
Abstract
Background
It is acknowledged that expansion of the remote normal region of the left ventricle causes remodeling after myocardial infarction (MI). However, the characteristics of that region have not been fully elucidated.
Methods
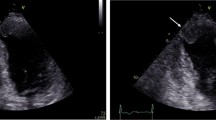
We studied 13 patients with atypical chest pain (controls) and 15 patients with a prior anterior MI who underwent cardiac catheterization. With Doppler strain imaging, we measured the peak radial myocardial systolic strain and peak radial early diastolic strain rate at the posterior wall of the left ventricle. None of the patients with atypical chest pain exhibited significant stenosis of the three major coronary arteries or left ventricular (LV) wall motion abnormality in cardiac catheterization. The patients with a prior anterior MI had single anterior descending artery disease without wall motion abnormality in the LV inferoposterior wall. LV ejection fraction and the LV relaxation time constant were also measured.
Results
The LV ejection fraction was significantly smaller in patients with a prior MI compared to controls. The peak radial systolic strain in the LV posterior wall was not significantly different between the patients with a prior MI and controls (125 ± 49 vs. 122 ± 29%). In contrast, the peak radial early diastolic strain rate in the same area was significantly lower in the patients with a prior MI than in controls (−7.4 ± 2.7 vs. −13.2 ± 4.0 s−1, p < 0.001). Peak early diastolic radial strain rate was significantly correlated with the LV relaxation time constant in all patients (r = 0.69, p < 0.001).
Conclusion
LV remodeling after an MI impairs local early diastolic myocardial function in the remote normal region and it is related to global LV diastolic dysfunction.



Similar content being viewed by others


References
Pfeffer MA, Braunwald E. Ventricular remodeling after myocardial infarction experimental observations and clinical implications. Circulation. 1990;81:1161–72.
Pfeffer JM, Pfeffer MA, Fletcher PJ, Braunwald E. Progressive ventricular remodeling in rat with myocardial infarction. Am J Physiol. 1991;260:H1406–14.
Sutton MG, Sharpe N. Left ventricular remodeling after myocardial infarction: pathophysiology and therapy. Circulation. 2000;101:2981–8.
Ohte N, Narita H, Iida A, Wakami K, Asada K, Fukuta H, et al. Impaired myocardial oxidative metabolism in the remote normal region in patients in the chronic phase of myocardial infarction and left ventricular remodeling. J Nucl Cardiol. 2009;16:73–81.
Costa KD, Takayama Y, McCulloch AD, Covell JW. Laminar fiber architecture and three-dimensional systolic mechanics in canine ventricular myocardium. Am J Physiol Heart Circ Physiol. 1999;276:H595–607.
D’hooge J, Heimdal A, Jamal F, Kukulski T, Bijnens B, Rademakers F, et al. Regional train and strain rate measurements by cardiac ultrasound: principles, implementation and limitations. Eur J Echocardiogr. 2000;1:154–70.
Ohte N, Narita H, Hashimoto T, Akita S, Kurokawa K, Fujinami T. Evaluation of left ventricular early diastolic performance by color tissue Doppler imaging of the mitral annulus. Am J Cardiol. 1998;82:1414–7.
Goto T, Ohte N, Miyabe H, Sakata S, Asada K, Mukai S, et al. Usefulness of plasma brain-type natriuretic peptide level to differentiate left ventricular diastolic dysfunction from preserved diastolic function in patients with systolic dysfunction. Am J Cardiol. 2005;95:1383–5.
Yoshida T, Ohte N, Narita H, Sakata S, Wakami K, Asada K, et al. Lack of inertia force of late systolic aortic flow is a cause of left ventricular isolated diastolic dysfunction in patients with coronary artery disease. J Am Coll Cardiol. 2006;48:983–91.
Weiss JL, Frederiksen JW, Weisfeldt ML. Hemodynamic determinants of the time-course of fall in canine left ventricular pressure. J Clin Investig. 1976;58:751–60.
Chapman CB, Baker O, Reynolds J, Bonte FJ. Use of biplane cinefluorography for measurement of ventricle volume. Circulation. 1958;18:1105–17.
Holtz J, Restorff WV, Bard P, Bassenge E. Transmural distribution of myocardial blood flow and of coronary reserve in canine left ventricular hypertrophy. Basic Res Cardiol. 1977;72:286–92.
Waller C, Hiller KH, Kahler E, Hu K, Nahrendorf M, Voll S, et al. Serial magnetic resonance imaging of microvascular remodeling in the infarcted rat heart. Circulation. 2001;103:1564–9.
Schwartzkopff B, Motz W, Frenzel H, Vogt M, Knauer S, Strauer B. Structural and functional alterations of the intramyocardial coronary arterioles in patients with arterial hypertension. Circulation. 1993;88:993–1003.
Tanaka M, Fujiwara H, Onodera T. Quantitative analysis of narrowings of intramyocardial small arteries in normal hearts, hypertensive hearts, and hearts with hypertrophic cardiomyopathy. Circulation. 1987;75:1130–9.
Gimelli A, Schneider-Eicke J, Neglia D, Sambuceti G, Giorgetti A, Bigalli G, et al. Homogeneously reduced versus regionally impaired myocardial blood flow in hypertensive patients: two different patterns of myocardial perfusion associated with degree of hypertrophy. J Am Coll Cardiol. 1998;31:366–73.
Uren NG, Crake T, Lefroy DC, de Silva R, Davies GJ, Maseri A. Reduced coronary vasodilator function in infarcted and normal myocardium after myocardial infarction. N Engl J Med. 1994;331:222–7.
Geshi T, Nakano A, Uzui H, Okazawa H, Yonekura Y, Ueda T, et al. Relationship between impaired microvascular function in the non-infarct-related area and left-ventricular remodeling in patients with myocardial infarction. Int J Cardiol. 2008;126:366–73.
Goto T, Ohte N, Miyabe H, Mukai S, Sakata S, Hayano J, et al. Tl-201 washout rate in remote normal regions in patients with prior myocardial infarction and left ventricular remodeling. J Nucl Cardiol. 2005;12:179–85.
Ohte N, Kurokawa K, Iida A, Narita H, Akita S, Yajima K, et al. Myocardial oxidative metabolism in remote normal regions in the left ventricles with remodeling after myocardial infarction: effect of beta-adrenoceptor blockers. J Nucl Med. 2002;43:780–5.
Vinereanu D, Ionescu A, Fraser AG. Assessment of left ventricular long axis contraction can detect early myocardial dysfunction in asymptomatic patients with severe aortic regurgitation. Heart. 2001;85:30–6.
Vinereanu D, Nicolaides E, Tweddel AC, Mädler CF, Holst B, Boden LE, et al. Subclinical left ventricular dysfunction in asymptomatic patients with type 2 diabetes mellitus, related to serum lipids and glycated haemoglobin. Clin Sci. 2003;105:591–9.
Ohte N, Narita H, Miyabe H, Takada N, Goto T, Mizuno H, et al. Evaluation of whole left ventricular systolic performance and local myocardial systolic function in patients with prior myocardial infarction using global long-axis myocardial strain. Am J Cardiol. 2004;94:929–32.
Nesto RW, Kowalchuk GJ. The ischemic cascade: temporal sequence of hemodynamic, electrocardiographic and symptomatic expressions of ischemia. Am J Cardiol. 1987;59:23C–30C.
Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–9.
Australia-New Zealand Heart Failure Research Collaborative Group. Effects of carvedilol, a vasodilator-beta-blocker, in patients with congestive heart failure due to ischemic heart disease. Circulation. 1995;92:212–8.
Kuznetsova T, Herbots L, Richart T, D’hooge J, Thijs L, Fagard RH, et al. Left ventricular strain and strain rate in a general population. Eur Heart J. 2008;29:2014–23.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kobayakawa, H., Ohte, N., Wakami, K. et al. Left ventricular remodeling after myocardial infarction impairs early diastolic, but not systolic, function in the radial direction in the remote normal region. J Echocardiogr 8, 112–117 (2010). https://doi.org/10.1007/s12574-010-0057-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12574-010-0057-6