completed.4
Induction and maintenance of anesthesia were not standardized, but pre-oxygenation was mandated to an end-tidal oxygen concentration of ≥ 80%, and all patients were paralyzed with rocuronium. After induction, the patient’s lungs were ventilated with a volatile anesthetic agent in 100% oxygen until the operator deemed it appropriate to begin intubation. A minimum delay of 90 sec was utilized for onset of paralysis.
The operator performed laryngoscopy with the GVL (size five) and graded the glottic view using the classification described by Cormack & Lehane.12 The ETT was then revealed, unblinding the operator, and the patient’s trachea was intubated with the ETT and assigned stylet. If necessary, operators were permitted to use external laryngeal manipulation in order to improve the glottic view or to facilitate intubation. If the operator removed the GVL blade or ETT from the patient’s mouth, this was counted as an additional attempt at intubation.
The primary outcome was the time to intubation as measured by a blinded observer. The time to intubation was defined from the moment the GVL blade first passed the patient’s teeth to the moment end-tidal CO2 of at least 30 mmHg was present on the anesthesia monitor. As soon as the timer started, the blinded observer turned so that only the anesthesia monitor was visible. At no point did the observer see the allocated stylet. If the novice operator took > 150 sec or more than two tries to perform the intubation, it was deemed a failure, and the airway was subsequently managed using any technique deemed appropriate by the attending anesthesiologist (the patients were analyzed in the group to which they were randomized regardless of the stylet or modality used for successful intubation). Failed intubations were included in the analysis (recorded as a time to intubation of 150 sec). Ventilation between attempts was permitted if necessary. Pre-specified secondary outcomes for each group included ease of intubation (scored by the operator immediately after laryngoscopy on a five-point ordinal scale), number of attempts, glottic grade, and use of external laryngeal manipulation. The time to intubation was not divulged to the operator until after the data collection sheet had been completed.
The sample size calculation was based on parametric analysis, although non-parametric analysis was planned for the outcomes in the study.13 A between-group difference of 15 sec in time to intubation was considered clinically significant. The standard deviation of the time to intubation —estimated to be approximately 20 sec— was based on a previous study in a group of both experienced and inexperienced operators.4 Standard Type I and Type II error rates were used (α = 0.05, β = 0.20). The calculated sample size was 28 patients per group, but a total sample size of 60 patients was selected in order to maintain statistical power in case of patient drop out or missing data.
Statistical analysis
Due to an anticipated right-skewed distribution, both time to intubation and ease of intubation were assessed using a non-parametric method (the Mann-Whitney test). Categorical data were analyzed with Pearson’s Chi square test. Data are shown as median and IQR unless otherwise noted. No corrections for multiple comparisons were made.14 Data were analyzed using Stata version 11.0 for Mac OS X. Results were considered statistically significant when P < 0.05.
Results
A total of 64 patients were screened. Three patients met the trial’s inclusion criteria but declined participation, and one patient did not meet the trial’s inclusion criteria (required rapid sequence induction). Sixty patients met the inclusion criteria, gave informed consent, were randomized, and contributed data to the primary outcome. No patients were lost or excluded after randomization. Baseline demographics were similar between groups, and similar numbers of unique trainees were operators in both groups (Table 1).
Operators failed to intubate the tracheas of four patients (two in each group) within 150 sec of inserting the GVL into the patient’s mouth. All of these failures were attributed (by the attending anesthesiologist) to the trainee’s lack of experience in visualizing glottic structures or passage of the ETT. The attending anesthesiologist easily intubated the tracheas of the four patients on the first attempt.
The median time to intubation was not significantly different between the two groups (Table 2). A Kaplan-Meier plot was constructed to illustrate the success of intubation as a function of time (Fig. 3). The ease of intubation was also similar between groups (Table 2 and Fig. 4).

Kaplan-Meier plot demonstrating the proportion of patients successfully intubated vs time. The four patients (two in each group) who were assigned times of 150 sec (see Methods) are not included in the figure; therefore, the proportion of patients successfully intubated in each group within 150 sec was 28/30 (93%). Groups were compared using the Mann-Whitney test

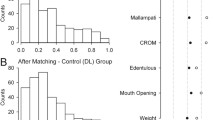
Ease of intubation by operators as measured on a five-point scale, separated by group. The scale on the data collection form was marked “Easy” (1) and “Difficult” (5). Groups were compared using the Mann-Whitney test
Glottic exposure was good in both groups, and there was no difference between groups in the number of attempts at intubation, failed intubations, usage of external laryngeal manipulation, or the first-attempt success rate (Table 2). No trauma occurred during any of the intubations in this trial.
Since non-parametric methods can lack statistical power, exploratory analysis was performed post-hoc to compare time to intubation between groups using a parametric method (Student’s t test). This analysis also showed no significant differences between stylet groups (Table 2). The difference in the mean time to intubation between the GRS and the malleable stylet was 0.4 sec in favour of the malleable stylet (95% confidence interval of the difference: -15.1 to 15.8 sec; P = 0.96).
Discussion
There was no advantage to using the GRS over the standard malleable stylet in this group of patients who underwent orotracheal intubation by novice operators with the GlideScope® videolaryngoscope. Specifically, both groups had similar times to intubation and ease of intubation. The Kaplan-Meier plot (Fig. 3) showing the proportion of patients whose tracheas were intubated successfully as time progressed demonstrates overlap at many time points, thus indicating no significant difference between stylets.
It is important to test new anesthesiology-related devices adequately in the clinical arena before widespread adoption. Although the design of a new device may appear sensible and possibly superior to a currently used device, it is not enough simply to have faith that the new device should work better than an older device. The new device should be tested, ideally under the rigors of a randomized clinical trial, to eliminate bias from known and unknown confounders. New devices are often more expensive than the devices they seek to replace, but the additional financial investment is not always associated with an improvement in clinical care. In this case, the GRS is a reusable device, which means it is potentially cost saving. However, no formal economic analysis was carried out in this trial, and the benefits of reusable devices (potential for cost saving) must be weighed against their disadvantages (potential for disease transmission, costs associated with inadvertent disposal of reusable devices, delay in use if being cleaned, and a potential decrease in reliability). It is speculative as to whether the GRS is potentially less traumatic to the pharynx, as palatal injuries have occurred with both the GRS7 and the malleable stylet.6
This trial has several limitations. Operators were aware they were participating in a clinical trial and that the tracheal intubation was being timed. This fact alone could have led to better clinical performance. However, it is expected that any improvement would have been equally distributed between the groups, thus minimizing the impact of this effect. Also, it was not possible to blind operators to the stylet they were using. However, all personnel in this study were blinded until the last possible moment in order to minimize any systematic bias, and the assessor of the primary outcome of the trial (the timer) was fully blinded. In addition, all operators were novices, and it is unlikely that they would possess a pre-existing bias for or against a certain stylet at such an early stage in their training. Since this trial was conducted in patients with normal-appearing airways, the results may not be applicable to patients with abnormal airways. Finally, it is possible that one of the two stylets was actually superior to the other, and this trial could not discern this superiority because of inadequate power (a Type II error). However, in this trial, the clinical importance of a difference too small to be detected is doubtful and would be debatable even if the difference were statistically significant.
In conclusion, the standard malleable stylet demonstrates similar performance to the GlideRite® Rigid Stylet when used by novice operators in conjunction with the GlideScope® videolaryngoscope to perform orotracheal intubation in patients with normal airways. Both stylets are suitable for orotracheal intubation by novice operators.
Notes
Verathon Medical Inc. GlideScope Video Intubation System - Operator and Service Manual, 2003.
References
Cooper RM, Pacey JA, Bishop MJ, McCluskey SA. Early clinical experience with a new videolaryngoscope (GlideScope) in 728 patients. Can J Anesth 2005; 52: 191-8.
Sun DA, Warriner CB, Parsons DG, Klein R, Umedaly HS, Moult M. The GlideScope(R) Video Laryngoscope: randomized clinical trial in 200 patients. Br J Anaesth 2005; 94: 381-4.
Jones PM, Armstrong KP, Armstrong PM, et al. A comparison of GlideScope videolaryngoscopy to direct laryngoscopy for nasotracheal intubation. Anesth Analg 2008; 107: 144-8.
Jones PM, Turkstra TP, Armstrong KP, et al. Effect of stylet angulation and endotracheal tube camber on time to intubation with the GlideScope(R). Can J Anesth 2007; 54: 21-7.
Doyle DJ. The GlideScope video laryngoscope. Anaesthesia 2005; 60: 414-5.
Cooper RM. Complications associated with the use of the GlideScope videolaryngoscope. Can J Anesth 2007; 54: 54-7.
Malik AM, Frogel JK. Anterior tonsillar pillar perforation during GlideScope video laryngoscopy. Anesth Analg 2007; 104: 1610-1.
van Zundert A, Maassen R, Lee R, et al. A Macintosh laryngoscope blade for videolaryngoscopy reduces stylet use in patients with normal airways. Anesth Analg 2009; 109: 825-31.
Bader SO, Heitz JW, Audu PB. Tracheal intubation with the GlideScope(R) videolaryngoscope, using a “J” shaped endotracheal tube. Can J Anesth 2006; 53: 634-5.
Turkstra TP, Harle CC, Armstrong KP, et al. The GlideScope-specific rigid stylet and standard malleable stylet are equally effective for GlideScope use. Can J Anesth 2007; 54: 891-6.
Mallampati SR, Gatt SP, Gugino LD, et al. A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J 1985; 32: 429-34.
Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics. Anaesthesia 1984; 39: 1105-11.
Lehmann EL, D’Abrera HJ. Nonparametrics: Statistical Methods Based on Ranks. San Francisco: Holden-Day; 1975 .
Perneger TV. What’s wrong with Bonferroni adjustments. BMJ 1998; 316: 1236-8.
Acknowledgements
We gratefully acknowledge the assistance of the respiratory therapists with data collection and the cooperation of the surgeons whose patients were involved in this trial.
Financial support
This study was funded by internal funding from the Department of Anesthesiology & Perioperative Medicine at the University of Western Ontario. Verathon® supplied the GlideRite® stylets but had no role in the trial’s conception, design, execution, analysis, or manuscript preparation.
Competing interests
Dr. Jones has received an honorarium for writing a chapter in a booklet about videolaryngoscopy using the GlideScope®.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jones, P.M., Loh, F.L.C., Youssef, H.N. et al. A randomized comparison of the GlideRite® Rigid Stylet to a malleable stylet for orotracheal intubation by novices using the GlideScope® . Can J Anesth/J Can Anesth 58, 256–261 (2011). https://doi.org/10.1007/s12630-010-9440-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-010-9440-z