
Abstract
Background
The risk of developing aggressive phenotype non-Hodgkin’s lymphomas is high among HIV infected individuals and is associated with worse prognosis than among non-HIV infected ones. Effective antiretroviral therapy has more recently been reported to greatly improve outcome among these patients. A retrospective review of treatment outcome for aggressive and highly aggressive phenotype non-Hodgkin’s lymphoma patients was carried out.
The objective was to compare outcome of treatment for poor prognosis subtypes of non-Hodgkin’s lymphomas in relation to HIV-serostatus. The setting was Hurlingham Oncology clinic, a private oncology clinic in Nairobi, Kenya. The main study endpoints were complete remission rate and overall survival.
Results
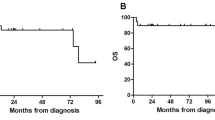
Thirty-two patients (42.7%) were HIV-positive, 32 (42.7%) were HIV-negative and 11 (14.7%) had HIV serostatus undetermined. Seven (21.9%) of HIV positive patients achieved complete remission compared with 24 (75%) of HIV negative ones. This difference was highly significant (P < 0.0001). Five (15.6%) of HIV-positive patients died during first-line treatment compared with none of the HIV-negative counterparts. The difference again was highly significant (P < 0.0001). The median survival time was 19 months among HIV-negative patients and 6 months among positive cases.
Conclusion
Complete remission rate among HIV-negative patients in this series was the same as reported from well established centres, but the rate among HIV-positive patients was lower than expected. Patients with HIV infection were more likely to die from toxicity during induction and had inferior survival compared with HIV-negative cases.
Résumé
Contexte
Le risque de développer un lymphome non-hodgkinien au phénotype agressif est élevé chez les patients séropositifs, et est associé à un pronostic plus grave que pour les patients séronégatifs. La thérapie antirétrovirale a été présentée récemment comme étant efficace pour améliorer significativement les résultats chez ces patients. Une analyse rétrospective des résultats du traitement pour le lymphome non-hodgkinien à phénotype agressif et très agressif a été réalisée.
L’objectif était d’évaluer les résultats du traitement pour les sous-types de lymphome non-hodgkinien à pronostic pauvre associé au sérostatut du VIH. L’étude a été menée à la clinique d’oncologie de Hurlingham, un établissement privé situé à Nairobi, au Kenya. Les principaux critères d’évaluation de l’étude étaient un taux de rémission complète et une survie généralisée.
Résultats
Trente-deux patients (42,7 %) étaient séropositifs, 32 (42,7 %) étaient séronégatifs, et 11 (14,7 %) n’avaient pas de sérostatut déterminé. On a constaté une rémission complète chez sept patients séropositifs (21,9 %) et chez 24 patients séronégatifs (75 %). Cette différence était très significative (P < 0,0001). Cinq des patients séropositifs (15,6 %) sont décédés au cours du traitement de première ligne, tandis qu’aucun n’a succombé parmi les patients séronégatifs. Là encore, la différence était très significative (P < 0,0001). La durée de survie moyenne constatée était de 19 mois chez les patients séronégatifs, et de 6 mois chez les patients séropositifs.
Conclusion
Le taux de rémission complète des patients séronégatifs de cette étude était identique à celui communiqué par des centres de soins bien établis, mais le taux de rémission chez les patients séropositifs était plus faible que prévu. Le risque de mourir dû à la toxicité pendant le début du traitement était plus élevé chez les patients séropositifs, et ces derniers présentaient un taux de survie plus faible que les patients séronégatifs.
Similar content being viewed by others

References
Telenti A, Egger M (1999) Risk of HIV related Kaposi’s sarcoma and non-Hodgkin’s lymphoma with potent antiretroviral therapy: prospective cohort study. Br Med J 319:23–24
Thirlwell C, Sarker D, Stebbing J, et al (2003) Acquired immunodeficiency syndrome-related lymphoma in the era of highly active antiretroviral therapy. Clin Lymphoma 4:86–92
Knowles DM (2003) Etiology and pathogenesis of AIDS-associated non-Hodgkin’s lymphoma. Hematol Oncol Clin N Aam 17:785–820
Dal Maaso L, Francheschi S (2003) Epidemiology of non-Hodgkin’s lymphomas and other haemolymphopoietic neoplasms in people with AIDS. Lancet Oncol 4:110–119
Ansari MQ, Dawson DB, Nador R, et al (1996) Primary body cavity-based AIDS-related lymphomas. Am J Clin Path 105: 221–229
Boulanger E, Gerard L, Gabarre J, et al (2005) Prognostic factors and outcome of human herpes virus 8-associated primary effusion lymphoma in patients with AIDS. J Clin Oncol. 23: 4372–4380
Lim ST, Karim R, Nathwani B, et al (2005) AIDS-related Burkitt’s lymphoma versus diffuse large-cell lymphoma in pre-highly active antiretroviral therapy (HAART) and HAART eras: significant differences in survival with standard chemotherapy. J Clin Oncol 19:4430–4438
Gabarre J, Raphael M, Le Page E, et al (2001) Human immunodeficiency virus-related lymphoma: Relation between clinical features and histologic subtypes. Am J Med 111: 704–711
Bower M, Fife K, Sullivan A, et al (1999) Treatment outcome in presumed and confirmed AIDS-related primary cerebral lymphoma. Eur J Cancer 35:601–604
Mathews GV, Bower M, Mandalia S, et al (2000) Changes in aquired immunodeficiency syndrome-related lymphoma since the introduction of highly active anti-retroviral therapy. Blood 96: 2730–2734
Bresson C, Goubar A, Gabarre J, et al (2001) Changes in AID-srelated lymphoma since the era of highly active anti-retroviral therapy. Blood 98:2329–2344
Antinori A, Cingolani A, Albal, et al (2001) Better response to chemotherapy and prolonged survival in AIDS-related lymphomas responding to highly active antiretroviral therapy. AIDS: 1483–14891
Gerard L, Galicier L, Maillord A, et al (2002) Systemic non-Hodgkin’s lymphoma in HIV-infected patients with effective suppression of HIV replication: persistent occurrence but improved survival. J Acquir Immune Defic Syndr 30:478–484
Hoffman C, Wolf E, Fatkenheuer G, el al (2003) Response to highly active antiretroviral therapy strongly predicts outcome in patients with AIDS-related lymphoma. AIDS 17:154–1529
Vaccher E, Spinal M, Talamini R, et al (2003) Improvement of systemic human immunodeficiency virus related non-Hodgkin’s lymphoma outcome in the era of highly active antiretroviral therapy. Clin Infect Dis 37:1556–1564
Straus DJ, Huang J, Testa AM, et al (1998) Prognostic factors in the treatment of human immunodeficiency virus-associated non-Hodgkin’s lymphoma: Analysis of AIDS Clinical Trialists Group protocol 142 — low dose versus standard dose m-BACOD plus granulocyte-macrophage colony-stimulating factor: National Institute of Allergy and Infections Disease. J Clin Oncol 16: 3601–3606
Kaplan LD, Strauss DJ, Testa MA, et al (1997) Low-dose compared with standard-dose m-BACOD chemotherapy in non-Hodgkin’s lymphoma associated with human immunodeficiency virus infection. N. Engl J Med 336:1641–1648
Carbonne PP, Kaplan HS, Muschoff K, et al (1971) Report of the committee on Hodgkin’s disease staging classification. Cancer Res 31:1860–1869
Shipp MR (1993) The International non-Hodgkin’s lymphomas prognostic Factors Project: A predictive model for aggressive non-Hodgkin’s lymphoma. N Engl J Med 329:987–991
McKelvey GM, Gottlieb JA, Wilson HE, et al (1976) Hydroxyldaunorubicin combined chemotherapy in malignant lymphoma. Cancer 1976; 48:1484
Klimo P, Conors JM (1986) MACOP-B chemotherapy for treatment of diffuse large-cell lymphoma. Ann Intern Med 104:757–65
Coiffier B, Haioun C, Ketterer N, et al (2000) Mabthera/rituximab plus CHOP is superior to CHOP alone in elderly patients with diffuse large B-cell lymphoma (DLBCL): Interim results of a randomized GELA trial. Blood 2000 96: 950a (Abstr)
Harris NL, Jaffe ES, Diebold J, et al (1999) World Health Organization (WHO) classifcation of neoplastic disease of the haematopoietic and lymphoid tissues: Report of the Clinical Advisory Committee — Airlie House, Virginia, November 1997. J Clin Oncol: 7835–7849
Harris N, Jaffe E, Stein H, et al (1994) A revised European — American classification of lymphoid neoplasms: A proposal from the International Lymphoma Study Group. Blood 84:1361–1392
Ioachim HL, Dorsett B, Cronin W, et al (1991) Acquired immunodeficiency syndrome-associated lymphomas: Clinical, pathologic, immunologic, and viral characteristics of 111 cases. Hum Pathol 22:659–673
Razvillas B and Anderson J (2001) An overview of oncology clinical trials. Oncology Special Edition 4:11–120
Longo DL, DeVita VT, Duffey PL, et al (1991) Superiority of ProMACE-cytaBOM over ProMACE-MOPP in the treatment of advanced diffuse aggressive lymphoma: Results of a prospective randomized trial. J Clin Oncol 9:25–38
Fisher RI, Miller TP, Dana BN, et al (1887) South West Oncology Group clinical trials for intermediate and high-grade non-Hodgkin’s lymphomas. Semin Hematol 24:21–25
Fisher RI, Gaynor ER, Dahlber S, et al (1993) Comparison of a standard regimen (CHOP) with three intensive chemotherapy regimens for advanced non-Hodgkin’s lymphoma. N Engl J Med 328:1002–1006
Skarin At, Canellos GP, Rosenthal DS, et al (2008) Improved prognosis of diffuse histiocytic and undifferentiated lymphoma by use of high dose methotrexate alternating with standard agents. J Clin Oncol 26:c85–c92
Sparano JA, Wiernik PH, Hu X, et al (1997) Infusional cyclophosphamide, doxorubicin, and etoposide (CDE) for HIV-associated non-Hodgkin’s lymphoma: Long-term follow-up and analysis of prognostic factors. J AIDS Hum Retroviral 14: A38, (Abstr 88)
Carpenter C, Fischl M, Hammer S, et al (1997) Updated recommendations of the International AIDS Panel. JAMA 227: 1962–1969
Vaccher E, Spina M, Di Gennaro G, et al (2001) Concomitant cyclophosphamide, doxorubicin, and prednisone chemotherapy plus highly active antiretroviral therapy in patients with human immunodeficiency virus-related non-Hodgkin’s lymphoma. Cancer 91:155–163
Sparano JA, Lee S, Chen MG, et al (2004) Phase II trial of infusional cyclophosphamide, doxorubicin, and etoposide in patients with HIV-associated non-Hondgkin’s lymphoma: An Eastern Cooperative Oncology Group Trial (E1494). J Clin Oncol 22:1491–1500
Antinori A, Cingolawi, Alba L, et al (2001) Better response to chemotherapy and prolonged survival in AIDS-related lymphomas responding to highly active antiretroviral therapy. AIDS 15: 1483–1491
Levine AM, Tulpule A, Espina B, et al (2004) Liposome-encopsulated doxorubicin in combination with standard agents (cyclophosphamide, vincristine, prednisone) in patients with newly diagnosed AIDS related non-Hodgkin’s lymphoma: Results of therapy and correlates of response. J Clin Oncol 22:2662–2670
Author information
Authors and Affiliations
Corresponding author
Additional information
The abstract of this paper was published in the Journal of Clinical Oncology, 2007 ASCO Annual Meeting Proceedings (Post-Meeting Edition), Vol. 25, No 18S9 June 20 Supplement), 2007:18535
About this article
Cite this article
Anthony Othieno Abinya, N., Wanjiru Kiarie, G., Otieno Abwao, H. et al. Outcome of poor prognostic phenotype non-Hodgkin’s lymphoma treatment in relation to human immunodeficiency virus serostatus. J Afr Cancer 1, 200–206 (2009). https://doi.org/10.1007/s12558-009-0040-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12558-009-0040-1
Keywords
- non-Hodgkin’s lymphoma
- HIV infection Chemotherapy
- Complete remission
- Treatment-related mortality
- Overall survival