
Abstract
Background
Although symptomatic patients with severe aortic stenosis have a high disease burden and guidelines recommend aortic valve replacement, many are treated conservatively. This study describes to what extent quality of life is changed by aortic valve replacement relative to conservative treatment.
Methods
This observational study followed 132 symptomatic patients with severe aortic stenosis who were subjected to an SF-36v2TM Health Survey.
Results
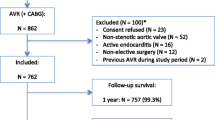
At baseline 84 patients were treated conservatively, 48 were referred for aortic valve replacement. In the conservatively treated group 15 patients died during a mean follow-up of 18 months (Kaplan-Meier survival was 85 % and 72 % at one and 2 years respectively) and 22 patients crossed over to the surgical group. Of the resulting 70 patients in the surgical group 3 patients died during a mean follow-up of 11 months (survival 95 % at 1 year). Physical functioning, vitality and general health improved significantly 1 year after aortic valve replacement. In conservatively treated patients physical quality of life deteriorated over time while general health, vitality and social functioning showed a declining trend. Mental health remained stable in both groups.
Conclusions
Aortic valve replacement improves physical quality of life, general health and vitality in patients with symptomatic severe aortic stenosis. Besides having a low life expectancy, conservatively treated patients experience deterioration of physical quality of life. Health surveys such as the SF-36v2TM can be valuable tools in monitoring the burden of disease for an individual patient and offer additional help in treatment decisions.




Similar content being viewed by others


References
Bonow RO, Carabello BA, Kanu C, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): developed in collaboration with the Society of Cardiovascular Anesthesiologists: endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. Circulation. 2006;114(5):e84–231.
Vahanian A, Baumgartner H, Bax J, et al. Guidelines on the management of valvular heart disease: The Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology. Eur Heart J. 2007;28(2):230–68.
Vahanian A, Alfieri O, Andreotti F, et al. Guidelines on the management of valvular heart disease (version 2012): The Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2012.
Bach DS, Cimino N, Deeb GM. Unoperated patients with severe aortic stenosis. J Am Coll Cardiol. 2007;50(20):2018–9.
Iung B, Cachier A, Baron G, et al. Decision-making in elderly patients with severe aortic stenosis: why are so many denied surgery? Eur Heart J. 2005;26(24):2714–20.
van Geldorp MW, van Gameren M, Kappetein AP, et al. Therapeutic decisions for patients with symptomatic severe aortic stenosis: room for improvement? Eur J Cardiothorac Surg. 2009;35(6):953–7. discussion 7.
Noyez L, de Jager MJ, Markou AL. Quality of life after cardiac surgery: underresearched research. Interact Cardiovasc Thorac Surg. 2011;13(5):511–5.
van Geldorp MWA, Heuvelman HJ, Kappetein AP, et al. Quality of life among patients with severe aortic stenosis. Neth Heart J. 2013;21. doi:10.1007/s12471-012-0364-9.
Lindsay GM, Hanlon P, Smith LN, et al. Assessment of changes in general health status using the short-form 36 questionnaire 1 year following coronary artery bypass grafting. Eur J Cardiothorac Surg. 2000;18(5):557–64.
Rumsfeld JS, Magid DJ, O’Brien M, et al. Changes in health-related quality of life following coronary artery bypass graft surgery. Ann Thorac Surg. 2001;72(6):2026–32.
Sedrakyan A, Vaccarino V, Paltiel AD, et al. Age does not limit quality of life improvement in cardiac valve surgery. J Am Coll Cardiol. 2003;42(7):1208–14.
Heuvelman HJ, van Geldorp MW, Kappetein AP, et al. Clinical course of patients diagnosed with severe aortic stenosis in the Rotterdam area: insights from the AVARIJN study. Neth Heart J. 2012. 10.1007/s12471-012-0309-3.
Ware Jr JE, Gandek B. Overview of the SF-36 Health Survey and the International Quality of Life Assessment (IQOLA) Project. J Clin Epidemiol. 1998;51(11):903–12.
Aaronson NK, Muller M, Cohen PD, et al. Translation, validation, and norming of the Dutch language version of the SF-36 Health Survey in community and chronic disease populations. J Clin Epidemiol. 1998;51(11):1055–68.
Ware Jr JE, Kosinski M, Bjorner JB, et al. User’s manual for the SF-36v2 TM health survey. 2nd ed. Lincoln: Quality Metric Incorporated; 2007.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale: Lawrence Erlbaum Associates; 1988.
Horstkotte D, Loogen F. The natural history of aortic valve stenosis. Eur Heart J. 1988;9(Suppl E):57–64.
Varadarajan P, Kapoor N, Bansal RC, et al. Clinical profile and natural history of 453 nonsurgically managed patients with severe aortic stenosis. Ann Thorac Surg. 2006;82(6):2111–5.
Sjogren J, Thulin LI. Quality of life in the very elderly after cardiac surgery: a comparison of SF-36 between long-term survivors and an age-matched population. Gerontology. 2004;50(6):407–10.
Sundt TM, Bailey MS, Moon MR, et al. Quality of life after aortic valve replacement at the age of >80 years. Circulation. 2000;102(19 Suppl 3):III70–4.
Florath I, Albert A, Rosendahl U, et al. Mid term outcome and quality of life after aortic valve replacement in elderly people: mechanical versus stentless biological valves. Heart. 2005;91(8):1023–9.
Baberg HT, Dirlich M, Laczkovics A, et al. Determinants of health-related quality of life after aortic valve replacement in six-month survivors of intervention. J Heart Valve Dis. 2004;13(6):914–20.
Lam BK, Hendry PJ. Patients over 80 years: quality of life after aortic valve replacement. Age Ageing. 2004;33(3):307–9.
Vicchio M, De Santo LS, Della Corte A, et al. Aortic valve replacement with 19-mm bileaflet prostheses in the elderly: left ventricular mass regression and quality of life. J Heart Valve Dis. 2008;17(2):216–21.
Acknowledgments
The authors would like to thank the patients, cardiologists, echo laboratory staff and secretaries of the following hospitals for their kind cooperation: Havenziekenhuis, Rotterdam; St. Franciscus Gasthuis, Rotterdam; IJsselland Hospital, Capelle aan den Ijssel; Vlietland Hospital, Vlaardingen; Albert Schweitzer Hospital, Dordrecht; Medisch Centrum Rijnmond Zuid, Rotterdam; and Erasmus University Medical Center, Rotterdam.
Disclosures
The authors have no disclosures to make.
Author information
Authors and Affiliations
Corresponding author
Additional information
The questions can be answered after the article has been published in print. You have to log in to: www.cvoi.nl.
Rights and permissions
About this article
Cite this article
van Geldorp, M.W.A., Heuvelman, H.J., Kappetein, A.P. et al. The effect of aortic valve replacement on quality of life in symptomatic patients with severe aortic stenosis. Neth Heart J 21, 28–35 (2013). https://doi.org/10.1007/s12471-012-0362-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12471-012-0362-y